Few research peptides carry a name as suggestive as DSIP — Delta Sleep-Inducing Peptide. The label promises exactly what many people search for: a molecule that switches on deep, slow-wave (delta) sleep. But a name is a hypothesis, not a verdict. The honest research question is narrower and harder: does Delta Sleep-Inducing Peptide actually improve sleep in a way that controlled science can reproduce, or is it a half-century-old riddle that has never been fully solved? This article walks through what DSIP is, how it was discovered, the mechanisms researchers have proposed, and—most importantly—what the actual human and animal evidence does and does not support, without inflating old, small, inconsistent data into proof it was never able to provide.
Educational and research context only. DSIP is not an approved drug in the United States or, to the best of available knowledge, anywhere else. Nothing here is medical advice, a treatment recommendation, or a human dosing protocol.
What is DSIP (Delta Sleep-Inducing Peptide)?
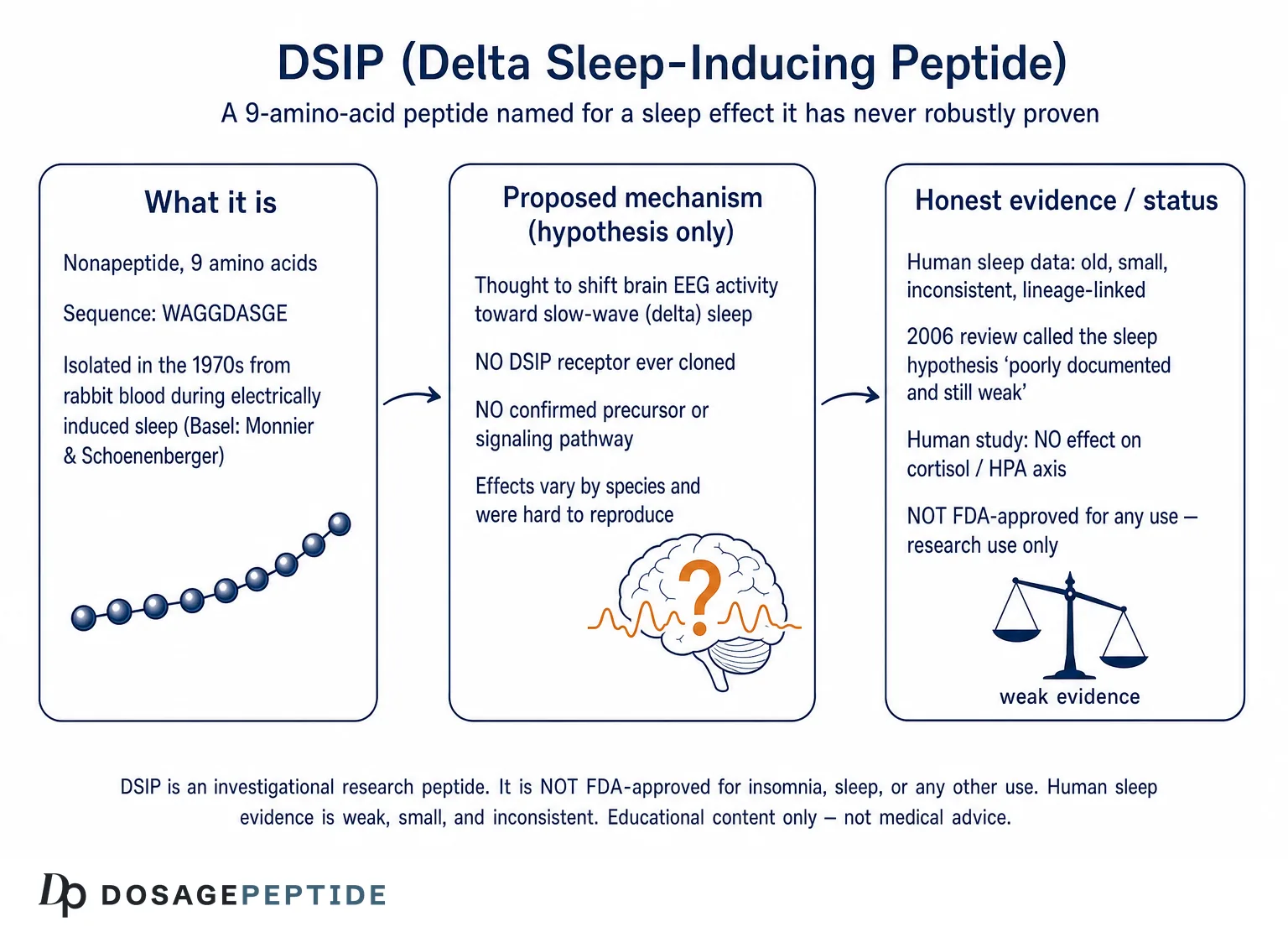
DSIP is a small, naturally occurring nonapeptide — a chain of nine amino acids — with the sequence Trp-Ala-Gly-Gly-Asp-Ala-Ser-Gly-Glu, usually written in single-letter code as WAGGDASGE.[1] Its molecular weight is roughly 849 daltons, which makes it a genuinely tiny signaling molecule compared with the large neuropeptides and hormones it is often grouped alongside.[3] The peptide is unusually simple in composition: it contains no sulfur-bearing residues, no aromatic residues beyond a single N-terminal tryptophan, and a run of small glycine and alanine residues that give it a flexible, largely unstructured backbone.
