The question of how retatrutide influences cardiovascular risk factors is, at first glance, a natural one to ask of any compound that produces double-digit weight loss and reshapes the metabolic profile so dramatically. Yet it is important to state plainly, before any numbers are discussed, that retatrutide is an investigational compound. It has not been approved by the U.S. Food and Drug Administration (FDA), the European Medicines Agency (EMA), or any other major regulator for any indication. As a result, the honest framing of this article is not “how does retatrutide treat cardiovascular disease” but rather “what has early research observed about the way retatrutide moves the surrogate markers that clinicians associate with cardiovascular risk, and how confident can we reasonably be in those observations?”1
That distinction matters enormously. Blood pressure, LDL cholesterol, triglycerides, HbA1c, body weight, and waist circumference are all risk factors — statistical predictors of future events such as heart attack, stroke, heart failure, and cardiovascular death. Moving a risk factor in a favorable direction is not the same as demonstrating that fewer people experience those events. Only a dedicated cardiovascular outcomes trial (CVOT), powered to count actual major adverse cardiovascular events (MACE), can establish the latter, and for retatrutide such a trial is only now underway, with results years away.6 Everything discussed below sits squarely in the category of surrogate-marker and early-phase evidence.
This article walks through what retatrutide is and where it came from, the molecular logic behind its effects on the cardiovascular system, the actual trial data on blood pressure, lipids, glycemia and heart rate, how those findings compare with related agents, the research models and methodology that generated them, the safety and tolerability picture, considerations relevant to a laboratory research context, the substantial gaps in the human evidence, and the current regulatory status. Throughout, the emphasis is on describing evidence at its true level of maturity — no more, no less.
What Retatrutide Is and Where It Came From
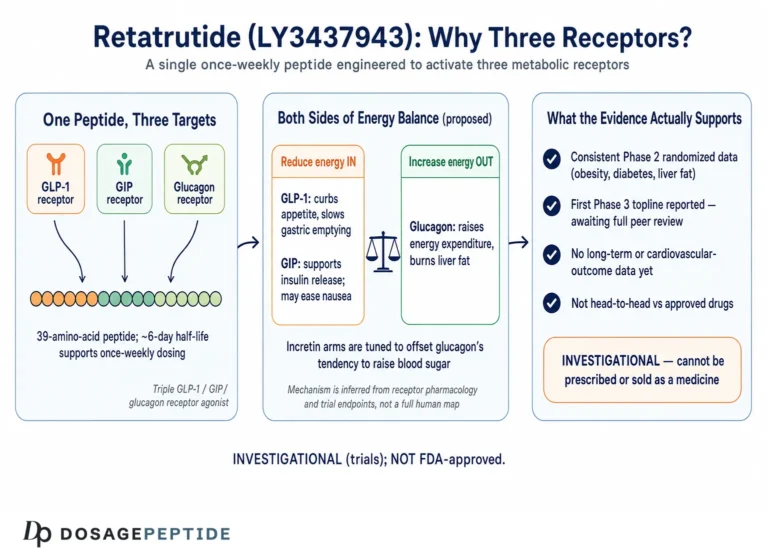
Retatrutide, also known by its development code LY3437943, is a synthetic, once-weekly injectable peptide engineered by Eli Lilly and Company. It belongs to the broad family of incretin-based agents, but it is distinguished by being a triple agonist: a single molecule designed to activate three distinct hormone receptors simultaneously — the glucose-dependent insulinotropic polypeptide (GIP) receptor, the glucagon-like peptide-1 (GLP-1) receptor, and the glucagon receptor.1 This three-receptor engagement is what sets it apart from the first-generation GLP-1 agonists such as semaglutide (single receptor) and from tirzepatide, the “twincretin” that engages GIP and GLP-1 but not glucagon.
The molecule itself is a modified 39-amino-acid peptide built on a glucagon/GIP backbone, with a C20 fatty-diacid moiety attached via a linker. That fatty-acid chain binds reversibly to serum albumin, slowing renal clearance and extending the elimination half-life to roughly six days — long enough to support a single subcutaneous injection per week.7 The design task was deceptively difficult: glucagon and GLP-1 have opposing effects on blood glucose (glucagon raises it, GLP-1 and GIP lower it), so the peptide had to be balanced so that the glucose-lowering incretin arms dominate while the glucagon arm contributes its distinctive effects on energy expenditure and hepatic fat metabolism without producing hyperglycemia.7
Why does the glucagon component matter so much for a cardiovascular discussion? Because glucagon-receptor agonism is the double-edged sword at the heart of retatrutide’s profile. On the favorable side, glucagon receptor activation increases energy expenditure, promotes lipolysis, and drives the striking reductions in hepatic fat that were observed in the liver substudies. On the cautionary side, glucagon has direct chronotropic and inotropic effects on the heart — it can increase heart rate and cardiac output — which is precisely why heart rate has emerged as the most closely watched cardiovascular signal for this compound.1 A candidate that reshapes weight, lipids and blood pressure favorably while nudging resting heart rate upward creates a genuinely open scientific question about the net cardiovascular balance, and that question is exactly what the ongoing outcomes trial is built to answer.
