Few research peptides have attracted as much attention from athletes, biohackers, and injured weekend warriors as BPC-157, a synthetic 15-amino-acid sequence widely promoted for its supposed ability to accelerate the repair of tendons, ligaments, muscle, and bone. Search the internet and you will find confident testimonials, before-and-after stories, and clinics offering it as a shortcut around slow-healing soft-tissue injuries. Yet when you set aside the marketing and look at what has actually been demonstrated in peer-reviewed science, a very different and more sober picture emerges. The evidence supporting BPC-157 for musculoskeletal healing is real, but it is almost entirely preclinical: it comes from rats, mice, cell cultures, and tissue explants, not from adequately designed human trials.
This article walks through that evidence in detail and tries to be scrupulously honest about its level. We will look at where BPC-157 came from, the molecular pathways researchers believe it engages, the specific animal studies on tendon, muscle, ligament, and bone that anchor its reputation, and how a recent systematic review summarized the whole body of work. We will also confront the uncomfortable parts: the near-total absence of published human data, the concentration of the literature in a single research group, the manufacturing and immunogenicity concerns flagged by regulators, and the fact that BPC-157 is not approved by the FDA, the EMA, or any other national drug authority for any use.
Throughout, the framing is educational and research-oriented. BPC-157 is an investigational compound. Nothing here should be read as a recommendation to use it, and none of the outcomes described in animals can be assumed to translate to people. If you take one idea away, let it be this: an interesting mechanism and a stack of promising rodent studies are the beginning of a drug-development story, not the end of one. For grounding on how the compound is discussed in a research-dosing context, see the DosagePeptide BPC-157 dosage protocol reference.
What BPC-157 Is and Where It Came From
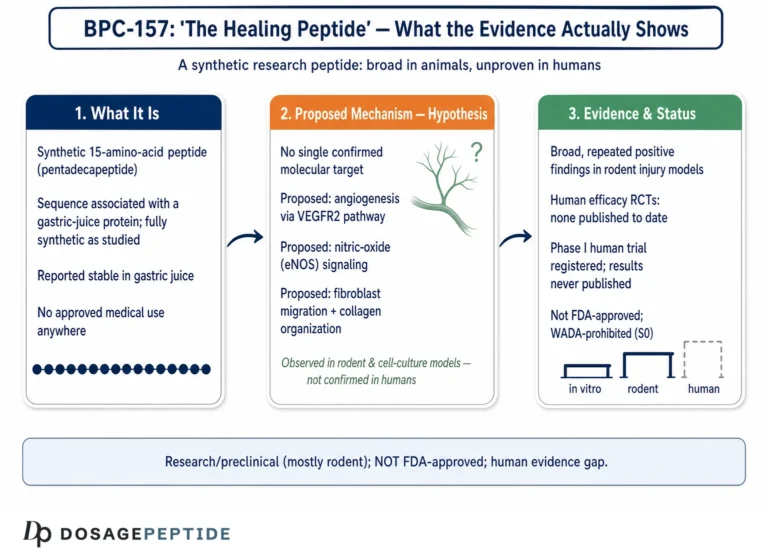
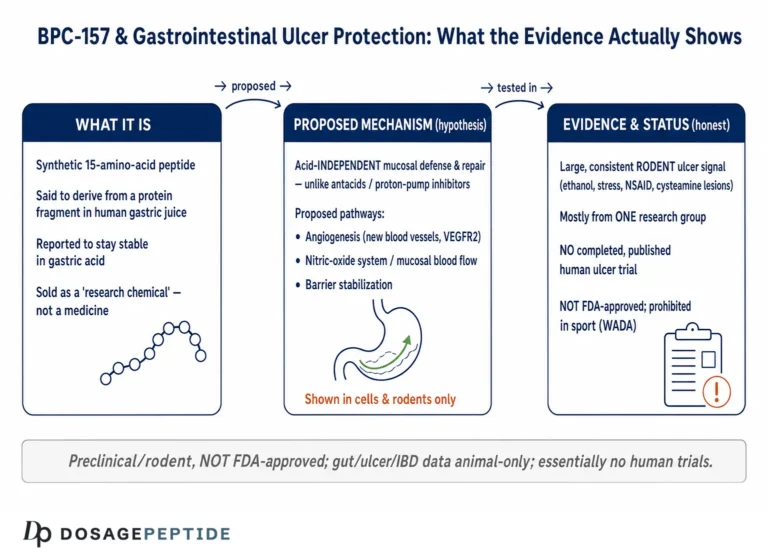
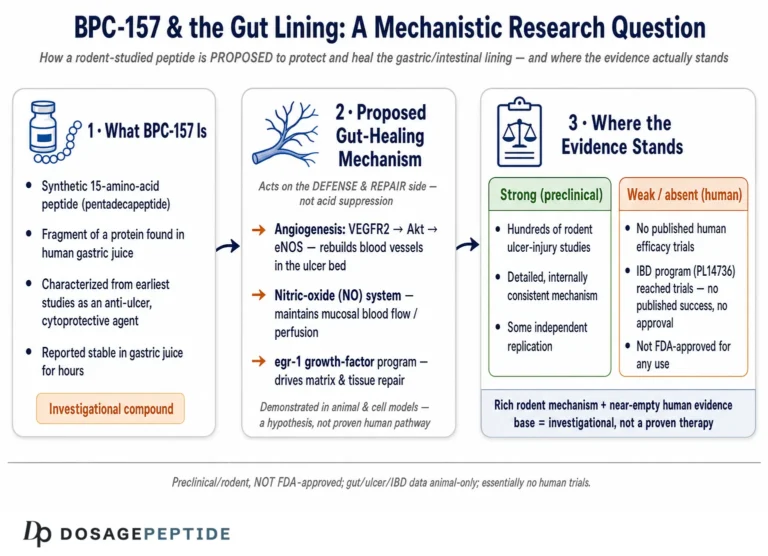
BPC-157 stands for “Body Protection Compound-157.” It is a synthetic pentadecapeptide, meaning it is a chain of exactly 15 amino acids, with the sequence Gly-Glu-Pro-Pro-Pro-Gly-Lys-Pro-Ala-Asp-Asp-Ala-Gly-Leu-Val (single-letter code GEPPPGKPADDAGLV) and a molecular weight of approximately 1419 daltons.1 The peptide is described in the literature as a partial sequence corresponding to a region of a larger protective protein originally identified in human gastric juice. In other words, it was conceived not as a randomly designed molecule but as a fragment thought to carry some of the cytoprotective, “organ-defending” activity that the stomach lining relies on to survive its own acid.1,6
That gastric origin matters for two reasons. First, it explains why the earliest research on BPC-157 focused on the gastrointestinal tract: cytoprotection of the stomach, healing of ulcers, and repair of intestinal anastomoses were the initial targets, and only later did investigators extend the work to tendons, muscle, and bone.6,9 Second, it is the source of one of the peptide’s most-repeated claims: that it is unusually stable in human gastric juice. Several papers report that BPC-157 resists degradation under the extreme low-pH conditions of the stomach, which is notable because most peptides are rapidly broken down there.1 This stability is real and reproducible in the laboratory, but it is frequently over-interpreted in consumer marketing to imply that oral BPC-157 is well absorbed and clinically effective in humans, a claim the published human pharmacokinetic literature simply does not support.