What makes DSIP scientifically distinctive is not its size but its origin story. It was not deduced from a gene or purified from a hormone-secreting gland. It was isolated from blood on the basis of a behavior — the appearance of delta waves on an electroencephalogram (EEG), the electrical signature of deep sleep. That functional definition is the source of both the peptide’s fame and its enduring controversy. To this day, decades after isolation, no specific DSIP receptor has been cloned, and no gene or precursor protein that produces DSIP has been definitively identified.[5] For a molecule named after a physiological effect, that is a striking and important gap, and it colors everything that follows.
If you are new to the vocabulary used throughout peptide research — terms like nonapeptide, half-life, blood-brain barrier, and slow-wave sleep — the peptide research glossary defines these plainly and is a useful companion to this article.
Where DSIP sits among neuropeptides
DSIP belongs to a loose category of “endogenous sleep factors” — substances the body was hypothesized to accumulate or release to promote sleep. Other candidates in that historical hunt included adenosine, prostaglandin D2, and various cytokines. Unlike adenosine, whose sleep-regulating role is now well established, DSIP’s status as a true physiological sleep factor was never confirmed to the same standard. It is more accurate to describe DSIP as a peptide isolated during sleep research than as a proven sleep hormone. That distinction is not pedantry; it is the entire crux of the evidence problem.
Chemistry, stability, and modified forms
The chemical simplicity of DSIP hides some real subtlety that matters for interpreting the research. The single aspartate residue in the sequence is prone to isomerization: the biologically active molecule is the alpha-aspartyl form, whereas the beta-aspartyl isomer that can form spontaneously is largely inactive, a distinction the Basel group established when they synthesized and tested the peptide.[2] This means a nominally “DSIP” sample can degrade toward an inactive species over time and under adverse storage conditions — a genuine complication for reproducibility, because two laboratories nominally studying the same peptide might be studying subtly different mixtures of active and inactive forms.
Researchers also described modified variants, most notably a phosphorylated form of DSIP (often abbreviated DSIP-P), phosphorylated on the serine residue, which was reported to have somewhat different properties and stability from the unphosphorylated parent. The existence of such naturally occurring modified forms complicated efforts to define a single “the” DSIP and to reconcile discordant results across studies.[5] When a research literature cannot fully agree on which molecular species is doing what, clean replication becomes correspondingly harder.
Where DSIP-like material shows up in the body
Early immunohistochemical and radioimmunoassay studies reported DSIP-like immunoreactive material distributed well beyond classic sleep centers — in various brain regions and in peripheral tissues — and reviewers took this broad distribution as a hint that DSIP, if physiologically real, might have functions extending past sleep into neuroendocrine and other roles.[3] The interpretive catch is that immunoreactivity is not the same as the intact, active peptide; antibodies can cross-react with fragments or related sequences. A widespread “DSIP-like” signal is consistent with a real, broadly distributed peptide, but it is equally consistent with the detection of assorted peptide fragments — another reason the peptide’s true endogenous identity stayed murky.
How was DSIP discovered?
The DSIP story begins in the 1960s and 1970s in Basel, Switzerland, with the physiologist Marcel Monnier and the biochemist Guido A. Schoenenberger. Monnier had spent years studying the electrical control of sleep, and he designed an elegant, now-classic experiment in rabbits. Using cross-circulation and dialysis techniques, he connected the cerebral circulation of a “donor” rabbit to a “recipient” rabbit. When the donor’s brain was driven into a sleep-like state by low-frequency electrical stimulation of the intralaminar thalamus, something in the donor’s cerebral venous blood, when transferred to the recipient, appeared to induce delta-wave EEG activity in the recipient as well. The implication was that a diffusible, blood-borne “humoral hypnogenic factor” was being generated during induced sleep.
Over years of painstaking fractionation, Schoenenberger and Monnier narrowed that activity down to a specific peptide. In 1977 they reported the characterization of a “delta-electroencephalogram (-sleep)-inducing peptide” in the Proceedings of the National Academy of Sciences, giving the amino acid sequence and showing that a synthetic version enhanced delta and spindle EEG patterns when infused into rabbit brain ventricles.[1] The following year, the Basel group published the detailed amino-acid analysis, sequence, chemical synthesis, and bioactivity of the nonapeptide as part of their long-running series on the peptide, confirming the WAGGDASGE structure and noting that only the correct alpha-aspartyl form — not its beta-aspartyl isomer — was highly active.[2]
The naming decision that shaped everything
It is worth pausing on how the peptide got its name, because the name has arguably done more marketing work than the data ever justified. The Basel group observed that their synthetic peptide enhanced delta-frequency EEG activity in a specific rabbit model. From that observation, the molecule was christened “delta sleep-inducing peptide.” The name encodes a strong causal claim — that the peptide induces delta sleep — on the basis of an experimental effect in one species under highly artificial infusion conditions. As later reviewers pointed out, the effect was modest, model-dependent, and difficult for other laboratories to reproduce consistently. The evocative name outran the evidence, and it has continued to do so in the decades since, especially in non-scientific and commercial contexts.