It is worth dwelling briefly on the historical trajectory of incretin science, because it explains why a triple agonist exists at all. The field began with the observation that gut-derived hormones amplify insulin secretion after a meal — the so-called incretin effect. GLP-1 was the first to be therapeutically exploited, yielding the GLP-1 receptor agonists. Researchers then reasoned that combining GLP-1 with a second incretin, GIP, might amplify metabolic benefit while improving tolerability, producing the dual agonist tirzepatide. Retatrutide represents the next conceptual step: adding glucagon-receptor agonism to recruit an additional axis of energy expenditure and hepatic fat mobilization. Each added receptor arm was intended to compound metabolic efficacy, and it is this stepwise escalation of pharmacological ambition that places retatrutide’s cardiovascular-risk-factor effects at the potent end of the spectrum — while also introducing the glucagon-driven heart-rate consideration that its predecessors largely avoided.7
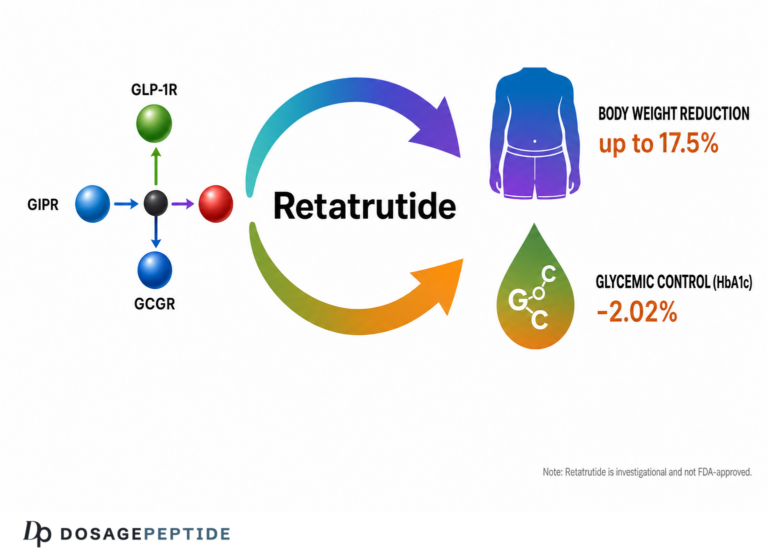
Retatrutide entered clinical testing around 2020–2021. Its pivotal early readout was a phase 2 trial in adults with obesity, published in the New England Journal of Medicine in 2023, which reported some of the largest weight reductions seen in the incretin field to that point — a mean of roughly 24 percent at 48 weeks in the highest-dose group.1 Those weight results, combined with parallel signals in type 2 diabetes and in metabolic dysfunction-associated steatotic liver disease (MASLD), propelled the compound into a large phase 3 program branded TRIUMPH. It is against that backdrop of dramatic weight and metabolic change that the cardiovascular-risk-factor data must be read, because many of the observed cardiovascular effects are at least partly downstream of weight loss itself rather than independent, direct drug actions. Readers interested in the formulation and vial-size landscape can review the peptide dosage protocol library for context on how this investigational compound is described in research settings.
Molecular Mechanism: How Three Receptors Shape Cardiometabolic Signals
To understand how retatrutide might influence cardiovascular risk factors, it helps to trace each receptor arm and its downstream physiology, then consider how they combine. This is mechanistic reasoning grounded in receptor pharmacology; it explains why certain markers move, but it does not by itself prove clinical benefit.
The GLP-1 receptor arm is the best characterized. GLP-1 receptor activation enhances glucose-dependent insulin secretion, suppresses inappropriate glucagon release after meals, slows gastric emptying, and acts centrally to reduce appetite. In the cardiovascular context, GLP-1 receptors are expressed in the heart, vasculature, kidney and central nervous system, and the class has been associated in approved agents with modest reductions in systolic blood pressure, favorable shifts in lipids, anti-inflammatory effects, and — importantly — a small increase in heart rate.1 Much of the blood-pressure lowering seen across the incretin class is thought to reflect a combination of weight loss, natriuresis (increased sodium excretion), improved endothelial function, and reduced arterial stiffness.
The GIP receptor arm is more nuanced and its cardiovascular contribution is still debated. GIP potentiates insulin secretion and appears to modulate adipose tissue metabolism and, in the brain, may reduce nausea and improve tolerability, potentially allowing higher effective dosing of the other components. Its independent effect on blood pressure or lipids in humans is less clearly defined, and researchers generally regard the GIP arm as a metabolic and tolerability enhancer rather than a primary driver of vascular risk factors.7
The glucagon receptor arm is the differentiator and the source of both the most interesting benefits and the principal cautionary signal. In the liver, glucagon receptor activation increases fatty-acid oxidation and reduces hepatic steatosis, which is the mechanistic explanation for the very large liver-fat reductions observed in the MASLD substudy.2 Systemically, glucagon raises energy expenditure, contributing to weight loss beyond appetite suppression alone. But glucagon receptors are present in cardiac tissue, and glucagon has long been known in clinical medicine as a positive chronotrope and inotrope — it is even used acutely to counteract beta-blocker overdose. The concern, therefore, is that sustained glucagon-receptor agonism could raise resting heart rate, and indeed a dose-dependent heart-rate increase is the most consistent cardiovascular signal reported for retatrutide.1
It is also worth considering the vascular and renal biology that may contribute to the blood-pressure findings. Incretin receptor activation has been linked in the broader literature to natriuresis — the kidney’s excretion of sodium — which reduces circulating volume and can lower blood pressure independently of weight. There is also evidence across the class for improved endothelial function and reduced arterial stiffness, both of which favor lower systolic pressure. Whether retatrutide engages these pathways to the same degree as pure GLP-1 agents, and how the glucagon arm modulates them, has not been directly established, so these mechanisms remain plausible contributors rather than proven ones. The honest mechanistic summary is that several biologically reasonable pathways point toward blood-pressure lowering, and the trial data are consistent with them, but attribution to any single mechanism is speculative.1
The inflammatory dimension deserves brief mention as well. Obesity and hepatic steatosis are associated with chronic low-grade inflammation, itself a contributor to atherogenesis. By reducing visceral fat, hepatic fat, and body weight so substantially, retatrutide would be expected to lower systemic inflammatory tone, and reductions in markers such as high-sensitivity C-reactive protein are commonly observed across the incretin class with significant weight loss. If present, such anti-inflammatory shifts would represent an additional favorable influence on the cardiovascular milieu — but they are, once again, surrogate observations several steps removed from demonstrated clinical benefit, and they should be weighted accordingly.
