Tesamorelin is one of the very few research peptides that has crossed the line from experimental compound to a fully FDA-approved medicine — a distinction that makes it unusually valuable for understanding what a growth-hormone-releasing hormone (GHRH) analog can and cannot do. This article answers the core question, what is tesamorelin and how does it work, by tracing its molecular identity, its receptor-level mechanism, and the human clinical evidence base that earned it approval as Egrifta for HIV-associated lipodystrophy. Throughout, evidence is labeled by strength: what is proven in randomized human trials, what remains exploratory, and what is simply unknown.
What is tesamorelin?
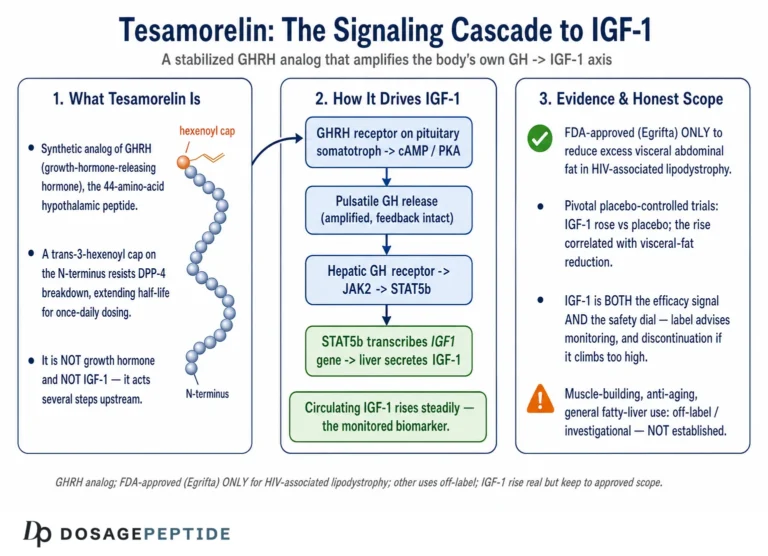
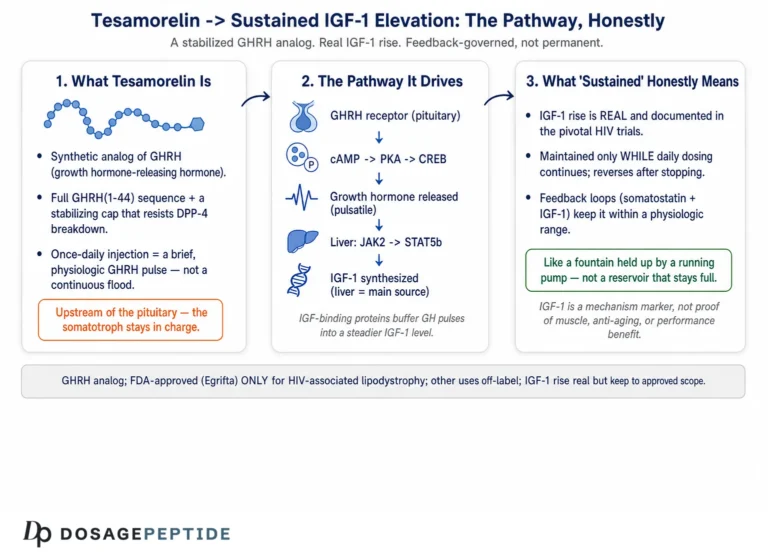
Tesamorelin is a synthetic, stabilized analog of human growth-hormone-releasing hormone (GHRH). Unlike the many peptides in the research space that mimic only a fragment of GHRH, tesamorelin reproduces the entire 44-amino-acid sequence of endogenous human GHRH (hGHRH[1–44]NH₂) and adds a single chemical modification that dramatically extends its stability.[1] That modification is a trans-3-hexenoic acid group (a short six-carbon fatty-acid chain containing a double bond) conjugated to the alpha-amino group of the N-terminal tyrosine residue. The result is a molecule that behaves like natural GHRH at the receptor but resists the enzymatic degradation that inactivates the native hormone within minutes.
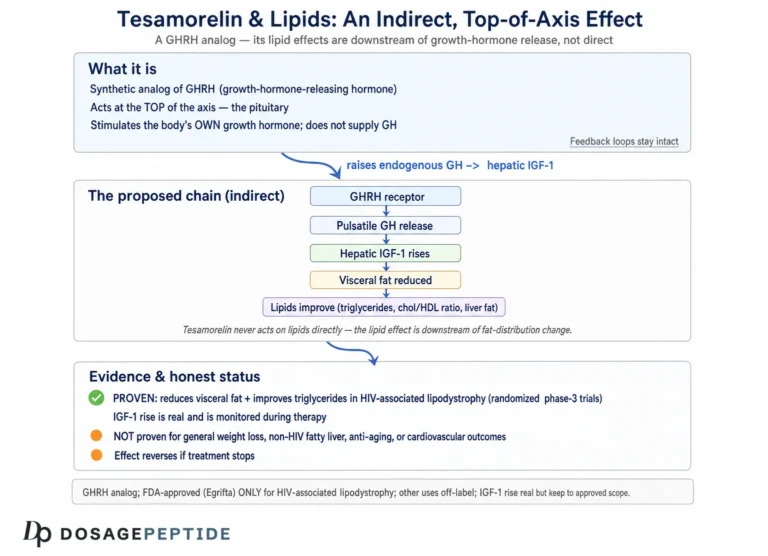
Because it is a GHRH analog rather than a direct growth hormone (GH) product, tesamorelin does not supply GH from the outside. Instead, it prompts the body’s own pituitary gland to secrete GH in its natural, pulsatile rhythm. This is a mechanistically important distinction from recombinant human growth hormone (rhGH), and it is central to both the compound’s therapeutic rationale and its comparatively favorable metabolic profile in trials.
The problem tesamorelin was designed to solve
To understand why tesamorelin exists, it helps to understand the clinical problem it was engineered for. In the era of combination antiretroviral therapy for HIV, a subset of treated patients developed lipodystrophy — an abnormal redistribution of body fat characterized by accumulation of deep visceral (intra-abdominal) fat, sometimes with loss of subcutaneous fat in the face and limbs. This excess visceral adipose tissue is not merely cosmetic: it is metabolically active tissue linked to dyslipidemia, insulin resistance, systemic inflammation, and elevated cardiovascular risk. Many of these patients also show a blunted growth-hormone axis, with reduced GH secretion that correlates with the degree of visceral fat accumulation.