It is worth being precise about terminology, because vendors are not. BPC-157 is sometimes marketed as “stable gastric pentadecapeptide BPC 157,” and a modified, arginine-salt formulation has appeared under the name “BPC-157 arginate” or “stable BPC-157.” These are not identical to the acetate salt most commonly sold, and the overwhelming majority of the primary research uses the base pentadecapeptide administered by injection (intraperitoneal, intramuscular, or intragastric) in rodents. The peptide itself has been developed and studied under industrial designations including PL-10, PLD-116, and PL 14736 by the Croatian pharmaceutical company Pliva, primarily for inflammatory bowel disease.9
Chemically, BPC-157 has no known endogenous receptor. It is not a hormone, and it is not a growth factor in the classical sense. Instead, the working hypothesis in the literature is that it acts as a broad modulator of healing and cytoprotection, nudging several existing signaling systems rather than binding one specific target. This is part of what makes it scientifically interesting and, simultaneously, difficult to characterize: a molecule that appears to touch angiogenesis, nitric oxide signaling, growth-factor receptor expression, and inflammatory tone all at once is hard to pin down with the reductionist tools drug developers usually rely on.
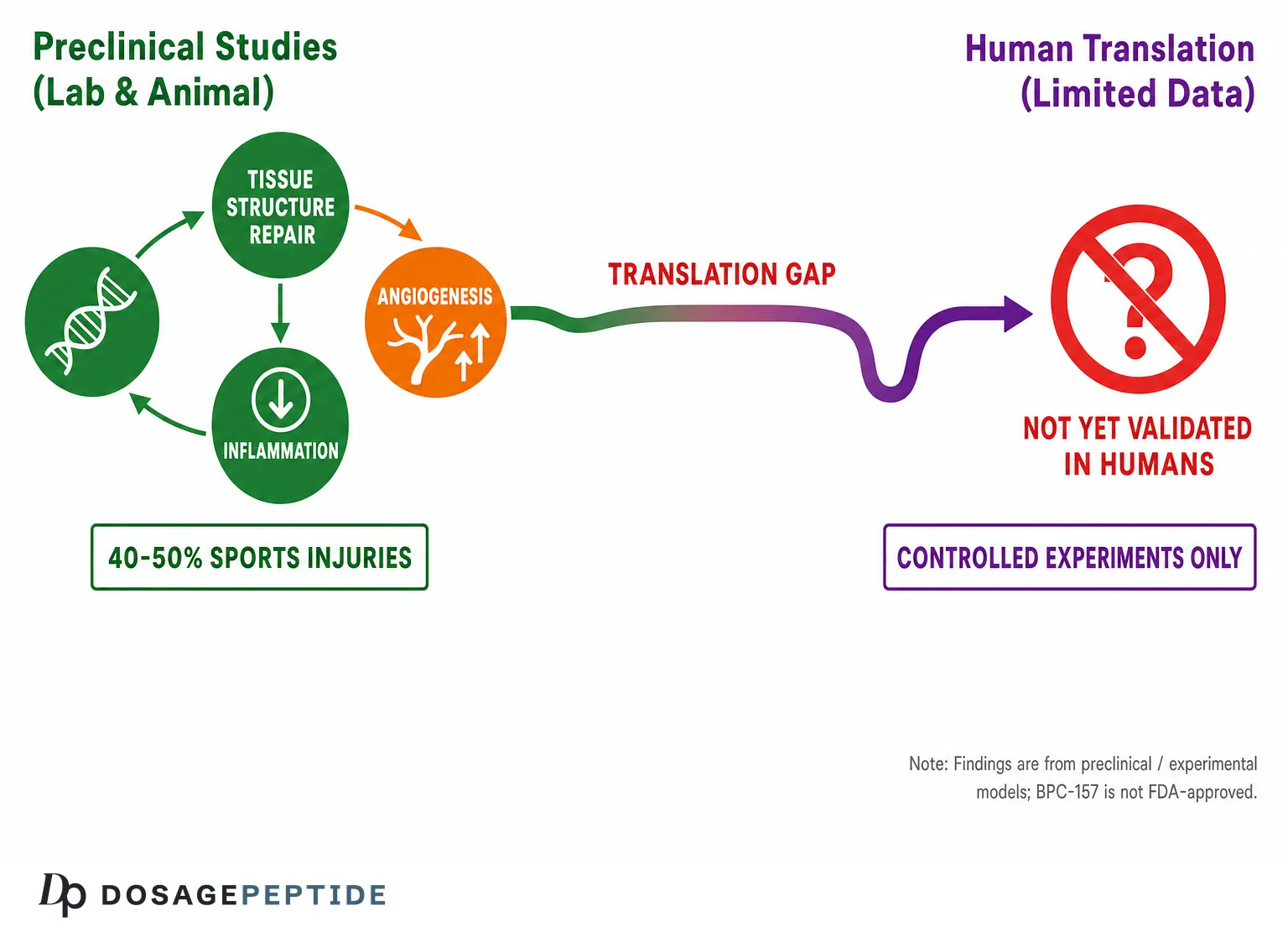
A crucial framing point, established up front: essentially all of the foundational biology described in the sections that follow was generated in animals and in vitro systems. When you read that BPC-157 “enhances,” “accelerates,” or “improves” something, the implied subject is almost always a rat, a mouse, or a dish of cultured cells. That does not make the findings worthless. Rodent models of tendon transection and muscle crush are legitimate, widely used tools in musculoskeletal research. But it does mean that every mechanistic story below carries an invisible asterisk: demonstrated in preclinical models; not established in humans.
The Proposed Molecular Mechanisms
If BPC-157 has no single receptor, how might it promote healing? The literature converges on a handful of overlapping, mutually reinforcing pathways. Understanding them is useful not because any of them is proven to matter clinically, but because they illustrate why researchers find the molecule plausible enough to keep studying.