When these three arms are combined in one molecule, the net effect on cardiovascular risk factors is a composite. Favorable pressure comes from profound weight loss, reduced visceral and hepatic fat, improved insulin sensitivity, lower triglycerides and atherogenic lipoproteins, and lower blood pressure. Countervailing pressure comes chiefly from the heart-rate elevation. The lipid effects deserve particular mechanistic attention: the reduction in triglyceride-rich lipoproteins and apolipoprotein C-III observed in the trials is consistent with enhanced clearance and reduced hepatic secretion of very-low-density lipoprotein, plausibly linked to the glucagon-driven improvement in liver fat.3 In other words, the same glucagon arm that raises the heart-rate question may also be responsible for some of the most cardioprotective-looking lipid shifts. This tension — benefit and caution flowing from the same receptor — is precisely why the compound cannot be assumed cardioprotective and why an outcomes trial is indispensable.
Key Evidence: What the Trials Actually Measured
The strongest human evidence on retatrutide’s cardiovascular risk factors comes from a small number of randomized, placebo-controlled phase 2 studies and their secondary analyses. It is essential to keep the evidence hierarchy in view: these are surrogate-marker findings from mid-stage trials, not outcome data.
The anchor study is the phase 2 obesity trial (NCT04881760) published in NEJM in 2023. It randomized 338 adults with obesity (BMI ≥30, or ≥27 with a weight-related condition) and without diabetes to placebo or retatrutide at escalating maintenance doses of 1, 4, 8, or 12 mg once weekly, over 48 weeks.1 Weight loss was the primary endpoint, but the trial pre-specified several cardiovascular risk factors as secondary and exploratory endpoints, including 24-hour ambulatory blood pressure, heart rate, and fasting lipids.
On blood pressure, the trial reported dose-related reductions in systolic pressure, with the higher-dose groups showing mean decreases in the range of roughly 4 to 8 mmHg from baseline by 24 weeks, versus little change on placebo, alongside smaller reductions in diastolic pressure.1 On heart rate, the same trial observed a dose-dependent increase, with mean elevations broadly in the range of a few beats per minute up to roughly 6 to 7 bpm at the higher doses at the point of maximum effect, generally attenuating somewhat over time.1 This is the signature push-pull of the compound: blood pressure down, heart rate up.
The lipid data are among the most striking. A dedicated secondary analysis presented at the European Society of Cardiology Congress in 2024 and published in the European Heart Journal supplement examined lipoprotein and apolipoprotein changes in the phase 2 cohort. At 48 weeks, retatrutide reduced non-HDL cholesterol by up to about 26.9 percent, triglycerides by up to about 40.6 percent, apolipoprotein B by up to about 24.2 percent, and apolipoprotein C-III by up to about 38.0 percent, all in a dose-dependent manner.3 The analysis also reported reductions in the total number of triglyceride-rich lipoprotein particles and small, highly atherogenic LDL particles, with a shift toward larger average HDL particle size.3 These directional changes are the kind clinicians associate with lower atherogenic burden — but again, they are marker changes, not demonstrated event reductions.
A 2026 systematic review and meta-analysis pooling the available randomized data offered somewhat more conservative aggregate estimates, reporting statistically significant reductions in systolic blood pressure of roughly 6.8 mmHg, diastolic pressure of roughly 2.5 mmHg, total cholesterol of about 22 mg/dL, LDL cholesterol of about 13 mg/dL, and triglycerides of about 41 mg/dL, while also confirming the heart-rate increase.4 The gap between the meta-analytic averages and the top-line single-study percentages is a useful reminder that effect sizes depend heavily on dose, population, and analysis method — and that pooled estimates temper the most dramatic single-arm figures.