The therapeutic logic was therefore elegant: rather than administer growth hormone directly — which carries a substantial burden of side effects, particularly insulin resistance and fluid retention, at the doses needed — restore the patient’s own GH pulses by stimulating the pituitary upstream with a stabilized GHRH analog. If the blunted GH axis could be reactivated within physiologic bounds, the visceral fat might be mobilized while the body’s intrinsic feedback loops limited the metabolic downside. Tesamorelin was developed to test exactly that hypothesis, and the pivotal trials described later confirmed it worked.
The GH–IGF-1 axis in brief
Tesamorelin sits at the top of a well-mapped endocrine cascade known as the somatotropic or GH–IGF-1 axis. The hypothalamus releases GHRH (stimulatory) and somatostatin (inhibitory) in a coordinated rhythm that governs how the anterior pituitary secretes growth hormone. GH is released in discrete bursts — largest during slow-wave sleep — and travels to the liver and peripheral tissues. In the liver, GH stimulates production of IGF-1, which mediates many of GH’s anabolic and metabolic effects and also feeds back on the hypothalamus and pituitary to restrain further GH release. This negative feedback is what keeps the system self-limiting. Age, obesity, chronic illness, and visceral adiposity all tend to blunt GH secretion, which is precisely the deficit tesamorelin is designed to counteract by acting at the GHRH-receptor level rather than bypassing the axis. Because tesamorelin engages this feedback-regulated system rather than flooding the body with exogenous hormone, IGF-1 elevations in trials generally stayed within or near the physiologic reference range.
Identity and pharmacology at a glance
The table below summarizes tesamorelin’s core physicochemical and pharmacologic properties as reported in the regulatory and pharmacology literature. Molecular weight and half-life figures reflect commonly cited values; the double-digit-minute half-life is the pharmacokinetic feature that most distinguishes it from native GHRH, whose circulating half-life is only a few minutes.
| Property | Tesamorelin |
|---|---|
| Class | Stabilized GHRH (GHRF) analog / growth hormone secretagogue |
| Peptide backbone | Full 44-amino-acid human GHRH sequence (hGHRH[1–44]NH₂) |
| Chemical modification | trans-3-hexenoic acid on N-terminal Tyr (alpha-amino group) |
| Approximate molecular weight | ~5,136 Da (free-base peptide) |
| Circulating half-life | Approximately 26–38 minutes (SC/IV in adults) |
| Molecular target | GHRH receptor (GHRHR) on pituitary somatotrophs |
| Downstream signal | Endogenous pulsatile GH → hepatic IGF-1 |
| Approved brand names | Egrifta, Egrifta SV, Egrifta WR (tesamorelin for injection) |
| Approved route/dose | 2 mg subcutaneous, once daily |
For readers who want a plain-language reference for the terms used here — somatotroph, IGF-1, GHRH receptor, pulsatile secretion — the peptide research glossary defines each concept in context.
How does tesamorelin work at the receptor level?
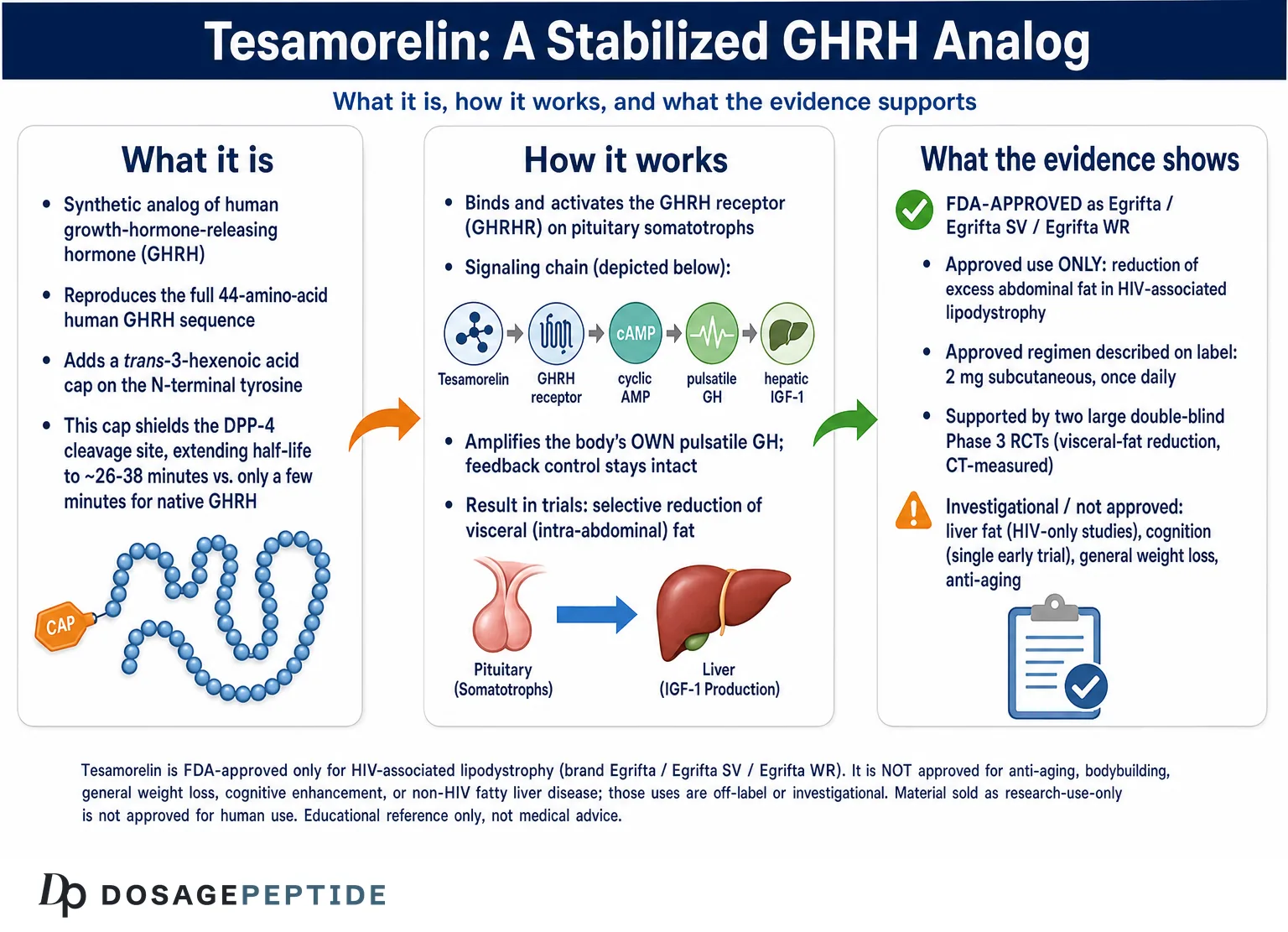
Tesamorelin works by binding and activating the GHRH receptor (GHRHR), a class B G-protein-coupled receptor expressed densely on the somatotroph cells of the anterior pituitary gland. When GHRH — or its analog tesamorelin — occupies this receptor, it activates a Gαs subunit, stimulates adenylate cyclase, and raises intracellular cyclic AMP. The rise in cAMP triggers synthesis and pulsatile release of growth hormone into the bloodstream.[1]
Once released, GH acts on multiple tissues directly, but a large fraction of its physiologic effect is mediated indirectly through insulin-like growth factor 1 (IGF-1), produced mainly in the liver in response to GH. IGF-1 is the principal circulating biomarker of GH-axis activity, and its measurement is central to both dosing safety and research monitoring of tesamorelin. In effect, the signaling chain is: tesamorelin → GHRH receptor → cAMP → pulsatile GH → hepatic IGF-1 → peripheral tissue effects.