An animal-model peptide from the start
A crucial point that is easy to lose: DSIP was defined in animals, in an invasive infusion paradigm, using EEG endpoints rather than behavioral sleep or subjective sleep quality. Everything downstream — the mechanistic hypotheses, the human trials, the modern interest — is built on that preclinical foundation. Preclinical origin is not a disqualification (many important therapeutics started that way), but it does mean the burden of proof for human sleep benefit was never actually discharged at the outset. It had to be established later, and, as we will see, it largely was not.
A long series of papers, and a slow decline of interest
The DSIP work was not a single publication but an extended, numbered series from the Basel group spanning years, refining the isolation, sequence, synthesis, distribution, and bioactivity of the peptide — the 1978 nonapeptide paper, for instance, was formally the eleventh installment in that series.[2] Through the late 1970s and early 1980s, DSIP attracted considerable attention; the Graf and Kastin reviews of 1984 and 1986 catalogued a large and growing literature on both sleep and “extra-sleep” effects.[3][4] But interest in DSIP as a sleep factor waned over subsequent decades precisely because the central claim never firmed up. By the 2000s, reviewers were openly describing it as an unsolved puzzle rather than a validated sleep molecule — a trajectory that tells you something important about how the evidence held up under scrutiny.[5]
What is slow-wave (delta) sleep, and why does it matter here?
To judge whether DSIP earns its name, it helps to be clear about what “delta sleep” actually is. Human sleep cycles through non-REM (NREM) and REM stages roughly every 90 minutes. The deepest NREM stage — historically stages 3 and 4, now combined as N3 — is called slow-wave sleep (SWS) because the EEG is dominated by large, slow delta waves (about 0.5 to 4 Hz). This is the sleep most associated with physical restoration, and it is when the brain’s slow oscillations, sleep spindles, and the lowest levels of arousal converge.
SWS is also the stage where the stress axis is naturally quietest: during deep NREM sleep, hypothalamic drive to release cortisol falls to its daily low. That physiological coupling — deep sleep and low cortisol occurring together — is exactly why a peptide claimed to both deepen delta sleep and calm the HPA axis sounded so biologically attractive. The catch, as later sections show, is that the human data did not confirm the cortisol-lowering half of that appealing package.[9]
The reason the delta-versus-REM question matters for DSIP is that a molecule that genuinely and selectively deepens SWS would be therapeutically interesting in a way that a molecule which merely shuffles sleep stages around would not. As we will see, DSIP’s effects on sleep architecture were neither large nor consistent enough across species and studies to support the strong, selective “delta-inducing” claim its name makes.
Does DSIP actually increase delta (slow-wave) sleep?
This is the question the name promises to answer, so it deserves a direct look. “Delta sleep” refers to slow-wave sleep (SWS) — the deep, restorative stages of non-REM sleep dominated by high-amplitude, low-frequency (delta, roughly 0.5–4 Hz) EEG activity. In the original rabbit work, synthetic DSIP infused into the brain was reported to increase delta and spindle EEG patterns relative to control infusions, which is the finding that generated the name.[1]
But the picture became muddier as more species and laboratories were studied. Reviews of the DSIP literature noted that the peptide appeared to induce mainly delta-type sleep in rabbits, rats, and mice, yet in cats the more prominent effect was on REM sleep rather than delta sleep — an inconsistency that does not fit a clean “delta-inducing” story.[3] Effects varied with dose, timing relative to the light–dark cycle, route of administration, and the baseline state of the animal. In some paradigms DSIP looked hypnogenic; in others it looked like a mild modulator with no reliable sleep effect at all. This species- and context-dependence is a recurring theme and a major reason the peptide’s reputation eventually cooled within sleep neuroscience.
The problem of very small effects
Even where positive delta effects were reported, they tended to be modest in magnitude and statistically fragile given small sample sizes. A percentage increase in delta power in a handful of animals, in one lab, under one protocol, is a hypothesis-generating observation — not a robust demonstration that a molecule reliably deepens sleep. When the effect sizes are small and the number of independent replications is limited, the literature is exactly the kind that can look supportive in aggregate summaries while remaining unconvincing on close inspection.
What does the human sleep research on DSIP actually show?
Here is where honesty matters most, because the human DSIP sleep literature is old, small, methodologically limited, and inconsistent. The most-cited positive human work came from the same Basel-linked research lineage that discovered the peptide, which is a relevant consideration when weighing independence of evidence.