| Cardiovascular risk factor | Reported direction & approximate magnitude | Evidence source | Level of evidence |
|---|---|---|---|
| Systolic blood pressure | Decrease, ~4–8 mmHg (single trial); ~6.8 mmHg (pooled) | Phase 2 obesity trial; meta-analysis | Surrogate, phase 2 |
| Diastolic blood pressure | Decrease, ~2–3 mmHg | Phase 2 trial; meta-analysis | Surrogate, phase 2 |
| Resting heart rate | Increase, ~2–7 bpm, dose-dependent | Phase 2 obesity trial | Surrogate, phase 2 |
| Triglycerides | Decrease, up to ~40% | ESC 2024 lipid substudy | Surrogate, secondary analysis |
| Non-HDL cholesterol | Decrease, up to ~27% | ESC 2024 lipid substudy | Surrogate, secondary analysis |
| Apolipoprotein B | Decrease, up to ~24% | ESC 2024 lipid substudy | Surrogate, secondary analysis |
| Body weight | Decrease, up to ~24% at 48 wk (phase 2) | Phase 2 obesity trial | Primary endpoint, phase 2 |
| MACE (heart attack, stroke, CV death) | Not yet established | CVOT ongoing | No completed outcome data |
Beyond blood pressure and lipids, the glycemic and anthropometric risk factors also moved favorably. Retatrutide reduced HbA1c and fasting glucose, improved measures of insulin sensitivity, and produced large reductions in waist circumference — a proxy for visceral adiposity that is itself an independent cardiovascular risk marker. In the type 2 diabetes arm of the phase 2 program, glycemic control improved substantially, consistent with the dominant incretin action of the molecule.1 Because dysglycemia and central adiposity are well-established contributors to cardiovascular risk, these changes reinforce the overall favorable surrogate picture. Yet they carry the same caveat as every other marker discussed: improvement in a glycemic or anthropometric surrogate is a predictor of, not a substitute for, reduced cardiovascular events.
The hepatic evidence adds a further dimension that is increasingly recognized as cardiovascular-relevant. In the MASLD substudy of the phase 2 program, retatrutide reduced liver fat content dramatically — by up to roughly 80 percent at higher doses at 24 weeks, with a large proportion of participants achieving normalization of liver fat.2 Because metabolic dysfunction-associated steatotic liver disease is bidirectionally linked with cardiovascular disease, and because hepatic fat drives atherogenic dyslipidemia, the striking liver-fat reductions are mechanistically consistent with the observed triglyceride and lipoprotein improvements. This coherence across liver and lipid endpoints strengthens the biological plausibility of the profile, even as it remains, in the strict sense, an interlocking set of surrogates rather than outcome proof.
The bottom line on evidence: retatrutide favorably moves nearly every cardiovascular risk factor that has been measured, sometimes to a striking degree, and it raises one — resting heart rate. Whether the favorable marker changes translate into fewer cardiovascular events, and whether the heart-rate increase carries any long-term risk, is genuinely unknown and awaits the outcomes trial.
Comparisons With Related Incretin Agents
Placing retatrutide alongside its better-studied relatives clarifies both what is novel about its cardiovascular-risk-factor profile and what remains uncertain. The natural comparators are semaglutide (a GLP-1 receptor agonist) and tirzepatide (a GIP/GLP-1 receptor agonist), both of which are approved and, in semaglutide’s case, backed by completed cardiovascular outcomes data.
On weight and metabolic magnitude, the phase 2 and emerging phase 3 data position retatrutide at the high end of the class, with mean weight reductions exceeding those typically reported for semaglutide and generally at or above tirzepatide at comparable time points.1,5 Because so many cardiovascular risk factors track with weight, this alone would predict favorable movements in blood pressure, glycemia and lipids — and that is broadly what the data show.
On blood pressure, all three agents lower systolic pressure, and the magnitude seen with retatrutide in phase 2 is at least comparable to, and in some analyses larger than, the reductions reported for semaglutide and tirzepatide, plausibly reflecting greater weight loss.4 On lipids, the triglyceride and atherogenic-lipoprotein reductions with retatrutide appear robust and are consistent with — and in the case of triglycerides possibly larger than — the class, likely aided by the glucagon-driven hepatic-fat reduction that the pure GLP-1 agents cannot match.2,3
The heart-rate comparison is where the picture diverges most. All incretin agents raise heart rate modestly, but retatrutide’s glucagon-receptor component provides an additional, mechanistically distinct driver, and several analyses suggest its heart-rate elevation may sit at or slightly above the upper end of the class.1 This does not automatically imply worse outcomes — semaglutide raises heart rate yet demonstrated cardiovascular benefit in outcome trials of its own indications — but the larger the heart-rate signal, the more important direct outcome confirmation becomes.
It is also instructive to compare the three agents on the coherence of their risk-factor packages. Semaglutide and tirzepatide each deliver a broadly favorable bundle — weight down, glycemia improved, blood pressure lower, lipids improved, heart rate modestly up. Retatrutide delivers a similar bundle but appears to push several components further, and it adds a distinctive hepatic-fat effect that the pure GLP-1 agents cannot replicate. In principle, a larger favorable movement across many correlated risk factors ought to predict greater benefit; in practice, cardiovascular pharmacology has repeatedly shown that the relationship between surrogate magnitude and outcome magnitude is not linear and cannot be assumed. The heart-rate signal is the specific reason this caution is not merely theoretical for retatrutide: it introduces a countervailing element whose weight in the final balance is unknown.1,4
A further comparative nuance concerns tolerability-driven dosing. The GIP component is thought to soften the gastrointestinal burden of aggressive incretin agonism, potentially allowing patients to reach and sustain higher effective doses. Since risk-factor benefit is dose-dependent, tolerability that permits higher maintenance dosing indirectly shapes the cardiovascular-risk-factor profile. This is a subtle but real way in which the multi-receptor design influences the cardiometabolic outcome, and it distinguishes the mechanism-level comparison from a simple ranking of potency.