At the molecular level, the GHRH receptor belongs to the secretin-like (class B) family of G-protein-coupled receptors. Agonist binding drives a conformational change that couples the receptor to the stimulatory G-protein Gαs, activating adenylate cyclase and elevating cyclic AMP. Cyclic AMP activates protein kinase A, which phosphorylates the transcription factor CREB and promotes transcription of the growth hormone gene, while also mobilizing intracellular calcium to trigger exocytosis of stored GH secretory granules. The net effect is both acute (release of pre-formed GH) and sustained (increased GH synthesis), which is why chronic GHRH-analog exposure raises the amplitude of GH pulses rather than simply causing a single spike. Tesamorelin occupies this receptor with the same functional agonism as native GHRH; its engineered advantage is not a different receptor interaction but a longer residence time in circulation.
Why visceral fat responds preferentially
A recurring question is why tesamorelin selectively reduces visceral adipose tissue rather than causing generalized fat loss. The leading explanation lies in the lipolytic action of growth hormone. GH promotes lipolysis — the breakdown of stored triglycerides into free fatty acids — and visceral fat is more metabolically active and more sensitive to lipolytic signaling than subcutaneous fat, with a higher density of relevant receptors and greater lipolytic responsiveness. When endogenous GH pulses are amplified, the visceral depot is mobilized preferentially. This selectivity is clinically desirable in lipodystrophy, where the goal is to shrink the harmful intra-abdominal depot without stripping protective subcutaneous fat, and it was demonstrated directly by CT imaging in the pivotal trials, which measured the two compartments separately.
Why the trans-3-hexenoic acid modification matters
Native human GHRH is rapidly cleaved by the enzyme dipeptidyl peptidase-4 (DPP-4), which removes amino acids from the N-terminus and inactivates the hormone almost immediately. The trans-3-hexenoic acid cap on tesamorelin’s N-terminal tyrosine sterically shields the DPP-4 cleavage site, slowing degradation and extending the functional half-life several-fold relative to unmodified GHRH.[1] This is a targeted stability engineering strategy: the peptide retains full GHRH-like receptor activity while gaining enough circulating time to drive a robust GH pulse.
Preserving pulsatility — the key physiologic advantage
A defining feature of GHRH-analog therapy is that it amplifies the body’s own GH secretion rather than replacing it. Endogenous GH is normally released in discrete pulses, chiefly overnight, under layered feedback control from somatostatin and IGF-1. Because tesamorelin acts upstream at the pituitary, it preserves this pulsatile pattern and leaves the negative-feedback loop intact — if IGF-1 climbs too high, somatostatin tone and feedback tend to blunt further GH release. This is mechanistically different from administering rhGH, which delivers continuous, non-physiologic GH exposure. Preserved feedback is the leading explanation for why tesamorelin’s trials generally showed more favorable glucose behavior than would be expected from equivalent rhGH dosing, although GH-axis stimulation still carries measurable metabolic effects discussed later.
Is tesamorelin FDA-approved?
Yes. Tesamorelin is FDA-approved, which places it in a small minority of research-associated peptides with genuine regulatory standing. It was first approved in the United States in 2010 under the brand name Egrifta for the reduction of excess abdominal fat in HIV-infected adult patients with lipodystrophy.[1] The approved label language describes it as a growth-hormone-releasing factor (GHRF) analog indicated specifically for that population, at a dose of 2 mg by subcutaneous injection once daily.[2]
The formulation has since been refined. A more concentrated version, Egrifta SV (the F4 formulation), simplified daily reconstitution. In March 2025 the FDA approved Egrifta WR (the F8 formulation of tesamorelin), which requires only weekly reconstitution and less than half the injection volume of the earlier product while still being administered daily — a convenience and adherence improvement, not a new indication.[3] Across all three formulations, the single approved indication remains HIV-associated lipodystrophy.
What tesamorelin is not approved for
It is important to state the regulatory boundaries plainly. Tesamorelin is not FDA-approved for general anti-aging, bodybuilding, cognitive enhancement, weight loss in the general population, or non-HIV fatty liver disease. Uses outside HIV-associated lipodystrophy are off-label or investigational. Material sold as “research-use-only” tesamorelin is not manufactured, labeled, or quality-controlled as an approved drug and is not intended for human administration. Every dosing figure discussed in this article reflects controlled clinical research or the approved label; none is presented as guidance for personal use.
What does the human clinical evidence show?