In 1981, Schneider-Helmert and Schoenenberger reported in Experientia that intravenous synthetic DSIP given to a small group of middle-aged chronic insomniacs was associated with longer sleep duration, fewer interruptions, and improved sleep quality, with the effect emerging in the second hour after injection; they concluded that DSIP had a “normalizing” influence on human sleep regulation.[6] A later study by Schneider-Helmert in European Neurology (1986) administered repeated intravenous DSIP over one week to 18 chronic psychophysiological insomniacs, split into middle-aged and elderly groups, and reported normalization of sleep parameters by the end of the investigation, with effects that appeared to correlate with the severity of baseline disturbance.[7]
Why this is weaker evidence than it sounds
Read quickly, those two studies sound like clinical validation. Read carefully, they illustrate why DSIP’s sleep claim never became established medicine:
- Tiny samples. We are talking about a handful to a couple of dozen participants — far too few to detect or exclude a modest effect reliably, and highly vulnerable to chance.
- Intravenous administration. The positive human data used intravenous DSIP under controlled conditions. That bears little resemblance to how the peptide is handled outside a clinic and says nothing about oral or subcutaneous use.
- Limited independence. Much of the supportive human work traces back to the group that discovered and championed the peptide. Independent replication by unaffiliated sleep laboratories was sparse and frequently unconvincing.
- Publication era and standards. These are studies from the early-to-mid 1980s, predating modern trial registration, pre-specified endpoints, and rigorous placebo-controlled crossover conventions now expected for sleep claims.
- Inconsistent replication. Other investigators studying DSIP in healthy sleepers and in insomnia did not consistently reproduce clear, clinically meaningful improvements, and the effects that did appear were often small and variable.
The verdict from within the field: a “still unresolved riddle”
The table below summarizes how the strength of evidence stacks up across the main claims made for DSIP — a useful antidote to write-ups that present every reported effect as if it carried equal weight.
| Claim | Main evidence type | Human data? | Honest strength |
|---|---|---|---|
| Increases delta / slow-wave sleep | Animal EEG (rabbit) + small human studies | Small, old, lineage-linked | Weak, inconsistent |
| Improves insomnia | A few small IV studies | Yes, but tiny samples | Weak, unreplicated |
| Lowers cortisol / calms HPA axis | Some animal work | Controlled human study: no effect | Unsupported in humans |
| Eases opioid / alcohol withdrawal | Uncontrolled case series | Yes, but no controls | Very weak (no RCTs) |
| Antioxidant / geroprotective | Animal & tissue models | No | Preclinical only, unrelated to sleep |
| Neuroprotection after injury | Rodent stroke model | No | Preclinical only |
Perhaps the most telling assessment comes from sleep neuroscience itself. In a 2006 review in the Journal of Neurochemistry pointedly titled “Delta sleep-inducing peptide (DSIP): a still unresolved riddle,” Kovalzon and Strekalova concluded that the hypothesis of DSIP as a genuine sleep factor was extremely poorly documented and remained weak, and that decades after isolation neither a receptor nor a definitive precursor had been established.[5] When a peer-reviewed review from within the discipline describes the core claim as “poorly documented and still weak” thirty years after discovery, that is the honest headline, and it should anchor expectations. For anyone examining a research-use DSIP handling and dosage reference for laboratory work, this evidentiary weakness is the single most important piece of context to carry along.
How might DSIP work? Proposed mechanisms of action
Because no DSIP receptor has been cloned and no signaling pathway has been definitively pinned down, every mechanism below should be read as a hypothesis supported by fragmentary and often preclinical data, not an established pathway. That caveat is not boilerplate; it is the literal state of the science.[5]
Direct action on sleep-related EEG activity
The founding hypothesis is that DSIP acts within central sleep-regulating circuits to shift EEG activity toward slow-wave (delta) frequencies. The rabbit infusion data are the anchor for this idea.[1] The difficulty is that no one has demonstrated a specific molecular target through which DSIP would produce this effect, and the cross-species inconsistency (delta in rodents, REM emphasis in cats) argues against a single, clean sleep-switch mechanism.[3]
Modulation of neuroendocrine and neurotransmitter systems
Some experimental work suggests DSIP can influence neuroendocrine signaling. In one rat study, DSIP inhibited somatostatin release from hypothalamic tissue in a concentration-dependent way, an effect blocked by the dopamine antagonist pimozide — implicating a dopaminergic mechanism in at least that particular action.[8] Findings like this indicate DSIP can touch multiple signaling systems in isolated tissue, but they do not add up to a coherent, sleep-specific pathway, and effects seen in excised hypothalamus do not automatically translate to whole-animal sleep behavior, let alone human sleep.
Stress-axis (HPA) modulation
A frequently repeated claim is that DSIP calms the hypothalamic-pituitary-adrenal (HPA) axis, lowering ACTH and cortisol and thereby easing stress-related sleep disruption. Some animal work is consistent with stress-buffering and corticosteroid-lowering effects. However, the human data directly undercut a simple version of this story. In a controlled human study, DSIP did not affect CRH-stimulated or meal-induced ACTH and cortisol secretion — responses during DSIP infusion were essentially identical to placebo.[9] This is a good example of a mechanism that looks promising in animal models and popular summaries but fails to hold up in the more relevant human context.