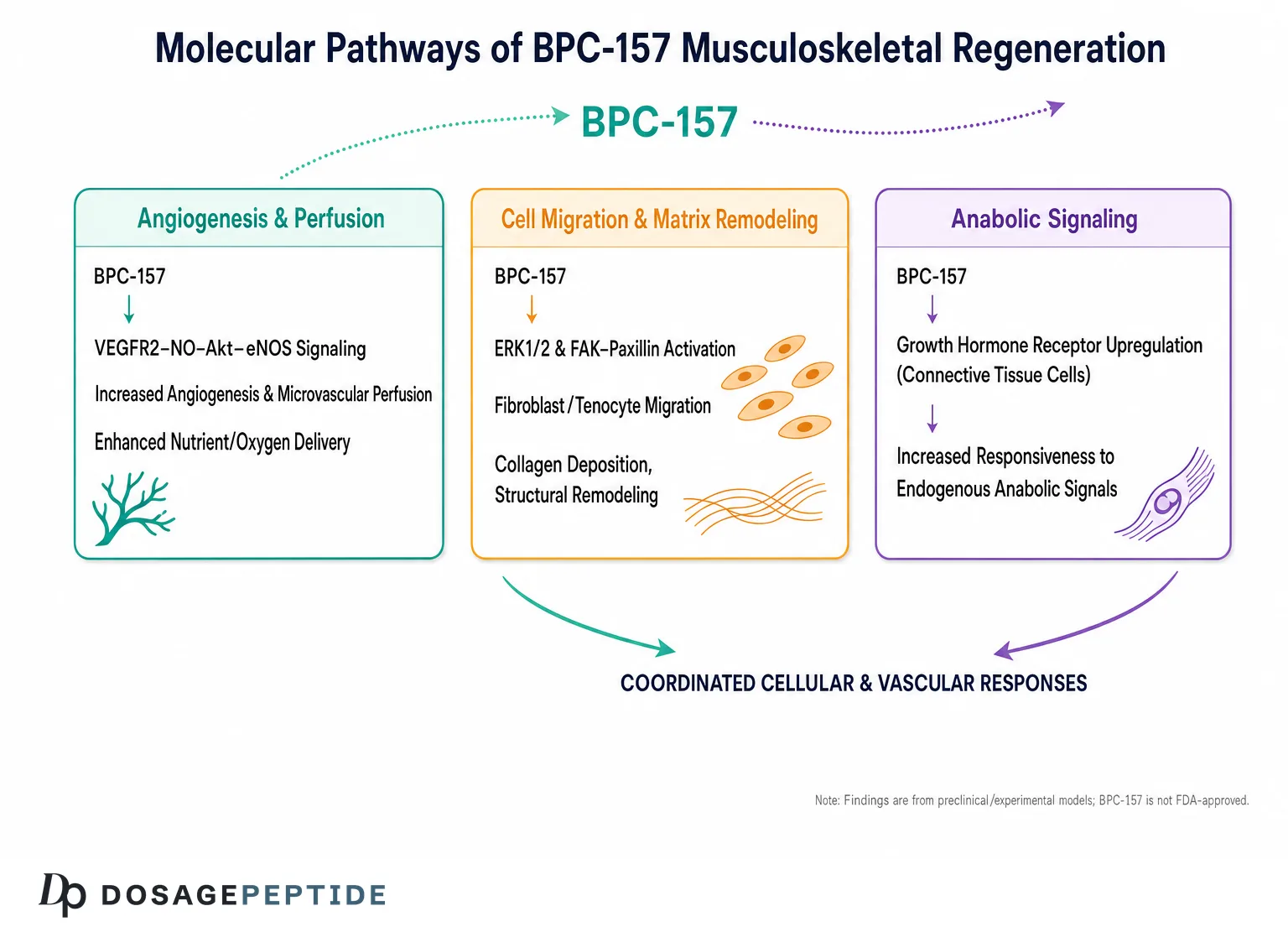
The most consistently cited mechanism is promotion of angiogenesis, the growth of new blood vessels. New vessels bring oxygen, nutrients, and progenitor cells to an injury site, and inadequate blood supply is a genuine bottleneck in the healing of poorly vascularized tissues such as tendons and ligaments. In vitro and in vivo work reports that BPC-157 upregulates vascular endothelial growth factor (VEGF) expression and, importantly, appears to act on the VEGF receptor 2 (VEGFR2) pathway. One influential mechanistic study found that BPC-157 enhances the expression and endocytosis of VEGFR2, which in turn drives phosphorylation of the downstream signaling kinase AKT and of endothelial nitric oxide synthase (eNOS).14
That connects to the second major theme: nitric oxide (NO) signaling. Nitric oxide is a short-lived gas that regulates vascular tone, blood flow, and cytoprotection. A 2020 study in isolated rat aorta showed that BPC-157 produces concentration-dependent, nitric-oxide-dependent effects on vasomotor tone through the Src-Caveolin-1-eNOS pathway, reducing the inhibitory interaction between caveolin-1 and eNOS and thereby increasing NO availability.5 The research group most associated with the peptide has argued for years that BPC-157 acts as a kind of stabilizer of the NO system, protecting or restoring its beneficial functions across many organs.10 It is worth noting that this NO-centric interpretation is itself the subject of scientific debate in the recent literature, with published comment-and-reply exchanges over how much of the effect is truly NO-mediated.10
The third mechanism is the most directly relevant to tendons: upregulation of the growth hormone receptor. In a well-cited 2014 study on cultured tendon fibroblasts, the growth hormone receptor emerged as one of the most strongly upregulated genes after BPC-157 exposure, with dose- and time-dependent increases at both the messenger RNA and protein levels.2 Because growth hormone and its downstream mediator IGF-1 stimulate fibroblast proliferation and collagen synthesis, increased receptor density could plausibly sensitize tendon cells to circulating growth-promoting signals. This is an elegant, tendon-specific mechanism, and it is one reason BPC-157’s soft-tissue reputation is not purely marketing invention.
A fourth cluster of effects involves cell survival, migration, and the cytoskeleton. Work on tendon explants reported that BPC-157 promotes the outgrowth of fibroblasts, supports their survival under stress conditions such as hydrogen-peroxide exposure, and accelerates their migration, an effect the authors linked to activation of the focal adhesion kinase (FAK)-paxillin pathway that governs how cells attach to and crawl across their surroundings.3 Faster, more resilient fibroblast migration into a wound could, in principle, speed the laying down of new collagen matrix.
Finally, the literature describes anti-inflammatory and cytoprotective modulation, including reductions in pro-inflammatory cytokines and a favorable shift in the balance of immune cells at injury sites, with more healing-associated mononuclear cells and fewer destructive granulocytes.4,6 Taken together, the proposed picture is of a molecule that improves blood supply, sensitizes repair cells to growth signals, helps those cells survive and migrate, and calms excessive inflammation. It is a coherent and attractive story. It is also, at present, a story assembled from preclinical fragments, and the relative contribution of each pathway, or whether any of them operates meaningfully in an intact human, remains unresolved.