Tesamorelin is unusual among research peptides in having a substantial base of randomized, double-blind, placebo-controlled human trials — the highest tier of clinical evidence. Its evidence base is strongest and clearest for its approved indication, and progressively more exploratory the further one moves from HIV-associated visceral fat.
The pivotal Phase 3 trial — Falutz et al., NEJM 2007
The registrational cornerstone is the multicenter Phase 3 trial led by Julian Falutz and colleagues, published in the New England Journal of Medicine in 2007. This double-blind, placebo-controlled study randomized HIV-infected patients with abdominal fat accumulation to 2 mg of tesamorelin or placebo subcutaneously daily. The primary endpoint was the change in visceral adipose tissue (VAT) measured by CT scan over 26 weeks.[4]
The trial met its endpoint decisively: tesamorelin produced a significant, selective reduction in visceral fat — on the order of a 15% decrease versus an increase in the placebo group — alongside improvements in triglycerides and other lipid measures, and without significant deterioration in glycemic control over the initial treatment period.[4] The reduction was notably selective for the metabolically active visceral compartment rather than subcutaneous fat, which is the therapeutic goal in lipodystrophy.
Several design features make this trial particularly credible. It used an objective, quantitative imaging endpoint (CT-measured visceral adipose tissue) rather than subjective assessment or crude anthropometry, minimizing measurement bias. It was double-blind and placebo-controlled, the gold-standard design for isolating a drug effect from placebo response and natural variation. And it was adequately powered and multicenter, reducing the chance that results reflected a single-site anomaly. The 26-week primary phase was followed by a 26-week extension in which patients originally on tesamorelin either continued or switched to placebo, allowing investigators to study what happens when treatment is maintained versus withdrawn. A key lesson from the extension design across the tesamorelin program is that the visceral-fat benefit depends on continued treatment: the depot tends to re-accumulate after the drug is stopped, indicating the effect is a maintained physiologic state rather than a permanent structural remodeling.
The confirmatory Phase 3 trial — 404 patients
A second, confirmatory 26-week Phase 3 trial reinforced these findings in an independent cohort of 404 randomized HIV patients with excess abdominal fat, again showing selective visceral-fat reduction with 2 mg daily tesamorelin.[5] Pooled across the two pivotal trials, roughly 800 patients contributed to the efficacy and safety dataset that underpinned the FDA approval — a genuinely large, replicated evidence base by peptide-research standards. Follow-up analyses of the pooled population reported that the visceral-fat reduction was associated with an improved metabolic profile, including favorable changes in triglycerides.[6]
| Study | Design | Population | Key finding | Evidence level |
|---|---|---|---|---|
| Falutz et al., NEJM 2007[4] | RCT, double-blind, 26 wk | HIV lipodystrophy | Selective ~15% VAT reduction; improved lipids | Human RCT (pivotal) |
| Confirmatory Phase 3, 2008[5] | RCT, 26 wk, 404 pts | HIV abdominal fat | Replicated selective VAT reduction | Human RCT (confirmatory) |
| Stanley et al., JAMA 2014[7] | RCT, 6 mo, 50 pts | HIV + abdominal fat | ~37% relative liver-fat reduction; VAT reduction | Human RCT (mechanistic) |
| NAFLD trial, Lancet HIV 2019[8] | RCT, multicenter | HIV + NAFLD | Reduced liver fat; less fibrosis progression | Human RCT (exploratory indication) |
| Baker et al., Arch Neurol 2012[9] | RCT, 20 wk, 152 adults | MCI + healthy older adults | Improved executive function; IGF-1 ↑ | Human RCT (early cognition signal) |
| T2DM safety trial, PLOS One 2017[10] | RCT, 12 wk, 53 pts | Type 2 diabetes | No significant worsening of HbA1c/glucose control | Human RCT (safety) |
Liver fat and NAFLD — a growing but still HIV-focused evidence line
Beyond visceral fat, tesamorelin has been studied for its effect on liver fat. A mechanistic randomized trial by Stanley and colleagues, published in JAMA in 2014, enrolled 50 antiretroviral-treated HIV patients with abdominal fat accumulation and randomized them to 2 mg daily tesamorelin or placebo for six months. Tesamorelin reduced hepatic fat fraction with an absolute effect of about −4.1% and a relative reduction of roughly −37% versus placebo (P=0.02), while also lowering visceral fat.[7]
A later multicenter randomized trial published in The Lancet HIV in 2019 examined tesamorelin specifically in HIV patients with non-alcoholic fatty liver disease (NAFLD), reporting reductions in liver fat and a lower rate of fibrosis progression compared with placebo.[8] These are important, methodologically strong findings — but note the crucial caveat: they were all conducted in HIV-positive populations. Tesamorelin is not approved for NAFLD, and its benefit in the general (non-HIV) NAFLD population has not been established to the same standard.
The liver-fat work is scientifically interesting because it suggests the visceral-fat and hepatic-fat effects share a mechanism: mobilizing ectopic fat from metabolically active depots. Fatty liver in this population is closely tied to the same visceral adiposity and insulin-resistance biology that tesamorelin targets, so a reduction in hepatic fat is mechanistically coherent with the drug’s primary action. The Lancet HIV trial went further than fat quantification alone by evaluating fibrosis, an important distinction because reducing fat content is not the same as preventing progression of liver disease. The reported reduction in fibrosis progression is therefore a meaningful signal — but it is a signal within the HIV-NAFLD niche, not a demonstrated treatment for the far larger population of people with metabolic-associated fatty liver disease unrelated to HIV. Extrapolating these results beyond the studied population would over-state what the evidence supports.
Distinguishing evidence tiers
Because tesamorelin is marketed and discussed in contexts far beyond its approval, it is worth being explicit about the hierarchy of its evidence. In descending order of strength: (1) two large, replicated, double-blind Phase 3 RCTs for visceral-fat reduction in HIV lipodystrophy — this is approval-grade evidence; (2) mechanistic RCTs with objective imaging endpoints for liver fat in HIV — strong but indication-specific; (3) a single 20-week cognition RCT in older adults — a genuine but unreplicated early signal; and (4) short safety RCTs in metabolically vulnerable groups. Notably, there is essentially no high-quality randomized evidence for the popular but off-label uses — general anti-aging, athletic body-recomposition, or fat loss in healthy adults — and any claims in those areas rest on extrapolation from mechanism, not on direct trials.