Antioxidant and cytoprotective activity
A separate body of largely Russian preclinical research attributes antioxidant and cytoprotective properties to DSIP. Experimental work describes DSIP suppressing lipid peroxidation, lowering malondialdehyde, and stimulating endogenous antioxidant enzymes such as superoxide dismutase and catalase, framing these as the basis of a “geroprotective” effect.[10] Whatever the merit of these observations, note that they describe general cellular stress-resistance mechanisms in animal and tissue models — they are not evidence that DSIP improves human sleep, and they should not be blurred together with the sleep question.
Thermoregulation and other physiological effects
DSIP has also been reported to influence thermoregulation, locomotor activity, heart rate, and blood pressure in animal experiments.[3] Because a small drop in core body temperature accompanies natural sleep onset, thermoregulatory effects are sometimes cited as an indirect route by which DSIP could favor sleep. This remains speculative and, again, rests on preclinical observations rather than demonstrated human sleep benefit.
What did DSIP research find on stress and the HPA axis?
Stress and sleep are tightly coupled, so the HPA-axis question deserves its own honest accounting. The animal literature contains reports that DSIP can blunt stress-induced corticosterone rises and help normalize disrupted corticosteroid rhythms, which is why DSIP is often described in popular writing as an “anti-stress” peptide. Reviews of the early literature catalogued a range of such “extra-sleep” effects alongside the sleep claims.[4]
The trouble is the translation to humans. The controlled human study cited above found no effect of DSIP on ACTH or cortisol secretion under either hormonal (CRH) or physiological (meal) stimulation.[9] Reviewers summarizing the field have similarly noted that where one human study suggested an effect on the adrenocortical axis, another found none — the classic signature of an unreliable, underpowered evidence base. The reasonable conclusion is that DSIP’s stress-axis effects are, at best, inconsistent in animals and largely unsupported in the human data that exist.
Could DSIP help with pain or drug and alcohol withdrawal?
Beyond sleep, one of the most-cited early clinical uses of DSIP was in managing withdrawal syndromes. In 1983, Dick, Grandjean, and Tissot reported in Neuropsychobiology that intravenous DSIP given to patients withdrawing from alcohol or opiates produced rapid, marked improvement in withdrawal symptoms, with an immediate onset of action, lasting suppression of somatic symptoms, and slower resolution of anxiety; they framed DSIP as having potential agonistic activity at opiate receptors.[11] This and similar reports are often quoted with impressive-sounding response rates.
Why the withdrawal data are not clinical proof
It is worth appreciating why the withdrawal setting is especially treacherous for uncontrolled research. Acute withdrawal from alcohol or opioids is a self-limiting process: symptoms peak and then subside over hours to days regardless of intervention. Patients are also highly suggestible in acute distress, and clinicians rating “improvement” without blinding will tend to see what they hope to see. Any treatment given during the natural downslope of withdrawal will look effective in an open-label design. This is exactly the scenario in which placebo and natural-history effects masquerade most convincingly as drug effects, which is why high reported “response rates” from such series carry so little evidentiary weight.
These withdrawal reports are best understood as uncontrolled case series from the 1980s. They generally lacked randomization, adequate blinding, and placebo controls; withdrawal symptoms fluctuate and improve on their own; and expectation effects are powerful in this setting. Impressive percentages of “improved” patients in an open-label series tell you very little about whether the peptide itself caused the improvement. The proposed opiate-receptor mechanism was also never firmly established. No large, rigorous, controlled trials converted these early observations into accepted therapy, and DSIP is not an approved treatment for withdrawal anywhere. It is a historically interesting signal, not a demonstrated clinical effect.
What about thermoregulation, chronobiology, and circadian timing?
Some of the more interesting DSIP research concerns timing rather than raw sleep-promotion. Because sleep is governed as much by circadian phase as by homeostatic sleep pressure, investigators explored whether DSIP might act on the timing of sleep. Early work examined DSIP in phase-shifted or circadian-disrupted insomnia, on the premise that the peptide might help realign disturbed sleep–wake schedules rather than simply sedate.
Combined with the thermoregulatory observations noted earlier — DSIP’s reported ability to modify body temperature, a variable tightly linked to circadian sleep gating — this paints DSIP less as a sedative and more as a putative modulator of sleep–wake regulation.[3] It is an appealing framing, and it is consistent with the peptide’s failure to behave like a straightforward hypnotic. But “appealing framing consistent with the data” is not the same as demonstrated efficacy. The chronobiological hypothesis, like the others, rests on small and dated studies and has not been established in rigorous modern trials.
DSIP beyond sleep: neuroprotection, antioxidant, and geroprotective research
A substantial share of the modern DSIP literature is not about sleep at all. It concerns the peptide’s reported cytoprotective effects in models of aging, oxidative stress, and injury — and it is important to keep this research mentally separate from the sleep question so the two are not conflated.
Aging and tumor-incidence models
In a long-term study in female SHR mice, monthly courses of a DSIP-containing preparation (“Deltaran”) were reported to slow some biomarkers of aging, reduce chromosome aberrations in bone marrow cells, increase maximum lifespan, and substantially lower spontaneous tumor incidence relative to controls.[12] A later report on the same Deltaran preparation described effects on longevity, physiological function, and carcinogenesis in mice.[13] These are intriguing animal findings from a specific research group, using a particular formulation, in a particular mouse strain — hypothesis-generating, not human evidence, and not about sleep.