The Core Preclinical Evidence for Musculoskeletal Healing
The reputation of BPC-157 rests on a specific set of animal experiments in which a defined musculoskeletal injury was created surgically and then treated with the peptide. These studies are the heart of the “evidence,” so they deserve close and honest description, including their consistent finding of benefit and their consistent limitation of being rodent models run largely by one collaborative network.
Tendon. The tendon literature is the most developed. In a frequently cited model, the rat Achilles tendon was completely transected and the animals were then treated with BPC-157. Reports describe improved recovery across multiple domains: biomechanically (greater load to failure and higher Young’s modulus of elasticity, meaning the healed tendon was stronger and stiffer), functionally (better performance on movement tests), microscopically (superior fibroblast and collagen organization with a more favorable inflammatory cell profile), and macroscopically (a smaller tendon defect and more complete restoration of tendon integrity).3 Complementary in vitro work showed that BPC-157 stimulated the growth of tendon explant-derived cells (tendocytes) directly.3 Layered on top is the growth-hormone-receptor finding described above, which provides a candidate molecular explanation for the tissue-level results.2
Muscle and the myotendinous junction. Muscle-healing studies extend the pattern. In rat models of muscle crush injury and of transected or detached muscle, BPC-157 has been reported to improve functional recovery and the histological quality of repair. A 2021 study focused specifically on the myotendinous junction, the mechanically vulnerable interface where muscle meets tendon, and reported that BPC-157 therapy improved healing of this disabled junction in rats, restoring function that was otherwise lost.4 Because the myotendinous junction is a common real-world injury site (think hamstring strains), this line of work is part of why muscle-strain repair became a candidate indication.
Ligament and bone. The evidence extends, more thinly, to ligament and bone. Preclinical studies have reported accelerated healing of transected ligaments and improved outcomes in bone-defect and muscle-to-bone reattachment models, with faster restoration of structural continuity and better biomechanical properties in treated animals compared with controls.7 A recurring experimental design involves surgically detaching a muscle or tendon from its bony insertion and then measuring whether reattachment and healing proceed faster with the peptide.
The single most useful summary of this body of work is a 2025 systematic review of BPC-157 in orthopaedic sports medicine. Searching PubMed, Cochrane, and Embase from inception through June 2024, the authors screened 544 articles and, after applying inclusion criteria, analyzed 36 studies. Of those 36, 35 were preclinical (animal or in vitro) and only 1 was clinical.7 Across the preclinical studies, BPC-157 was reported to improve functional, structural, and biomechanical outcomes in muscle, tendon, ligament, and bony injuries, consistent with the mechanisms of enhanced growth-hormone-receptor expression, angiogenesis, and reduced inflammatory cytokines.7
That 35-to-1 ratio is the single most important number in this entire article. It tells you that the case for BPC-157 in musculoskeletal healing is, quantitatively, an animal case. The consistency of the preclinical results is genuinely notable; it is unusual for a compound to show benefit so reliably across tissue types and laboratories. But consistency in rodents is not the same as efficacy in humans, and a large preclinical literature that has not yet been mirrored by controlled human trials is exactly the pattern seen with many compounds that later failed to replicate their promise in people. For readers exploring how these healing peptides are combined in research protocols, DosagePeptide maintains reference pages such as the BPC-157 + TB-500 blend protocol.
How Strong Is the Evidence, Really?
To weigh BPC-157 fairly, it helps to place its evidence on the standard hierarchy that clinicians and regulators use. At the bottom sit mechanistic and in vitro studies; above them, animal studies; then uncontrolled human case series; then small controlled trials; then large randomized controlled trials; and at the top, systematic reviews and meta-analyses of those trials. BPC-157’s evidence lives almost entirely in the bottom two tiers.
Consider the strengths first, because they are real. The preclinical findings are reproducible across many separate studies and multiple injury models. They are mechanistically coherent, with plausible molecular explanations (angiogenesis, VEGFR2-AKT-eNOS signaling, growth-hormone-receptor upregulation, FAK-paxillin-driven cell migration) that fit the tissue-level results.2,3,5,14 And the effects are often large in the models where they appear, which is why the compound attracted a company’s interest and progressed toward trials in gastrointestinal disease.9
Now the weaknesses, which are equally real and more consequential. The first is the concentration of authorship. A very large fraction of the BPC-157 literature originates from or is connected to a single collaborative research network centered in Croatia, led for decades by Predrag Sikiric and colleagues. This is not an accusation of misconduct; pioneering groups often dominate the early literature on a molecule they discovered. But independent replication by unaffiliated laboratories is a cornerstone of scientific reliability, and the relative scarcity of it here means the evidence base is less diversified than the raw study count suggests.
The second weakness is methodological rigor and risk of bias. The 2025 systematic review summarized the literature but did not pool the data in a meta-analysis or apply a formal, quantitative risk-of-bias score to the included preclinical studies.7 A separate 2026 narrative review of BPC-157 in tissue repair was, by design, a narrative synthesis rather than a registered systematic review, and likewise carried no meta-analysis or standardized risk-of-bias assessment.15 Many individual animal studies do not report blinding of outcome assessors, randomization procedures, or sample-size justification to modern standards. In preclinical research, these omissions are known to inflate apparent effect sizes.
The third and decisive weakness is the near-absence of human efficacy data. As the 2025 systematic review documented, only one of 36 included studies was clinical, and even the widely referenced Phase II program in inflammatory bowel disease (conducted by Pliva under the PL 14736 designation) has never been published as a standalone, peer-reviewed clinical trial report with full results, which makes independent evaluation impossible.7,8,9 For a musculoskeletal indication specifically, there was, until very recently, no completed controlled human trial at all.
| Evidence tier | BPC-157 for musculoskeletal healing | Interpretation |
|---|---|---|
| In vitro / mechanistic | Substantial (tendocyte growth, VEGFR2, GH-receptor, FAK-paxillin) | Plausible biology established |
| Animal studies | Substantial and consistent (35 of 36 studies in the 2025 review) | Promising but not human-predictive |
| Human case series | Anecdotal only; no rigorous published series | Not reliable evidence |
| Controlled human trials | One Phase II musculoskeletal trial recruiting (2026); GI program never fully published | Essentially absent to date |
| Systematic reviews / meta-analyses of trials | None possible (no trial pool exists) | Cannot be assessed |
The honest verdict, then, is that BPC-157 has a strong preclinical evidence base and an empty clinical one for musculoskeletal healing. That is a legitimate and even encouraging place for an early-stage investigational compound to be. It is not a basis for the confident efficacy claims that saturate the consumer market, and it is certainly not evidence that BPC-157 treats or cures any injury or disease in humans.