Cognition and healthy aging — a genuine but early signal
One of the most-cited exploratory findings comes from a randomized, double-blind, placebo-controlled trial by Baker and colleagues, published in Archives of Neurology in 2012. It enrolled 152 older adults — some with mild cognitive impairment (MCI) and some cognitively normal — and gave 1 mg tesamorelin or placebo subcutaneously at bedtime for 20 weeks. The treated group showed improvements in executive function and verbal memory, and IGF-1 rose substantially while remaining within the physiologic range.[9]
This is a real, well-designed trial, and it is frequently invoked to justify “nootropic” use of GHRH analogs. It should be read with discipline: it was a single, relatively short study using cognitive-test endpoints (not clinical dementia outcomes), it has not driven any regulatory approval for cognition, and it does not establish that tesamorelin prevents or treats dementia. It is best characterized as a promising early signal that warrants larger, longer confirmatory trials — not as proven cognitive therapy.
Safety in metabolically vulnerable populations
Because GH stimulation can theoretically worsen glucose handling, a dedicated 12-week randomized, placebo-controlled trial published in PLOS One in 2017 tested tesamorelin (1 mg and 2 mg) against placebo in 53 patients with type 2 diabetes. Over the treatment period, there were no significant between-group differences in insulin sensitivity, fasting glucose, or HbA1c, and the 2 mg group actually showed modest reductions in total and non-HDL cholesterol.[10] This does not eliminate the glucose-related cautions on the label — it was a short study — but it is reassuring human data in a group where GH-axis stimulation is most concerning.
What are the documented benefits of tesamorelin?
Benefits below are ranked by evidence strength. The first is an approved, replicated indication; the rest range from strong mechanistic data to early exploratory signals.
- Selective visceral fat reduction (proven, approved). The core, FDA-recognized effect: preferential loss of metabolically dangerous visceral adipose tissue in HIV-associated lipodystrophy, demonstrated in two pivotal RCTs.[4]
- Improved lipid profile (strong). Reductions in triglycerides and improvements in other lipids accompanied visceral-fat loss in the pivotal and pooled analyses.[6]
- Reduced liver fat (strong, HIV-specific). Randomized data show meaningful hepatic-fat reduction and less fibrosis progression in HIV patients.[7]
- Restored IGF-1 within physiologic range (mechanistic). Tesamorelin raises IGF-1 by stimulating endogenous GH, reflecting reactivation of a GH axis often blunted with age or illness.[9]
- Early cognitive signal (exploratory). One RCT showed executive-function and verbal-memory gains in older adults — promising but unconfirmed and non-approved.[9]
A frequent misconception is that these results generalize to healthy adults seeking body-recomposition or anti-aging effects. They do not automatically transfer: the pivotal evidence comes from a specific patient population (HIV lipodystrophy) in whom visceral fat and GH-axis biology differ from the general population. Honest interpretation keeps the approved benefit and the exploratory signals in separate mental buckets.
It is also worth noting what tesamorelin does not reliably do, based on the trial record. It is not a weight-loss drug in the conventional sense: because it selectively mobilizes visceral fat and can promote fluid retention and lean tissue changes, total body-weight change on the scale is not the meaningful endpoint — visceral fat area and metabolic markers are. It does not produce the dramatic total-fat reductions associated with modern GLP-1 receptor agonists, and it targets a different problem (ectopic visceral fat and GH-axis deficit) through a different mechanism. Framing tesamorelin as a general obesity treatment misrepresents both its approved use and its measured effects; its documented value is specific, mechanism-driven, and population-defined.
What are the side effects and safety signals?
The approved label and trial record give an unusually detailed safety picture. The most common adverse reactions (occurring in at least 5% of patients) reported on the tesamorelin label are shown below, with the approved-product percentages versus placebo.[2]
| Adverse reaction | Tesamorelin | Placebo |
|---|---|---|
| Injection-site reactions (erythema, pruritus, pain) | 17% | 6% |
| Arthralgia (joint pain) | 13% | 11% |
| Pain in extremity | 6% | 5% |
| Peripheral edema (fluid retention) | 6% | 2% |
| Myalgia (muscle pain) | 6% | 2% |
Injection-site reactions
The most frequent adverse effect is local reaction at the injection site — redness, itching, or discomfort. The majority of these reactions in trials were mild (Grade 1) and self-limited. Rotating injection sites is the standard mitigation described in the product information.[2]
IGF-1 elevation and theoretical neoplasm risk
Because tesamorelin’s entire mechanism is to raise GH and therefore IGF-1, a labeled warning centers on the theoretical concern that elevated IGF-1 could promote growth of pre-existing malignancy. The label directs that IGF-1 be monitored and that treatment be reconsidered if IGF-1 rises persistently above the normal reference range. Active malignancy is a formal contraindication.[2] In the pivotal trials, IGF-1 rose meaningfully but no specific malignancy signal was attributed to treatment over the studied timeframe; the caution is precautionary and reflects GH-axis physiology.
Glucose and insulin effects
Growth hormone is a counter-regulatory (insulin-antagonizing) hormone, so any GH-raising agent warrants attention to glucose. The pivotal trials did not show clinically significant worsening of fasting glucose or HbA1c over 26 weeks, and the dedicated type 2 diabetes trial found no significant deterioration in diabetes control over 12 weeks.[10] Nonetheless, the label advises evaluating glucose status before starting and monitoring periodically, because glucose intolerance remains a listed warning and individual responses vary.[11]
The relatively benign glucose profile observed in trials is one of the most instructive findings about tesamorelin, and it traces back to mechanism. Because the peptide amplifies the body’s own pulsatile GH secretion within a feedback-regulated system rather than delivering continuous supraphysiologic GH, the glucose-antagonizing effect appears more modest than what is typically seen with exogenous rhGH at comparable biological intensity. This is a genuine mechanistic advantage — but it is not a guarantee of glucose neutrality for any individual, and the studied durations were measured in months, not years. Longer-term glucose safety, particularly in people with pre-existing insulin resistance, remains an area where the data are reassuring but not exhaustive.