Neuroprotection after injury
More recent work has examined DSIP in neurological injury. In a 2021 rat study, intranasal DSIP after focal stroke was associated with significantly better motor recovery on the rotarod test, although the reduction in infarct size did not reach statistical significance; the authors linked the benefit to possible neuroprotective, mitochondrial, and antioxidant mechanisms.[14] Again: a single-species preclinical result, useful for generating hypotheses about DSIP’s broader biology, but not evidence of a sleep benefit and not a clinical finding.
The reason to mention this non-sleep research at all is precisely to draw a boundary around it. Popular write-ups frequently stack up DSIP’s antioxidant, anti-tumor, and neuroprotective animal studies as if their sheer number strengthens the sleep case. It does not. A molecule can have real, reproducible effects on oxidative stress in mice and still not improve human sleep. These are different questions with different, largely non-overlapping evidence.
Why did DSIP’s sleep effects fail to replicate?
If DSIP were a reliable sleep-inducer, half a century of research should have nailed it down. Instead, the sleep claim faded from serious contention. Several interlocking reasons explain why.
No receptor, no precursor, no clear pathway
Sleep-active endogenous molecules that have stood the test of time (adenosine being the clearest example) come with identified receptors and defined signaling. DSIP has neither a cloned receptor nor a definitively identified biosynthetic precursor, despite decades of searching.[5] Without a target, it is hard to design mechanistically informed experiments, hard to predict dose–response relationships, and hard to explain why effects appear in one paradigm and vanish in another.
Small, heterogeneous, and lineage-linked studies
The supportive sleep studies were small, used varied species, doses, timings, and routes, and were disproportionately produced by the discovering research lineage. When independent groups applied the peptide under their own conditions, results were inconsistent. Heterogeneity plus small samples plus limited independent replication is a recipe for an evidence base that never converges.[3]
Debated endogenous role
It has never been firmly established that DSIP circulates and acts as a physiological sleep signal in intact animals. Some evidence suggested that if endogenous DSIP-like material exists, it may be bound to carrier proteins or embedded within larger precursor molecules whose identity remains unknown.[5] A molecule whose very existence as a free, active endogenous sleep factor is uncertain cannot easily be confirmed as one.
The name created a bias toward positive interpretation
Finally, the name itself — “delta sleep-inducing peptide” — primes everyone, including researchers and especially commercial marketers, to interpret ambiguous data charitably. A weakly positive or null result on a compound literally named for inducing sleep is more likely to be framed as “promising” than a null result on a neutrally named molecule. That framing bias helped keep the sleep narrative alive well past the point the data supported it.
What do we know about DSIP pharmacokinetics and blood-brain barrier penetration?
A recurring practical objection to DSIP as a sleep agent concerns pharmacokinetics. DSIP is a small, unmodified peptide, and small peptides are generally susceptible to rapid enzymatic degradation in blood and tissue. The reported biological half-life of DSIP in circulation is very short — on the order of minutes — which raises an obvious question: how could a molecule cleared that quickly produce sustained effects on an all-night process like sleep? Some human observations even described effects emerging in a delayed window (for example, in the second hour after injection), which is difficult to reconcile with a peptide that should already be largely degraded.[6]
This mismatch between a very short measured half-life and claims of overnight effects is one of the most under-discussed weaknesses in the popular DSIP narrative. Small linear peptides like DSIP are natural substrates for the peptidases that patrol blood and tissue, so rapid breakdown is the default expectation, not a surprise. If the intact peptide is gone within minutes, any explanation of a sustained sleep effect has to invoke something other than the continued presence of DSIP itself — a downstream trigger, a protected reservoir, or an active metabolite. None of those bridging mechanisms has been demonstrated to the standard that would let you say confidently how DSIP could produce a full night of deeper sleep.
Two hypotheses have been floated to bridge this gap. One is that DSIP acts as a trigger, initiating a downstream cascade that outlasts the peptide itself. The other is that endogenous DSIP-like material is protected from degradation by binding to a carrier protein or by existing within larger precursors, extending its functional life.[5] Both are plausible and both remain unproven. Blood-brain barrier penetration is a further open question: for a peripherally administered peptide to influence central sleep circuits, it must either cross the barrier in meaningful amounts or act through peripheral-to-central signaling, and the extent to which intact DSIP reaches sleep-regulating brain regions after systemic dosing is not well characterized. These pharmacokinetic uncertainties are not trivia; they are part of why the mechanism has never been convincingly closed.
How does DSIP compare to how other calming and nootropic peptides are studied?
Placing DSIP alongside other “calming” or neuroactive research peptides is instructive, because it highlights what a better-characterized (though still preclinical) peptide evidence base looks like. Consider two commonly discussed examples.