Comparisons With Related Compounds
BPC-157 is rarely discussed in isolation. Within the research-peptide world it is grouped with, and frequently combined with, several other “healing” and regenerative agents. Comparing them clarifies what is and is not distinctive about BPC-157’s evidence, while reinforcing that all of these compounds share the same fundamental limitation: a preclinical evidence base and no regulatory approval.
TB-500 (a thymosin beta-4 fragment). The most common partner for BPC-157 is TB-500, a synthetic peptide related to the naturally occurring protein thymosin beta-4. Where BPC-157’s proposed mechanisms center on angiogenesis and growth-factor-receptor signaling, TB-500’s center on actin regulation and cell migration. The rationale for combining them is that they might address complementary steps of repair. This pairing is so common that dedicated combination protocols exist, and DosagePeptide documents them in references such as the TB-500 and BPC-157 stack protocol and the standalone TB-500 dosage protocol. Crucially, TB-500 shares BPC-157’s core weakness: its human evidence for musculoskeletal healing is likewise essentially preclinical, and it too is prohibited in sport and unapproved as a drug.
KPV and other anti-inflammatory tripeptides. KPV, a tripeptide fragment of the hormone alpha-MSH, is sometimes added to healing blends for its anti-inflammatory properties, producing three-way combinations. DosagePeptide describes one such formulation in its Tri-Heal (TB-500 + BPC-157 + KPV) protocol reference. The evidentiary situation is the same: interesting preclinical anti-inflammatory data, no controlled human musculoskeletal trials.
Growth hormone secretagogues and IGF-1 pathway agents. Peptides such as the GHRH analogs and ghrelin-receptor agonists are sometimes discussed alongside BPC-157 because tendon and muscle repair depend on the GH/IGF-1 axis, the very axis BPC-157’s growth-hormone-receptor upregulation is thought to sensitize.2 The difference is that at least some GH-axis peptides have more extensive human pharmacology, whereas BPC-157’s growth-hormone-receptor effect has been shown only at the cellular and tissue level in rodents.
Established, evidence-based comparators. The most important comparison is not with other peptides but with interventions that actually have human trial evidence for musculoskeletal healing, however imperfect: structured rehabilitation and progressive loading (the best-supported approach for tendinopathy), and, more controversially, orthobiologics such as platelet-rich plasma. Even these established or semi-established options have mixed or debated human trial data, which puts BPC-157’s complete absence of completed controlled human musculoskeletal trials into stark relief. A compound with zero finished human efficacy trials is not “better than” or “as good as” any of these; it is simply not yet in the same evidentiary conversation.
| Compound | Proposed primary mechanism | Human musculoskeletal trial evidence | Regulatory / sport status |
|---|---|---|---|
| BPC-157 | Angiogenesis, GH-receptor upregulation, NO signaling | Preclinical only; one Phase II strain trial recruiting | Not FDA/EMA approved; WADA-prohibited (S0) |
| TB-500 (TB4 fragment) | Actin regulation, cell migration | Preclinical only | Not approved; WADA-prohibited |
| KPV (alpha-MSH fragment) | Anti-inflammatory signaling | Preclinical only | Not approved as a drug |
| Progressive loading / rehab | Mechanotransduction, tissue remodeling | Multiple human trials (best-supported for tendinopathy) | Standard of care |
The comparative takeaway is not that BPC-157 is uniquely weak; several fashionable regenerative peptides share its evidentiary gaps. It is that none of them, BPC-157 included, has earned the confident healing claims made on their behalf, and that the interventions with genuine human evidence are the unglamorous ones.
Research Models and Methodology
To interpret the BPC-157 literature responsibly, you need to understand the experimental machinery that produced it, because the models both enable the findings and limit their reach. Musculoskeletal healing research in BPC-157 studies relies on a fairly standard toolkit of animal injury paradigms, each with characteristic strengths and blind spots.
The workhorse is the rodent transection or crush model. A tendon (commonly the Achilles), a muscle, or a ligament is surgically severed or crushed under anesthesia, creating a reproducible, well-characterized injury. The animals are then randomized (ideally) to peptide or vehicle control, and healing is measured over days to weeks. Outcomes fall into four families: biomechanical (load to failure, stiffness, Young’s modulus, measured by pulling the healed tissue apart on a materials-testing machine); histological (microscopic assessment of collagen organization, fibroblast density, and inflammatory cell populations); functional (gait, weight-bearing, or movement scores); and macroscopic (defect size, gross integrity).3,4 BPC-157 studies characteristically report benefit across several of these families simultaneously, which is more persuasive than improvement on a single measure.
Alongside whole-animal work sit ex vivo and in vitro systems. Tendon explants, small pieces of harvested tendon cultured in a dish, allow researchers to watch fibroblasts grow out of the tissue and measure how the peptide affects that outgrowth, survival, and migration.3 Isolated cell cultures permit gene- and protein-expression studies, such as the growth-hormone-receptor upregulation work, where messenger RNA and protein levels can be quantified precisely under controlled conditions.2 Isolated tissue preparations, like the rat aortic rings used in the nitric oxide study, let physiologists dissect signaling pathways with pharmacological blockers.5 Each system trades physiological realism for experimental control.
Several methodological features deserve scrutiny. Dosing in these studies is expressed per kilogram of body weight and administered by injection (often intraperitoneal or intramuscular) or intragastrically; the doses used in rodents cannot be linearly extrapolated to human dosing, and doing so is a common error in consumer material. Route matters too: much of the animal data uses injection, so claims about oral efficacy rest on the peptide’s gastric stability rather than on demonstrated oral healing outcomes in people.1 Controls are typically vehicle-injected animals, which is appropriate, but the adequacy of blinding and randomization is inconsistently reported.
There is also the perennial problem of translation. Rodents heal differently from humans: they are smaller, they metabolize compounds faster, their tendons experience different loads, and laboratory injuries are cleaner and more uniform than the chronic, degenerative, mechanically complex injuries humans actually present with. A drug that reliably accelerates healing of a freshly transected rat Achilles tendon may do nothing measurable for a middle-aged runner’s chronic insertional tendinopathy. This is not a hypothetical concern; the history of musculoskeletal medicine is littered with agents that healed rodent injuries and failed human trials.
Finally, pharmacokinetics. Published rodent and beagle-dog data report a short elimination half-life, on the order of well under 30 minutes after intravenous or intramuscular dosing, which raises legitimate questions about how a compound cleared so quickly produces durable tissue-level effects, and no peer-reviewed human pharmacokinetic study has been published to resolve them.7 The proposed answer, that BPC-157 triggers signaling cascades whose effects outlast the molecule’s presence, is plausible but unproven in humans. Understanding these methodological realities is what separates a careful reading of the BPC-157 literature from an credulous one.