Recommended monitoring in the approved setting
In the approved clinical context, the label frames a monitoring program that reflects the drug’s biology: baseline and periodic IGF-1 measurement to detect excessive GH-axis stimulation; assessment of glucose status before and during treatment; and clinical attention to fluid retention and to any new or changing symptoms that could signal neoplasm in at-risk patients. Treatment is meant to be reassessed if IGF-1 rises persistently above the reference range, and discontinued if a contraindication such as active malignancy or pregnancy arises. This structured monitoring is a defining feature of tesamorelin used as an approved medicine — and it is precisely the safety scaffolding that is absent when unregulated “research-use” material is used outside a clinical setting.
Fluid retention and musculoskeletal effects
Peripheral edema, arthralgia, and myalgia are consistent with a GH-mediated mechanism (GH promotes sodium and fluid retention and can cause joint and muscle symptoms). These effects were generally mild-to-moderate in trials and are dose- and IGF-1-related in the broader GH literature.[1]
Contraindications
The approved label lists four clear contraindications: disruption of the hypothalamic-pituitary axis (e.g., from hypophysectomy, hypopituitarism, or head irradiation); active malignancy; known hypersensitivity to tesamorelin or any of its excipients; and pregnancy.[2] Regarding liver safety specifically, the LiverTox monograph assigns tesamorelin a likelihood score indicating it is an unlikely cause of clinically apparent liver injury, with no confirmed cases of drug-induced hepatotoxicity reported.[1]
How does tesamorelin compare to sermorelin, CJC-1295, and ipamorelin?
Tesamorelin is often grouped with other GH-axis peptides, but there are important mechanistic and regulatory distinctions. Sermorelin, CJC-1295, and tesamorelin are all GHRH analogs that act on the GHRH receptor; ipamorelin is different — it is a growth hormone secretagogue that acts on the ghrelin receptor (GHS-R1a), a separate pathway. The most consequential difference, however, is regulatory: tesamorelin and sermorelin have FDA approvals for defined indications, whereas CJC-1295 and ipamorelin are not FDA-approved for any human therapeutic use.
| Peptide | Class / target | Structure | Approx. half-life | FDA status |
|---|---|---|---|---|
| Tesamorelin | GHRH analog / GHRHR | Full GHRH(1–44) + hexenoic acid cap | ~26–38 min | Approved (HIV lipodystrophy) |
| Sermorelin | GHRH analog / GHRHR | GHRH(1–29) fragment | ~10–20 min | Previously approved (pediatric GH deficiency); brand withdrawn |
| CJC-1295 (no DAC) | GHRH analog / GHRHR | Modified GRF(1–29) | ~30+ min | Not FDA-approved |
| CJC-1295 (with DAC) | GHRH analog / GHRHR | GRF(1–29) + albumin-binding DAC | Days (long-acting) | Not FDA-approved |
| Ipamorelin | GH secretagogue / ghrelin receptor (GHS-R1a) | Pentapeptide | ~2 hours | Not FDA-approved |
Interpreting the comparison honestly
A common marketing claim is that these peptides are interchangeable “GH boosters.” The evidence does not support treating them as equivalent. Tesamorelin is the only compound in this group with two large replicated Phase 3 trials and an FDA-approved indication built on hard imaging endpoints (CT-measured visceral fat). Sermorelin has a long historical safety record but its clinical data concentrate on pediatric GH deficiency. CJC-1295 and ipamorelin are supported mainly by pharmacology and small studies, not by large registrational trials, and their long-term human safety is not characterized to the same standard. When evidence strength — not just mechanism — is the yardstick, tesamorelin stands apart.
GHRH analogs versus ghrelin-receptor secretagogues
The mechanistic split within this group deserves emphasis because it is frequently blurred in popular sources. GHRH analogs (tesamorelin, sermorelin, CJC-1295) and ghrelin-receptor agonists (ipamorelin, and the GHRP family more broadly) stimulate GH through two distinct receptors that can act complementarily. GHRH analogs act on the GHRH receptor to raise the amplitude of GH pulses; ghrelin-receptor secretagogues act on GHS-R1a to both stimulate GH release and blunt somatostatin’s inhibitory tone. This is the rationale behind popular “GHRH + secretagogue” pairings in the research space: activating both pathways can produce a larger GH response than either alone. It is important to stress, however, that combination approaches are studied far less rigorously than tesamorelin monotherapy, that they are not FDA-approved, and that stacking amplifies not only the GH signal but also the theoretical IGF-1-related and glucose-related concerns discussed above — without the monitoring framework that accompanies approved use.
What sets tesamorelin’s structure apart
Structurally, tesamorelin is distinguished from the other GHRH analogs by using the full 44-amino-acid GHRH sequence rather than the truncated 1–29 fragment that sermorelin and CJC-1295 (modified GRF 1–29) are based on. The 1–29 fragment retains the minimum region needed for receptor activation, which is why those shorter analogs are functional; tesamorelin’s use of the complete sequence, combined with its trans-3-hexenoic-acid stabilization, produces its specific pharmacokinetic and receptor-engagement profile. CJC-1295 “with DAC” takes a different stabilization route entirely, adding a drug-affinity-complex that binds serum albumin to extend half-life to a matter of days — a fundamentally different pharmacology that trades tesamorelin’s short, pulsatile-preserving action for prolonged, non-pulsatile receptor exposure. These are not trivial distinctions: the shape of the GH signal over time (pulsatile versus continuous) is itself thought to influence downstream effects and tolerability.
How is tesamorelin studied and handled in research settings?
Tesamorelin is supplied as a lyophilized (freeze-dried) powder that must be reconstituted with a sterile diluent before use. In research and clinical settings the handling principles mirror those of other peptide products: careful reconstitution technique, cold-chain storage, and attention to stability after mixing.
Reconstitution and stability principles
Lyophilized peptides are hygroscopic and sensitive to heat, agitation, and repeated freeze-thaw cycles. Reconstitution is typically performed by adding diluent slowly against the vial wall rather than directly onto the powder, and by swirling rather than vigorously shaking, to avoid shearing the peptide. Once reconstituted, tesamorelin has limited stability and is generally kept refrigerated and protected from light. General best practices are described in the peptide reconstitution guide, and storage-specific considerations for reconstituted tesamorelin are covered in the dedicated tesamorelin storage guidance.