Selank, a synthetic analog of the immunomodulatory peptide tuftsin, has been studied with at least a proposed and partially investigated mechanistic framework — effects on GABAergic and monoaminergic signaling, brain-derived neurotrophic factor, and neuroinflammatory markers — giving researchers concrete pathways to probe. Semax, an ACTH(4–10) fragment analog, similarly has a body of work exploring BDNF, dopaminergic tone, and neuroprotective signaling. None of these peptides is FDA-approved, and their evidence bases are also dominated by animal work and small studies; they are not held up here as proven therapies. But the contrast with DSIP is real: DSIP is unusual in having a strong name and a famous discovery story while lacking the identified receptor and coherent pathway that would let researchers systematically test its central claim.
There is also a methodological contrast worth naming. Selank and Semax research, for all its limitations, has increasingly used defined behavioral models, molecular markers, and mechanistic readouts that let a hypothesis be tested and potentially falsified. Much of the classic DSIP sleep literature, by contrast, leaned on a small number of paradigms in a small number of hands, with endpoints (delta-power changes in a specific rabbit infusion model) that were difficult for outsiders to reproduce. A field advances when independent groups can take a claim, run their own version, and either confirm or kill it. DSIP’s sleep claim never fully entered that self-correcting cycle, which is part of why it neither triumphed nor was cleanly refuted — it simply lingered.
The broader lesson is a methodological one that applies to the entire research-peptide space. Discovery hype, an evocative name, and a scattering of positive early reports are not the same as a reproducible, mechanistically grounded effect. DSIP is a cautionary example of how a compelling story can carry a molecule for decades on thin data. When you encounter confident claims about any research peptide — DSIP included — the questions to ask are simple: Is there an identified target? Have independent groups reproduced the effect? Is the human evidence more than a handful of small, old studies? For DSIP’s sleep claim, the answers are, respectively, no, largely no, and no.
Is DSIP approved, and how is it handled in research?
DSIP is not an approved drug. It has no FDA approval for insomnia, sleep, withdrawal, or any other indication, and it is not, to the best of available knowledge, an approved medicine in any jurisdiction. It exists as a synthetic peptide used in laboratory and experimental settings, and any material sold is intended for research use, not human therapeutic use. There is no established, validated human dose, no long-term human safety dataset from controlled trials, and no regulatory quality assurance behind research-grade material.
Why “research use only” is a meaningful limitation
The absence of approval is not a technicality to be waved away. It means that purity, identity, sterility, and content of research-grade DSIP are not guaranteed to pharmaceutical standards; that the safety profile of repeated administration in humans has not been characterized in rigorous trials; and that there is no authoritative guidance on interactions, contraindications, or long-term effects. In peptide research, correct identity and handling — reconstitution, sterility, storage, and accurate concentration — are foundational for any experiment to mean anything. Laboratories working with lyophilized peptides typically consult a peptide reconstitution guide and a reconstitution and dosage calculator to convert vial contents into accurate working concentrations, precisely because sloppy handling is a common source of unreliable data. Compound-specific handling notes, such as a DSIP vial reference, exist for the same reason: to keep the mechanics of a research protocol consistent. None of that infrastructure, however, changes the core scientific reality: the evidence that DSIP improves human sleep is weak, and no amount of careful measurement can manufacture an effect the underlying data do not robustly show.
What is and isn’t known about safety
The early human studies generally reported that intravenous DSIP was well tolerated over short exposures, with few obvious acute adverse effects noted in those small samples.[11] That limited historical tolerability is not equivalent to an established safety profile. Small, short, dated studies cannot detect uncommon adverse events, drug interactions, or consequences of repeated long-term exposure. Absence of documented harm in a few dozen people is not evidence of safety at scale.
The honest bottom line: what the research actually shows
Stripped of marketing and the seductive name, here is what the DSIP literature supports:
- DSIP is real and well-characterized as a molecule. The nonapeptide WAGGDASGE was genuinely isolated during rigorous sleep-physiology experiments and its structure and synthesis are solid.[1][2]
- The core sleep claim is weak. Human sleep evidence is old, small, inconsistent, and largely lineage-linked; independent replication is poor; and a within-field review flatly called the sleep hypothesis “poorly documented and still weak.”[5]
- Mechanisms are hypotheses. No receptor, no confirmed precursor, no closed pathway; the HPA-axis story in particular failed in controlled human testing.[9]
- Non-sleep effects are a separate story. Antioxidant, geroprotective, and neuroprotective findings exist in animal models but say nothing about human sleep and should not be used to prop up the sleep claim.[10]
- It is not approved and not proven. DSIP is an investigational research peptide with no regulatory approval and no rigorous long-term human safety data.
If there is a single sentence to take away, it is this: DSIP is a molecule whose reputation was set by its name and its dramatic discovery story, not by a body of reproducible evidence that it improves sleep. The intellectually honest position is that DSIP is a fascinating, unresolved chapter in sleep neuroscience — a molecule that earned an ambitious name it has never quite lived up to. It is a legitimate subject of continued research, especially given the intriguing preclinical work on cellular protection and injury. It is not a demonstrated sleep therapy. Anyone evaluating DSIP for laboratory research should treat the sleep-benefit narrative with appropriate skepticism and let the actual evidence — small, dated, and inconsistent — set the expectation. For those conducting formal research who need accurate handling and measurement information for the compound, the DSIP research reference and handling guide is the appropriate resource, always used strictly within a research-only, non-therapeutic framework and alongside the honest evidence picture laid out above.