Safety and Tolerability Signals
One reason BPC-157 has spread so widely is its reputation for safety, and that reputation is not baseless, but it is frequently overstated and rests almost entirely on animals. Here is what the preclinical safety data actually show, and where the genuine human uncertainties lie.
In rodent toxicology, BPC-157 has a striking profile: acute-toxicity studies have been unable to establish a lethal dose (LD50). Reports describe administering the peptide intravenously or intraperitoneally across an enormous dose range, from nanograms up to very high milligram-per-kilogram quantities, without producing mortality or obvious toxic changes.1,10 The peptide is described as “limit-test negative,” meaning that even at the ceiling doses used in standard toxicology screens, no toxicity threshold was reached.1 Across a large animal literature spanning three decades, significant toxic effects have not been a prominent finding. On its face, this is a reassuring signal.
But several important caveats convert that reassurance into cautious uncertainty. First, and most fundamentally, absence of toxicity in rodents does not establish safety in humans. Human immune systems, metabolism, and long-term physiology differ from those of rodents, and adverse effects that require months or years, or that depend on human-specific biology, would not appear in short rodent studies. Second, regulators have flagged specific concerns that rodent LD50 data do not address. In evaluating BPC-157 for pharmacy compounding, the U.S. Food and Drug Administration raised the possibility of immunogenicity (the risk that an injected peptide provokes an immune response) and highlighted peptide-related impurities arising from manufacturing as potential risks, alongside a general insufficiency of safety data to establish that it is safe for human use.11
That manufacturing point deserves emphasis in a research context. Much of the BPC-157 sold to consumers and, in some cases, used in clinics is produced by suppliers who are not subject to pharmaceutical-grade quality control. Independent testing of research peptides has repeatedly found products that are underdosed, contaminated, or not the labeled compound at all. In this scenario, the relevant safety risk may come less from BPC-157 itself than from what accompanies it in an unregulated vial, including bacterial endotoxin, residual solvents, and synthesis by-products. The clean toxicology of pure peptide in a controlled laboratory says little about the safety of an anonymous product of uncertain purity.
A further, more speculative safety question flows directly from the proposed mechanism. If BPC-157 genuinely promotes angiogenesis, the same property that could help a poorly vascularized tendon heal is theoretically undesirable in the context of a tumor, since solid tumors depend on new blood-vessel growth. This “angiogenesis double-edged sword” has been raised in the literature as a reason for caution, particularly for anyone with a history of cancer, and although there is no direct evidence that BPC-157 promotes tumor growth in humans, the theoretical concern is legitimate and unresolved.10
The bottom line on safety is nuanced rather than alarmist. The preclinical data are genuinely favorable and show no obvious acute toxicity. But “no LD50 in rats” is not the same as “safe for humans,” regulators have identified specific unaddressed concerns, product quality in the real world is highly variable, and the very mechanism that makes the compound interesting carries a theoretical downside. A responsible reading treats BPC-157 as an investigational compound of unknown human safety, not as a proven-safe supplement.
Handling, Reconstitution, and Stability in a Research Context
Because BPC-157 is handled as a lyophilized (freeze-dried) research peptide, its physical handling and stability are practical topics in the laboratory literature, distinct from any question of human use. This section is descriptive of research practice and reflects what published stability observations report; it is not administration guidance.
In its lyophilized powder form, BPC-157 is comparatively stable. Reported storage conditions describe stability on the order of many months to a couple of years when kept frozen (around -20 degrees Celsius) and roughly a year when refrigerated (2 to 8 degrees Celsius), provided the powder is protected from light and moisture. This solid-state stability is one of the more consistent practical observations about the compound and reflects the general behavior of dry peptides, whose degradation reactions are slowed dramatically in the absence of water.
Reconstitution in a research setting typically uses bacteriostatic water, which is sterile water containing about 0.9% benzyl alcohol as a preservative. The benzyl alcohol inhibits microbial growth, which is why bacteriostatic water is preferred over plain sterile water when a reconstituted solution will be stored and drawn from repeatedly rather than used all at once. Once reconstituted, the solution is generally kept refrigerated and, per reported stability observations, retains activity for roughly a few weeks (commonly cited as around 28 days at 2 to 8 degrees Celsius), after which degradation becomes a concern.
The degradation pathways that limit the reconstituted shelf life are the standard enemies of peptides in solution: oxidation, hydrolysis of the peptide bonds, and microbial contamination. Repeated freeze-thaw cycles are described as damaging and are avoided in careful laboratory practice, because each cycle stresses the molecule and can accelerate aggregation and loss of activity. Sterile technique during reconstitution and drawing is emphasized precisely because a contaminated vial is both a stability problem and, in any use scenario, a safety problem.
It is worth noting the apparent paradox between BPC-157’s celebrated gastric stability and its ordinary solution stability. The peptide’s resistance to degradation in stomach acid is a specific, notable property reported in the source literature.1 But that gastric robustness does not make it indefinitely stable once dissolved in water at refrigerator temperature; the two are different chemical situations. This distinction is routinely blurred in marketing that implies the compound is nearly indestructible.
For readers who encounter reconstitution mathematics in research references, DosagePeptide provides worked examples across its protocol pages, such as the BPC-157 protocol reference and its broader peptide dosages index. These are useful for understanding how concentration, vial size, and volume relate arithmetically. None of that arithmetic, however, changes the central regulatory and evidentiary reality described elsewhere in this article: reconstitution technique is a laboratory-handling topic, not a green light for human administration of an unapproved compound.
The Human-Evidence Gap and the First Controlled Trial
The defining feature of BPC-157’s musculoskeletal story is the chasm between its animal evidence and its human evidence. It is worth stating the gap as plainly as possible: as of this writing, there is no completed, published, peer-reviewed randomized controlled trial demonstrating that BPC-157 accelerates the healing of any tendon, ligament, muscle, or bone injury in humans. Every confident claim you have read to the contrary is extrapolating from rodents or citing anecdote.
The closest thing to prior human data comes from outside the musculoskeletal field. In the 2000s, the Croatian company Pliva advanced BPC-157 (as PL 14736) into clinical development for inflammatory bowel disease, and the compound reportedly reached Phase II trials for ulcerative colitis.8,9 This is genuinely relevant because it means the peptide has been administered to humans in a regulated trial setting. But the value of that program as evidence is severely limited by a critical fact: the full results were never published as a standalone, peer-reviewed clinical trial report. The trials appear to have been discontinued, and without published data the outcomes, safety findings, and dosing cannot be independently evaluated.8,9 A trial you cannot read is not usable evidence, and it says nothing directly about musculoskeletal healing.