Tesamorelin’s handling requirements are one reason its pharmaceutical formulation has been iteratively improved. The original approved product required daily reconstitution, which imposed a meaningful daily burden. The F4 formulation (Egrifta SV) concentrated the product to simplify that step, and the F8 formulation (Egrifta WR, approved in 2025) went further: it is reconstituted only once per week yet still administered daily, and uses less than half the injection volume of the earlier product.[3] This formulation history is a useful reminder that peptide stability after reconstitution is a real, engineerable property — and that the reconstitution and storage practices which matter in a research setting are the same variables the manufacturer had to solve to make the drug practical.
Concentration and volume calculations
Because tesamorelin vials come in different masses (commonly discussed as 5 mg and 10 mg presentations) and diluent volumes vary, the delivered concentration per unit volume depends entirely on how the vial is reconstituted. Getting this arithmetic right is a core research-handling skill; a reconstitution and dosage calculator can convert a target amount into a syringe volume for a given vial size and diluent quantity. For worked, vial-specific reference walkthroughs, see the tesamorelin 10 mg vial protocol and the companion tesamorelin 5 mg vial protocol.
For reference — and strictly as a description of the studied regimen, not as advice — the dose used throughout tesamorelin’s pivotal trials and reflected on the approved label is 2 mg administered by subcutaneous injection once daily.[2] The cognition study used a lower 1 mg dose at bedtime, chosen to align GH stimulation with the natural nocturnal secretory pattern.[9] These figures illustrate how the studied amount, timing, and route were deliberately matched to the mechanism and endpoint of each trial; they are context for interpreting the literature, not a template for personal use, which sits outside the scope of this educational reference.
Research models and measurement methods
The human trials that define tesamorelin’s profile relied on rigorous quantitative endpoints rather than subjective report. Visceral adipose tissue was measured by cross-sectional CT imaging at the L4–L5 level; liver fat was quantified with proton magnetic resonance spectroscopy (1H-MRS) to derive hepatic fat fraction; and GH-axis engagement was tracked through serum IGF-1 assays. Cognitive studies used standardized neuropsychological batteries assessing executive function and memory. These objective imaging and biomarker methods are a major reason tesamorelin’s data are considered robust: fat compartments and liver fat were measured directly, not inferred.
The choice of endpoints is worth dwelling on, because it separates tesamorelin’s evidence from the anecdote-heavy literature surrounding many research peptides. Cross-sectional CT at a defined anatomical landmark yields a reproducible, operator-independent measurement of the visceral fat area in square centimeters — a hard number that can be compared across time and between arms. Proton MRS is a validated, non-invasive method for quantifying intrahepatic lipid content, allowing the NAFLD and liver-fat studies to report percentage changes in hepatic fat fraction rather than relying on surrogate blood markers alone. IGF-1 assays provide a pharmacodynamic readout confirming that the drug actually engaged its intended axis, which is essential for interpreting whether a null or positive clinical result reflects the mechanism or a failure of target engagement. In the NAFLD work, some studies additionally incorporated histology or non-invasive fibrosis assessment, moving beyond fat quantity toward disease-relevant tissue outcomes. Collectively, this methodological rigor is why regulators and clinicians treat tesamorelin’s core claims as established rather than provisional.
What the models can and cannot tell us
Even strong methods carry interpretive limits. The trial populations were defined by HIV-associated lipodystrophy, so the biology being measured — blunted GH axis, visceral fat expansion driven partly by antiretroviral and disease factors — is not identical to the biology of an otherwise healthy adult. A CT-verified visceral-fat reduction in that population is genuinely proven for that population; it is an inference, not a proof, that the same magnitude of effect would occur elsewhere. Likewise, cognitive-battery improvements over 20 weeks are a legitimate signal of a drug effect on measured cognitive tasks, but they cannot, by study design, speak to whether long-term dementia risk is altered. Reading the models honestly means crediting them fully for what they measured and declining to stretch them past their design.
What are the limitations and open questions?
An honest reference must be as clear about what is unknown as about what is proven.
- Population specificity. The strongest data derive from HIV-associated lipodystrophy. Whether the visceral-fat and liver-fat benefits translate with the same magnitude to non-HIV populations is not established by equivalent Phase 3 evidence.
- Durability and rebound. Visceral fat tends to re-accumulate after tesamorelin is stopped, indicating the effect is maintained by ongoing treatment rather than being a permanent structural change.
- Long-term neoplasm safety. Because the mechanism raises IGF-1, long-horizon cancer-risk data would be reassuring but are inherently difficult to generate; the current position is precautionary monitoring, not a demonstrated harm.
- Cognition remains a single-signal question. The 2012 cognitive trial is encouraging but unreplicated at scale and did not measure clinical dementia outcomes.
- Non-approved uses lack a safety framework. Any use outside the approved HIV indication — anti-aging, athletic, general metabolic — sits outside the evidence base and outside labeled monitoring.
- Product quality outside the regulated supply chain is unverified. Peptides sold as research chemicals vary in purity, identity, and endotoxin content; the clinical data described here were generated with pharmaceutical-grade tesamorelin and do not transfer to unverified material.
These open questions do not diminish what tesamorelin has proven; they define the frontier of what is still unknown. The compound occupies an unusual middle ground: far better validated than the typical research peptide, yet far narrower in its established scope than the broad claims often attached to it. A responsible reading credits the two pivotal trials and the mechanistic imaging studies as genuine, high-quality science while treating cognition, general NAFLD, and anti-aging applications as hypotheses awaiting the same caliber of evidence. The gap between “mechanistically plausible” and “demonstrated in humans” is exactly where most overstatement about tesamorelin lives, and closing that gap requires trials that, for these off-label uses, have not yet been done.
What is the current regulatory status of tesamorelin?
As of mid-2026, tesamorelin remains FDA-approved solely for the reduction of excess abdominal fat in HIV-infected adults with lipodystrophy, available as Egrifta, Egrifta SV, and the newer Egrifta WR (F8) formulation approved in March 2025.[3] No new therapeutic indication (for cognition, general NAFLD, weight loss, or anti-aging) has been approved. Tesamorelin sold outside the approved pharmaceutical supply chain — including “research-use-only” material — is not an approved drug, is not quality-assured for human use, and is intended strictly for laboratory research. Nothing in this article should be read as encouragement to self-administer tesamorelin or as a substitute for professional medical advice.