The single most important comparison, however, is at the level of evidence maturity, not effect size. Semaglutide has completed dedicated cardiovascular outcomes trials in relevant populations, providing hard-endpoint data. Tirzepatide’s outcomes program has been maturing. Retatrutide, by contrast, has no completed outcomes trial at all; its cardiovascular case rests entirely on risk-factor surrogates and mechanistic analogy to the class.6 So while retatrutide may look, on paper, like the most potent cardiometabolic risk-factor modifier of the group, it is simultaneously the least proven in terms of the endpoints that actually matter to patients. That combination — impressive surrogates, absent outcomes — is exactly the situation in which overinterpretation is most tempting and most inappropriate. For readers comparing formulations across the class, the site’s 12 mg retatrutide protocol reference and related vial pages catalog how the investigational compound is described relative to its dose range.
Research Models and Methodology
Understanding how the cardiovascular-risk-factor data were generated is essential to judging their reliability. The findings come from a layered research pipeline: preclinical pharmacology, then randomized human phase 2 trials, then secondary and pooled analyses, and — pending — outcome trials.
At the preclinical stage, retatrutide’s receptor activity was characterized in cell-based assays measuring cyclic AMP signaling at the human GIP, GLP-1 and glucagon receptors, establishing the relative potency at each. Animal models (rodents and non-human primates) then demonstrated the combined effects on food intake, body weight, glucose tolerance, energy expenditure and hepatic lipid content that motivated the balanced triple-agonist design.7 These models are indispensable for mechanism but translate imperfectly to human cardiovascular physiology, and no animal model reliably predicts human MACE.
The human phase 2 methodology is the backbone of the current cardiovascular-risk-factor evidence. The obesity trial used randomization, placebo control, and blinding, with dose escalation to mitigate gastrointestinal side effects. Critically for cardiovascular questions, it employed 24-hour ambulatory blood pressure monitoring for blood pressure and heart rate rather than relying solely on single clinic measurements — a methodological strength, because ambulatory monitoring captures the full circadian profile and is less prone to white-coat effects.1 Lipids were measured as fasting standard panels, and the deeper lipoprotein-particle and apolipoprotein analyses used specialized assays (for example, nuclear magnetic resonance particle profiling) reported in the ESC secondary analysis.3
Several methodological limitations must be weighed. First, the phase 2 trials were powered for weight loss, not for cardiovascular endpoints; the blood-pressure, heart-rate and lipid findings are secondary or exploratory, meaning they are hypothesis-generating rather than confirmatory and carry a greater risk of chance findings. Second, the sample sizes are modest — a few hundred participants total, with the liver substudy involving fewer than 100 — limiting the ability to detect rarer cardiovascular signals such as arrhythmia. Third, the trials were relatively short (up to 48 weeks), whereas cardiovascular risk plays out over years. Fourth, the populations were selected (adults with obesity, largely without established cardiovascular disease), so the findings may not generalize to higher-risk groups.1
The meta-analysis methodology adds value by pooling across studies to produce more stable estimates, but it inherits the limitations of its inputs: if all included trials share the same short duration and surrogate endpoints, pooling cannot overcome those constraints — it can only sharpen the estimate of the surrogate effect.4 Finally, the outcomes trial (TRIUMPH-Outcomes) represents the methodologically decisive step: an event-driven, large-scale randomized trial that counts adjudicated MACE in a population with established cardiovascular disease, running for several years until a pre-specified number of events accrue.6 Until that trial reports, the methodological ceiling on any cardiovascular claim for retatrutide is “favorable surrogate change,” and no rigorous reading of the current literature can honestly go beyond it.
Safety and Tolerability in the Cardiovascular Context
Any discussion of cardiovascular risk factors must be paired with the broader safety and tolerability profile, because tolerability shapes whether the favorable risk-factor changes could ever be sustained, and because some adverse effects have indirect cardiovascular relevance.
The dominant adverse events across the retatrutide trials were gastrointestinal — nausea, vomiting, diarrhea and constipation — typical of the incretin class and driven largely by the GLP-1 arm and gastric-emptying effects. These were mostly mild to moderate, dose-related, and tended to occur during dose escalation before attenuating.1 While GI effects are not directly cardiovascular, severe vomiting or diarrhea can cause volume depletion and electrolyte disturbance, which in vulnerable individuals can have downstream cardiovascular and renal consequences; this is one reason gradual dose escalation is emphasized.
The most cardiovascularly specific tolerability signal is the heart-rate increase already discussed. In the phase 2 trials, this elevation was dose-dependent but was not accompanied by a signal of increased arrhythmia or serious cardiovascular events over the study period — although, as noted, the trials were too small and too short to rule such signals out.1 The clinical significance of a sustained few-beats-per-minute rise in resting heart rate over years is genuinely uncertain: epidemiologically, higher resting heart rate is associated with worse cardiovascular outcomes, yet drug-induced heart-rate increases do not always carry the same prognostic weight, and this is one of the specific uncertainties the outcomes trial is designed to resolve.