What has genuinely changed the landscape is the recent launch of the first controlled human trial aimed squarely at a musculoskeletal indication. Registered on ClinicalTrials.gov as NCT07437547 and titled “BPC 157 for Acute Hamstring Muscle Strain Repair,” this is a Phase 2, randomized, double-blind, placebo-controlled study sponsored by Hudson Biotech.12 Its design directly targets the questions this article has raised. Roughly 120 participants with an acute grade II hamstring strain are to be randomized 1:1 to subcutaneous BPC-157 or matching placebo once daily for 14 days, with co-primary endpoints of time to return to unrestricted sport and change in MRI-assessed injury volume at day 14.12 Recruitment reportedly began in early 2026, with primary completion anticipated around early 2027.12
This trial is important for several reasons. It is placebo-controlled and blinded, which addresses the bias concerns that plague the animal literature. It uses an objective structural endpoint (MRI injury volume) alongside a clinically meaningful functional one (return to sport). And it studies exactly the kind of injury, an acute muscle strain at a common real-world site, that BPC-157’s myotendinous-junction preclinical work would predict it might help.4,12 If it reports a positive, robust result, it would be the first real human efficacy signal for musculoskeletal healing. If it is null, it would be a powerful demonstration of how rodent promise can fail to translate.
Until that trial and others like it report, intellectual honesty requires holding the question open. The correct current statement is not “BPC-157 works” and not “BPC-157 doesn’t work,” but rather: BPC-157 shows consistent preclinical promise for musculoskeletal healing, its efficacy in humans is unproven, and the first rigorous human test is only now underway. Anyone claiming more certainty than that, in either direction, is getting ahead of the evidence. It is also worth remembering that a single positive Phase 2 trial, should one emerge, would be a beginning rather than a conclusion; drug approval requires replication, larger trials, and a full safety database.
Regulatory Status
The regulatory picture is unambiguous and important, because it is where the gap between BPC-157’s popularity and its evidence has real legal and safety consequences. To state the core fact directly: BPC-157 is not approved by the U.S. Food and Drug Administration, the European Medicines Agency, or any other national drug regulator for any therapeutic use in humans. It is an investigational compound. It has no approved indication, no approved label, and no established human dosing regimen sanctioned by any regulator.
In the United States, the situation has evolved through the pharmacy-compounding review process, and the details matter. In 2023 the FDA placed BPC-157 in Category 2 of its 503A interim policy on bulk drug substances nominated for compounding, the category for substances that raise significant safety risks, citing concerns including potential immunogenicity, risks from peptide-related manufacturing impurities, and insufficient data to establish that it is safe for human use.11 The regulatory position then shifted rather than hardened: in April 2026 the FDA removed both BPC-157 and TB-500 from Category 2 after the nominations supporting their compounding were withdrawn, which left the peptide in a regulatory gray zone rather than moving it into the permitted Category 1.11 A further review by the FDA’s Pharmacy Compounding Advisory Committee is scheduled for July 23-24, 2026, and as of this writing that meeting has not yet taken place, so its outcome is not known.11 The practical effect today is unchanged in what matters most: BPC-157 has no FDA-approved indication, legitimate compounding of it for human use is not affirmatively sanctioned, and products sold as “research chemicals” carry explicit “not for human use” labeling for a reason.
In the world of competitive sport, the status is equally clear and stricter. BPC-157 was added to the World Anti-Doping Agency (WADA) Prohibited List, where it falls under category S0, “Non-Approved Substances”, which covers pharmacological substances not currently approved by any governmental regulatory health authority for human therapeutic use.13 Because it is on the WADA list, it is prohibited at all times (in and out of competition) for athletes subject to the World Anti-Doping Code, which includes those under the U.S. Anti-Doping Agency (USADA) and equivalent national bodies worldwide.13 There are no therapeutic-use exemptions of the ordinary kind for an S0 substance, and real sanctions have followed real athletes who tested positive.13
These regulatory facts should reframe how the earlier scientific discussion is read. The preclinical promise is real, but “promising in rats and prohibited or unapproved everywhere it matters for humans” is the accurate summary of BPC-157’s status. The compound sits in a legal gray zone sustained by the “research chemical” designation, sold to a public that often treats it as a supplement, while regulators treat it as an unapproved drug with unresolved safety questions and anti-doping authorities treat it as a banned substance. The recently launched Phase 2 trial is the mechanism by which that status could eventually change, but change would require positive, replicated human data and a formal regulatory review that has not happened.11,12,13
For anyone approaching BPC-157, the regulatory status is not a footnote; it is central. It means there is no approved product with guaranteed identity and purity, no sanctioned human dose, no medical oversight framework, and, for athletes, a clear path to sanction. Those realities exist precisely because the human evidence that would justify approval does not yet exist.
Frequently Asked Questions
Is BPC-157 proven to heal tendons and muscles in humans?
No. The evidence that BPC-157 accelerates healing of tendon, muscle, ligament, and bone comes almost entirely from animal studies and cell-culture experiments. A 2025 systematic review of the orthopaedic literature found that 35 of 36 relevant studies were preclinical and only one was clinical.7 There is no completed, published randomized controlled trial demonstrating musculoskeletal healing benefit in humans. The first such trial, a Phase 2 study in acute hamstring strains, only began recruiting in 2026 and had not reported results as of this writing.12
How does BPC-157 supposedly work?
The proposed mechanisms, all demonstrated in preclinical systems, include promotion of new blood-vessel growth (angiogenesis) via the VEGFR2-AKT-eNOS pathway, modulation of nitric oxide signaling, upregulation of the growth hormone receptor on tendon fibroblasts, and enhancement of fibroblast survival and migration through the FAK-paxillin pathway, together with anti-inflammatory effects.2,3,5,14 BPC-157 has no known single receptor and is best understood as a broad modulator of healing pathways rather than a targeted drug. Whether any of these mechanisms operates meaningfully in intact humans is unproven.
Is BPC-157 FDA approved?
No. BPC-157 is not approved by the FDA, the EMA, or any other national regulator for any use. In the United States, the FDA evaluated it for pharmacy compounding and did not permit it, citing concerns about immunogenicity, manufacturing impurities, and insufficient safety data.11 Products are sold as research chemicals labeled “not for human use,” and legitimate compounding for human use is not sanctioned.
Is BPC-157 banned in sports?
Yes. BPC-157 is on the World Anti-Doping Agency Prohibited List under category S0 (Non-Approved Substances), meaning it is prohibited at all times for athletes subject to the World Anti-Doping Code, including those under USADA jurisdiction.13 Athletes have received competition bans for testing positive. There is no ordinary therapeutic-use exemption available for an S0 substance.