Frequently Asked Questions
Is tesamorelin the same as growth hormone?
No. Tesamorelin does not contain growth hormone. It is a GHRH analog that binds the GHRH receptor on the pituitary and prompts the gland to release the body’s own growth hormone in a natural pulsatile pattern. This upstream mechanism preserves normal feedback control, which distinguishes it from injecting recombinant growth hormone directly and is thought to underlie its comparatively favorable glucose behavior in trials.
What is tesamorelin FDA-approved for?
Tesamorelin is FDA-approved only for the reduction of excess abdominal (visceral) fat in HIV-infected adults with lipodystrophy, first approved in 2010 as Egrifta and now also available as Egrifta SV and Egrifta WR. It is not approved for anti-aging, bodybuilding, general weight loss, cognitive enhancement, or non-HIV fatty liver disease. Any use outside the HIV indication is off-label or investigational.
How does tesamorelin reduce visceral fat?
By raising endogenous growth hormone and, in turn, IGF-1, tesamorelin promotes lipolysis (fat breakdown) that is preferential for the metabolically active visceral fat compartment. In two pivotal Phase 3 trials, 2 mg daily produced a selective reduction in CT-measured visceral adipose tissue — on the order of 15% — without a comparable loss of subcutaneous fat, which is why it is used specifically for lipodystrophy.
Does tesamorelin improve memory or cognition?
There is a genuine but early signal. A 2012 randomized trial in 152 older adults reported improved executive function and verbal memory over 20 weeks, alongside a rise in IGF-1 within the physiologic range. However, this was a single, relatively short study using cognitive-test endpoints rather than clinical dementia outcomes, it has not been confirmed in larger trials, and tesamorelin is not approved for any cognitive indication.
What are the most common side effects of tesamorelin?
The most frequent side effects reported in trials and on the label are injection-site reactions (redness, itching, pain), joint pain (arthralgia), muscle pain (myalgia), pain in the extremities, and peripheral edema from fluid retention. Most were mild-to-moderate. Because the drug raises IGF-1, the label also warns about theoretical neoplasm risk and glucose intolerance and advises periodic monitoring.
Does tesamorelin affect blood sugar?
Growth hormone antagonizes insulin, so glucose is monitored. In the pivotal 26-week trials and a dedicated 12-week study in type 2 diabetes, tesamorelin did not significantly worsen fasting glucose or HbA1c. Even so, the label lists glucose intolerance as a warning and recommends checking glucose status before starting and periodically during use, because individual responses can vary.
How is tesamorelin different from CJC-1295 and ipamorelin?
Tesamorelin and CJC-1295 are both GHRH analogs acting on the GHRH receptor, while ipamorelin works on a different pathway — the ghrelin receptor. The decisive difference is evidence and regulation: tesamorelin has two large Phase 3 trials and FDA approval, whereas CJC-1295 and ipamorelin are not FDA-approved and lack registrational human trials. They should not be treated as interchangeable.
Is research-use tesamorelin the same as prescription Egrifta?
No. Prescription Egrifta (and Egrifta SV/WR) is a regulated pharmaceutical manufactured and quality-controlled to FDA standards. Material sold as “research-use-only” tesamorelin is not approved for human administration, is not held to those manufacturing and purity standards, and is intended only for laboratory research. The clinical data described here apply to the approved product, not to unregulated research chemicals.
References
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury — Tesamorelin. National Institute of Diabetes and Digestive and Kidney Diseases. https://www.ncbi.nlm.nih.gov/books/NBK548730/
- EGRIFTA SV (tesamorelin) prescribing information (label). DailyMed, U.S. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=3d783378-b02d-4f19-99dd-0fc91a042224
- Contagion Live. FDA Approves F8 Formulation (EGRIFTA WR) of Theratechnologies’ Tesamorelin for HIV-Associated Lipodystrophy, March 2025. https://www.contagionlive.com/view/fda-approves-f8-formulation-of-theratechnologies-tesamorelin-for-hiv-associated-lipodystrophy
- Falutz J, et al. Metabolic Effects of a Growth Hormone–Releasing Factor in Patients with HIV. New England Journal of Medicine. 2007;357:2359–2370. https://www.nejm.org/doi/full/10.1056/NEJMoa072375
- Results from the 26-week Confirmatory Phase 3 Trial of Tesamorelin (TH9507) in HIV Patients with Excess Abdominal Fat: 404 Randomized Patients. NATAP (IAS 2008). https://natap.org/2008/IAS/IAS_56.htm
- Stanley TL, et al. Reduction in visceral adiposity is associated with an improved metabolic profile in HIV-infected patients receiving tesamorelin. PubMed 22495074. https://pubmed.ncbi.nlm.nih.gov/22495074/
- Stanley TL, et al. Effect of Tesamorelin on Visceral Fat and Liver Fat in HIV-Infected Patients with Abdominal Fat Accumulation: A Randomized Clinical Trial. JAMA. 2014;312(4):380–389. https://jamanetwork.com/journals/jama/fullarticle/1889139
- Effects of tesamorelin on non-alcoholic fatty liver disease in HIV: a randomised, double-blind, multicentre trial. The Lancet HIV. 2019. https://www.thelancet.com/journals/lanhiv/article/PIIS2352-3018(19)30338-8/abstract
- Baker LD, et al. Effects of Growth Hormone–Releasing Hormone on Cognitive Function in Adults with Mild Cognitive Impairment and Healthy Older Adults. Archives of Neurology. 2012. PMC3764914. https://pmc.ncbi.nlm.nih.gov/articles/PMC3764914/
- Clemmons DR, et al. Safety and metabolic effects of tesamorelin in patients with type 2 diabetes: A randomized, placebo-controlled trial. PLOS One. 2017. PMC5472315. https://pmc.ncbi.nlm.nih.gov/articles/PMC5472315/
- Tesamorelin Disease Interactions (professional). Drugs.com. https://www.drugs.com/disease-interactions/tesamorelin.html?professional=1