Other observed effects with metabolic-cardiovascular relevance include modest increases in heart rate coinciding with reductions in blood pressure (the push-pull noted throughout), transient changes in some laboratory parameters, and — reassuringly in the liver substudy — reductions in hepatic fat with no hepatotoxicity signal through 48 weeks.2 As with the entire GLP-1/incretin class, class-level cautions such as the theoretical concern regarding thyroid C-cell tumors (based on rodent data), pancreatitis monitoring, and gallbladder-related events are typically carried forward into the investigational safety framework, though these are not specific to retatrutide’s cardiovascular profile.
It is also worth situating the heart-rate observation within the wider physiology of the compound. A rise in resting heart rate can, in principle, reflect several non-equivalent phenomena: direct cardiac stimulation, a compensatory response to peripheral vasodilation or blood-pressure lowering, or shifts in autonomic tone accompanying rapid weight loss and altered energy metabolism. Distinguishing among these possibilities matters, because a heart-rate increase that reflects benign hemodynamic adjustment carries a different prognostic implication than one reflecting sustained sympathetic or direct chronotropic drive. The current phase 2 data do not resolve which mechanism predominates, and this mechanistic ambiguity is one more reason the long-term significance of the heart-rate signal cannot be settled without dedicated outcome and physiological studies.1
A crucial safety caveat concerns unregulated sourcing. Because retatrutide is investigational and not approved, any material encountered outside a sanctioned clinical trial is not a pharmaceutical product and has not passed regulatory manufacturing and quality controls. Purity, identity, sterility, endotoxin content and actual peptide quantity cannot be assumed. From a cardiovascular-safety standpoint, this compounds the uncertainty enormously: the favorable risk-factor data were generated with a precisely characterized clinical-grade molecule at defined doses under medical supervision with cardiovascular monitoring, none of which applies to non-clinical material. Nothing in the trial literature should be read as endorsing use outside a controlled clinical or laboratory research context.
Handling and Reconstitution in a Research Context
In laboratory and research settings where investigational peptides are handled, questions of physical handling and reconstitution frequently arise. This section is included for completeness and describes general peptide-handling principles reported in the research literature; it is not a use protocol, not medical guidance, and not an endorsement of administration to humans or animals outside sanctioned studies. Retatrutide remains investigational, and handling of any research compound must comply with applicable institutional and legal requirements.
Lyophilized (freeze-dried) peptides of this class are typically supplied as a white powder in a sealed vial and are generally described in the research literature as requiring cold storage, with the dry powder often kept frozen for longer-term stability and reconstituted material kept refrigerated and used within a limited window. Reconstitution in a research context typically involves a sterile diluent such as bacteriostatic water, added slowly against the vial wall rather than directly onto the powder to minimize mechanical stress on the peptide, followed by gentle swirling rather than vigorous shaking, which can shear and denature peptide chains.1
Concentration arithmetic is a routine source of error in research handling and is worth understanding conceptually: the final concentration is simply the mass of peptide in the vial divided by the volume of diluent added. A larger vial nominal size does not change the underlying peptide chemistry — it changes the mass available and therefore the concentration for a given diluent volume. Research-oriented reference pages such as the 6 mg vial protocol, the 20 mg vial protocol, the 24 mg vial protocol, and the 30 mg vial protocol catalog how different nominal vial sizes map to reconstitution math in a research reference framework. These pages are informational references, not authorizations for use.
From a cardiovascular-research standpoint, the handling discussion matters for one specific reason: reproducibility. The favorable blood-pressure and lipid data described earlier were obtained with a precisely quantified, quality-controlled clinical compound. Any material of uncertain concentration or purity introduces uncontrolled variables that make it impossible to relate observed physiological effects — including any change in heart rate or blood pressure — back to a known exposure. This is a core reason why surrogate-marker data from rigorous trials cannot be extrapolated to non-clinical settings, and why the research-integrity emphasis on characterized material and accurate concentration is inseparable from the cardiovascular question. Verification tools such as a certificate of analysis are frequently referenced in the research-integrity literature as a minimum expectation for compound identity in any laboratory context.
Limitations and the Human-Evidence Gap
Having surveyed the favorable risk-factor data, it is now essential to be explicit and thorough about what those data do not show, because the gap between surrogate improvement and clinical benefit is the single most important idea in this entire article.
The foremost limitation is the absence of any completed cardiovascular outcomes trial. Every cardiovascular claim about retatrutide currently rests on surrogate endpoints — blood pressure, lipids, glycemia, weight, heart rate. The history of cardiovascular medicine contains cautionary examples in which drugs improved surrogate markers yet failed to reduce, or even worsened, hard outcomes. Improving a risk factor is a necessary-looking but not sufficient condition for clinical benefit, and only an adequately powered, event-driven trial can close that gap.6 For retatrutide, that trial is ongoing and years from reporting.