Is BPC-157 safe?
Its human safety is not established. Rodent toxicology is favorable, with studies unable to identify a lethal dose even at very high quantities.1 However, absence of toxicity in rats does not prove safety in humans, and regulators have flagged specific unresolved concerns including immunogenicity and impurity risks.11 Real-world product quality is highly variable because most BPC-157 is not made to pharmaceutical standards, and the compound’s proposed angiogenic mechanism raises a theoretical caution for anyone with a history of cancer.10,11
What is the difference between BPC-157 and TB-500?
They are different peptides with different proposed mechanisms that are often combined in research protocols. BPC-157 is a 15-amino-acid peptide linked in preclinical work to angiogenesis and growth-factor-receptor signaling, while TB-500 is a fragment related to thymosin beta-4, associated with actin regulation and cell migration.1,2 Both share the same critical limitation: their musculoskeletal-healing evidence is essentially preclinical, and both are unapproved and prohibited in sport. DosagePeptide documents combined-use references such as the TB-500 and BPC-157 stack protocol.
Why is so much of the BPC-157 research from one group?
A large share of the primary literature originates from or is connected to a single long-running Croatian research network. This is common for a molecule’s discovering laboratory and is not evidence of wrongdoing, but it does mean independent replication by unaffiliated groups is relatively limited, which weakens the overall reliability of the evidence base until more diverse laboratories confirm the findings.7,10
Does BPC-157 work orally?
This is frequently claimed but not well supported for musculoskeletal outcomes. BPC-157 is genuinely reported to be unusually stable in gastric juice, which is the basis for oral-use claims.1 However, gastric stability is not the same as demonstrated oral absorption and healing efficacy in humans, most of the animal healing data used injectable routes, and no peer-reviewed human pharmacokinetic study has established oral bioavailability.1,7
References
- Jozwiak M, et al. Multifunctionality and Possible Medical Application of the BPC 157 Peptide, Literature and Patent Review. Pharmaceuticals. 2025;18(2):185. PMC11859134. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11859134/
- Chang CH, Tsai WC, Hsu YH, Pang JS. Pentadecapeptide BPC 157 Enhances the Growth Hormone Receptor Expression in Tendon Fibroblasts. Molecules. 2014;19(11):19066-19077. PMC6271067. https://pmc.ncbi.nlm.nih.gov/articles/PMC6271067/
- Chang CH, Tsai WC, Lin MS, Hsu YH, Pang JS. The promoting effect of pentadecapeptide BPC 157 on tendon healing involves tendon outgrowth, cell survival, and cell migration. J Appl Physiol. 2011;110(3):774-780. https://journals.physiology.org/doi/abs/10.1152/japplphysiol.00945.2010
- Staresinic M, et al. Stable Gastric Pentadecapeptide BPC 157 as a Therapy for the Disabled Myotendinous Junctions in Rats. PMC8615275. 2021. https://pmc.ncbi.nlm.nih.gov/articles/PMC8615275/
- Hsieh MJ, et al. Modulatory effects of BPC 157 on vasomotor tone and the activation of Src-Caveolin-1-endothelial nitric oxide synthase pathway. Sci Rep. 2020;10:17078. PMC7555539. https://www.nature.com/articles/s41598-020-74022-y
- Seiwerth S, et al. Stable Gastric Pentadecapeptide BPC 157 and Wound Healing. PMC8275860. 2021. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8275860/
- Vasireddi N, Hahamyan H, Salata MJ, Karns M, Calcei JG, Voos JE, Apostolakos JM. Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review. HSS Journal: The Musculoskeletal Journal of Hospital for Special Surgery. 2025;21(4). DOI 10.1177/15563316251355551. PMID 40789979. https://journals.sagepub.com/doi/abs/10.1177/15563316251355551
- Sikiric P, et al. Focus on Ulcerative Colitis: Stable Gastric Pentadecapeptide BPC 157. Curr Med Chem. Bentham Science. https://www.eurekaselect.com/article/18825
- Klicek R, et al. Stable gastric pentadecapeptide BPC 157 in trials for inflammatory bowel disease (PL-10, PLD-116, PL14736, Pliva, Croatia) heals ileoileal anastomosis in the rat. Surgery Today. 2007;37(9):768-777. PMID 17713731. https://pubmed.ncbi.nlm.nih.gov/17713731/
- Sikiric P, et al. Reply to Sikiric et al. BPC 157 Therapy: Targeting Angiogenesis and Nitric Oxide (Comment on Jozwiak et al., Pharmaceuticals 2025, 18, 185). PMC12567171. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12567171/
- U.S. Food and Drug Administration. Pharmacy Compounding Advisory Committee (PCAC) briefing materials on BPC-157 (503A bulk drug substances review; Category 2 placement and subsequent April 2026 removal following nomination withdrawal). FDA PCAC briefing document. https://www.fda.gov/media/193343/download ; PCAC meeting (July 23-24, 2026): https://www.fda.gov/advisory-committees/advisory-committee-calendar/
- ClinicalTrials.gov. BPC 157 for Acute Hamstring Muscle Strain Repair (NCT07437547). Sponsor: Hudson Biotech. 2026. https://clinicaltrials.gov/study/NCT07437547
- U.S. Anti-Doping Agency (USADA). BPC-157: Experimental Peptide Creates Risk for Athletes (WADA Prohibited List, category S0). https://www.usada.org/spirit-of-sport/bpc-157-peptide-prohibited/
- Hsieh MJ, Liu HT, Wang CN, Huang HY, Lin Y, Ko YS, Wang JS, Chang VHS, Pang JHS. Therapeutic potential of pro-angiogenic BPC157 is associated with VEGFR2 activation and up-regulation. J Mol Med (Berl). 2017;95(3):323-333. DOI 10.1007/s00109-016-1488-y. https://doi.org/10.1007/s00109-016-1488-y
- From Regeneration to Analgesia: The Role of BPC-157 in Tissue Repair and Pain Management (2026 narrative review). Int J Mol Sci. 2026;27(6):2876. MDPI. PMID 41898733; PMC13026520. https://www.mdpi.com/1422-0067/27/6/2876
Disclaimer: This article is provided for educational and research purposes only. It is not medical advice, and nothing in it should be interpreted as a recommendation to obtain, possess, or administer BPC-157. BPC-157 is an investigational compound that is not approved by the FDA, EMA, or any other regulatory authority for any use in humans, is not established as safe or effective in people, and is prohibited in competitive sport. The evidence for its effects on musculoskeletal healing is almost entirely preclinical (animal and in vitro). Always consult a qualified, licensed healthcare professional before making any health-related decision.