A second limitation is the heart-rate signal itself, which represents a directionally unfavorable change embedded within an otherwise favorable profile. Because elevated resting heart rate is epidemiologically linked to adverse cardiovascular outcomes, and because retatrutide’s glucagon arm provides a plausible mechanism for sustained elevation, this signal cannot be dismissed. It is precisely the kind of finding that surrogate data cannot resolve — the net effect of “many markers better, one marker worse” can only be adjudicated by counting events.1
Third, the existing trials have limited scope and duration. They enrolled hundreds, not thousands, of participants; ran for up to about a year; largely excluded people with established cardiovascular disease; and under-represented some demographic groups. Cardiovascular events accrue over years in higher-risk populations, so short trials in lower-risk cohorts cannot characterize the event profile that matters most.1,4
Fourth, much of the favorable risk-factor change is plausibly weight-loss-mediated rather than a direct vascular drug effect. This is not a criticism — weight loss is a legitimate route to better risk factors — but it means the cardiovascular story is entangled with, and partly secondary to, the weight story, and disentangling direct from indirect effects requires dedicated study designs not yet completed.
Fifth, the strongest lipid findings come from secondary and exploratory analyses, which are more susceptible to multiplicity (the statistical problem of many comparisons yielding some chance findings) and require confirmation in prospectively designed studies. The 2026 meta-analysis, while valuable, cannot transcend the surrogate nature of its source data.3,4
A sixth consideration is publication and reporting maturity. Much of the most eye-catching cardiovascular-risk-factor data has been communicated through conference presentations and supplement abstracts rather than full, peer-reviewed primary articles subject to complete methodological scrutiny. Conference data are legitimate and often preview robust findings, but they typically provide less detail on statistical handling, subgroup behavior, and adverse-event granularity than a full manuscript. Prudent interpretation therefore treats the headline lipid percentages as provisional until fully reported, and weights the peer-reviewed obesity and liver trials more heavily in any honest appraisal.3
Taken together, these limitations define an honest verdict: retatrutide is one of the most potent modifiers of cardiovascular risk factors yet studied in the incretin field, and it is simultaneously among the least proven in terms of cardiovascular outcomes. Both statements are true at once, and responsible interpretation holds them together rather than collapsing the second into the first.
Regulatory Status
The regulatory status of retatrutide is straightforward and unambiguous, and it frames everything above. As of mid-2026, retatrutide is investigational and is not approved by the FDA, the EMA, or any comparable regulatory authority for any indication, cardiovascular or otherwise.5 It exists legally only within the context of authorized clinical trials and controlled research.
The compound is advancing through a large phase 3 program (branded TRIUMPH by its developer) spanning obesity, type 2 diabetes, and related metabolic conditions, and phase 3 weight-loss readouts have been reported that broadly reinforce the potency signal seen earlier.5 Progress through phase 3 with positive weight-loss results is a necessary step toward eventual regulatory submission, but it is not the same as approval, and it is emphatically not the same as a demonstrated cardiovascular benefit. A regulatory submission and any subsequent approval for a weight or metabolic indication would still leave the cardiovascular-outcome question formally open until the dedicated outcomes trial reports.6
The cardiovascular outcomes trial (TRIUMPH-Outcomes) is the specific study that will ultimately determine whether the favorable risk-factor profile translates into fewer cardiovascular events. It is designed as a large, event-driven trial enrolling on the order of ten thousand participants with overweight or obesity and established cardiovascular disease, and by its nature it will run for several years until enough adjudicated events accumulate.6 Until it reports, no regulator has evaluated — and no evidence base supports — a cardiovascular-benefit claim for retatrutide.
For anyone encountering retatrutide, the regulatory reality carries direct practical implications. Because it is unapproved, any material available outside a clinical trial is not a regulated medicine; it has not been assessed for the manufacturing quality, labeling accuracy, and safety monitoring that approval requires. The favorable surrogate data discussed in this article were generated under trial conditions with clinical-grade compound and cardiovascular monitoring, and they cannot be assumed to apply outside that setting. The honest, evidence-cautious position is therefore that retatrutide’s cardiovascular-risk-factor profile is a promising but unproven area of active research, appropriate for scientific interest and continued study, and not a basis for any conclusion about cardiovascular treatment. Readers seeking additional context on how vial formats are described in a research reference framework can consult the 10 mg vial reconstitution reference.
Frequently Asked Questions
Does retatrutide lower blood pressure?
In phase 2 randomized trials, retatrutide was associated with dose-dependent reductions in systolic blood pressure — broadly in the range of about 4 to 8 mmHg at higher doses in the anchor obesity trial, and roughly 6.8 mmHg systolic in a pooled meta-analysis — along with smaller diastolic reductions.1,4 These are favorable surrogate-marker changes measured over up to 48 weeks, and much of the effect is plausibly linked to weight loss. They do not establish that retatrutide prevents strokes, heart attacks, or other blood-pressure-related events, which would require a completed cardiovascular outcomes trial.
Why does retatrutide raise heart rate?
The most likely explanation is its glucagon-receptor agonism. Glucagon has direct effects on the heart that can increase heart rate and cardiac output, and this arm is unique to retatrutide among the leading incretin agents. In phase 2 trials the increase was dose-dependent, broadly a few beats per minute up to roughly 6 to 7 bpm at higher doses, without a signal of increased arrhythmia over the study period — though the trials were too small and short to fully characterize this.1 The long-term significance of this heart-rate increase is a key open question for the ongoing outcomes trial.
Has retatrutide been proven to reduce heart attacks or strokes?
No. There is currently no completed cardiovascular outcomes trial for retatrutide. All cardiovascular data to date are surrogate risk-factor changes — blood pressure, lipids, glycemia, weight, heart rate — from mid-stage trials. A dedicated event-driven outcomes trial is underway but will take several years to report. Until then, no claim of proven cardiovascular event reduction is supported.6
How do retatrutide’s lipid effects compare with its effect on heart rate?
They pull in opposite directions, which is the central tension of its cardiovascular profile. Secondary analyses reported large favorable lipid changes — triglycerides down up to about 40 percent, non-HDL cholesterol down up to about 27 percent, and apolipoprotein B down up to about 24 percent — alongside reductions in atherogenic small LDL particles.3 At the same time, resting heart rate rose. The net cardiovascular balance of “many markers better, one worse” cannot be judged from surrogates and requires outcome data.
Is retatrutide FDA approved for cardiovascular disease or anything else?
No. As of mid-2026 retatrutide is investigational and not approved by the FDA, EMA, or any comparable regulator for any indication. It is advancing through phase 3 trials, but progress in trials is not approval, and no cardiovascular-benefit claim has been evaluated or authorized.5,6
Are the cardiovascular findings from retatrutide direct drug effects or a result of weight loss?
Both mechanisms are plausibly involved, and current studies cannot cleanly separate them. Retatrutide produces very large weight loss, and weight loss alone improves blood pressure, glycemia and lipids; the incretin and glucagon arms may also exert some direct effects on the vasculature, kidney and liver. Because the phase 2 trials were designed around weight loss, the cardiovascular risk-factor changes are entangled with the weight changes, and disentangling them would require dedicated study designs not yet completed.1
Why is unregulated retatrutide a concern for cardiovascular safety specifically?
Because the favorable risk-factor data were generated with precisely characterized clinical-grade compound, at defined doses, under medical supervision with cardiovascular monitoring — none of which applies to material obtained outside a clinical trial. Unapproved material has not passed regulatory manufacturing and quality controls, so its identity, purity and actual peptide content cannot be assumed. Given that the compound also raises heart rate, using uncharacterized material without monitoring compounds the uncertainty considerably. The trial data should not be read as endorsing any use outside a controlled clinical or laboratory research context.
When will we know whether retatrutide actually improves cardiovascular outcomes?
Only when the dedicated cardiovascular outcomes trial reports. It is an event-driven study enrolling roughly ten thousand higher-risk participants and must run until a pre-specified number of adjudicated cardiovascular events accrue, a process expected to take several years.6 Until that readout, the scientifically honest position is that retatrutide favorably changes cardiovascular risk factors but has not been shown to change cardiovascular outcomes.
References
- Jastreboff AM, Kaplan LM, Frías JP, et al. Triple–Hormone-Receptor Agonist Retatrutide for Obesity — A Phase 2 Trial. New England Journal of Medicine. 2023;389(6):514-526. NCT04881760. PubMed PMID: 37366315. Available at: https://www.nejm.org/doi/full/10.1056/NEJMoa2301972
- Sanyal AJ, Kaplan LM, Frias JP, et al. Triple hormone receptor agonist retatrutide for metabolic dysfunction-associated steatotic liver disease: a randomized phase 2a trial. Nature Medicine. 2024. PMC11271400. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC11271400/
- Triple-hormone receptor agonist retatrutide significantly improves lipoprotein and apolipoprotein profiles in participants with obesity or overweight (ESC Congress 2024 secondary analysis). European Heart Journal. 2024;45(Supplement_1):ehae666.1501. Available at: https://academic.oup.com/eurheartj/article/45/Supplement_1/ehae666.1501/7836502
- Effect of Retatrutide, a Novel Triple Receptor Agonist, on Blood Pressure and Lipid Levels: A Systematic Review and Meta-analysis of Randomized Controlled Trials. High Blood Pressure & Cardiovascular Prevention. 2026. PubMed PMID: 42371360. Available at: https://pubmed.ncbi.nlm.nih.gov/42371360/
- Retatrutide Phase 3 TRIUMPH program topline results (weight-loss readouts, 2025–2026). AJMC / Pharmaceutical Journal reporting on TRIUMPH-1 and related phase 3 trials. Available at: https://www.ajmc.com/view/retatrutide-achieves-up-to-30-3-average-weight-loss-in-phase-3-triumph-1-trial
- TRIUMPH-Outcomes: A cardiovascular outcomes trial of retatrutide in adults with overweight or obesity and established cardiovascular disease (ongoing, event-driven; ClinicalTrials.gov registration). Eli Lilly and Company.
- Coskun T, Urva S, Roell WC, et al. LY3437943, a novel triple glucagon, GIP, and GLP-1 receptor agonist for glycemic control and weight loss: From discovery to clinical proof of concept. Cell Metabolism. 2022;34(9):1234-1247. Available at: https://pubmed.ncbi.nlm.nih.gov/36070682/
Educational and research-use disclaimer: This article is provided strictly for educational and informational purposes and describes preclinical and early-phase research. Retatrutide is an investigational compound that is not approved by the FDA, EMA, or any comparable regulatory authority for any use. Nothing herein is medical advice, a treatment recommendation, or an endorsement of use in humans or animals outside of sanctioned clinical trials. All cardiovascular-related findings described are surrogate-marker or early-trial data; no cardiovascular outcome benefit has been established. Always consult a qualified healthcare professional and comply with all applicable laws and institutional requirements before handling any research compound.