Frequently Asked Questions
Does DSIP actually make you sleep better?
The evidence that DSIP reliably improves human sleep is weak. A few small, dated studies — mostly from the research lineage that discovered the peptide — reported benefits, but samples were tiny, administration was intravenous, and independent replication was poor. A 2006 review in the Journal of Neurochemistry described the sleep hypothesis as poorly documented and still weak. DSIP is not a proven sleep aid, and it is not an approved treatment for insomnia.
What does DSIP stand for and what is it?
DSIP stands for Delta Sleep-Inducing Peptide. It is a small, naturally occurring nonapeptide (nine amino acids, sequence WAGGDASGE) first isolated in the 1970s by Schoenenberger and Monnier from the cerebral venous blood of rabbits during electrically induced sleep. It was named for its reported ability to enhance delta-wave (slow-wave) EEG activity in that specific animal model, though that causal claim has never been robustly confirmed in humans.
Is DSIP FDA-approved or safe to use?
No. DSIP is not approved by the FDA or, to the best of available knowledge, by any regulator, for sleep or any other use. It is handled as a research-only peptide. Early small studies reported short-term intravenous tolerability, but there is no rigorous long-term human safety data, no validated human dose, and no regulatory quality assurance for research-grade material. Limited historical tolerability is not the same as an established safety profile.
How was DSIP discovered?
In cross-circulation experiments, Marcel Monnier found that blood from rabbits in an electrically induced sleep state could promote delta-wave EEG activity when transferred to other rabbits, suggesting a diffusible sleep factor. Guido Schoenenberger’s group isolated and sequenced the responsible peptide, publishing its characterization in PNAS in 1977 and its full synthesis and activity in 1978.
Why has no DSIP receptor been found?
Despite decades of research, no specific DSIP receptor has been cloned and no definitive biosynthetic precursor identified. This is one of the peptide’s central unresolved problems: a molecule named for a physiological effect but lacking a known molecular target. The absence of a receptor makes it difficult to design mechanistically informed studies and helps explain why effects appear inconsistently across species and paradigms.
Was DSIP ever used for drug or alcohol withdrawal?
Early-1980s reports, including a 1983 Neuropsychobiology study, described rapid improvement of alcohol and opiate withdrawal symptoms after intravenous DSIP, proposing possible opiate-receptor activity. However, these were uncontrolled case series without randomization or placebo controls, and withdrawal symptoms fluctuate and remit on their own. No rigorous controlled trials confirmed the effect, and DSIP is not an approved withdrawal treatment.
How is DSIP different from a sleeping pill?
Conventional hypnotics have identified molecular targets (for example, GABA-A receptors), established pharmacology, regulatory approval, and controlled-trial evidence. DSIP has none of these: no confirmed receptor, no proven pathway, no approval, and only weak, inconsistent sleep data. It behaves less like a reliable sedative and more like a putative, unproven modulator of sleep–wake regulation, which is part of why it never became an accepted therapy.
Does DSIP lower cortisol and stress?
Some animal studies suggest DSIP can blunt stress-induced corticosteroid rises, but the human data are unsupportive. In a controlled human study, DSIP had no effect on CRH-stimulated or meal-induced ACTH and cortisol secretion, with responses essentially identical to placebo. The “anti-stress” framing rests largely on preclinical work that did not translate to humans, so it should be treated with caution.
References
- Schoenenberger GA, Monnier M. Characterization of a delta-electroencephalogram (-sleep)-inducing peptide. Proc Natl Acad Sci USA. 1977;74(3):1282–1286.
- Schoenenberger GA, Maier PF, Tobler HJ, Wilson K, Monnier M. The delta EEG (sleep)-inducing peptide (DSIP). XI. Amino-acid analysis, sequence, synthesis and activity of the nonapeptide. Pflugers Arch. 1978;376(2):119–129.
- Graf MV, Kastin AJ. Delta-sleep-inducing peptide (DSIP): a review. Neurosci Biobehav Rev. 1984;8(1):83–93.
- Graf MV, Kastin AJ. Delta-sleep-inducing peptide (DSIP): an update. Peptides. 1986.
- Kovalzon VM, Strekalova TV. Delta sleep-inducing peptide (DSIP): a still unresolved riddle. J Neurochem. 2006;97(2):303–309.
- Schneider-Helmert D, Schoenenberger GA. The influence of synthetic DSIP (delta-sleep-inducing-peptide) on disturbed human sleep. Experientia. 1981;37(9):913–917.
- Schneider-Helmert D. Efficacy of DSIP to normalize sleep in middle-aged and elderly chronic insomniacs. Eur Neurol. 1986;25(6):448–453.
- Iyer KS, McCann SM. Delta sleep inducing peptide inhibits somatostatin release via a dopaminergic mechanism. Neuroendocrinology. 1987;46(1):93–95.
- Späth-Schwalbe E, Schäfer A, Uthgenannt D, Born J, Fehm HL. Delta-sleep-inducing peptide does not affect CRH and meal-induced ACTH and cortisol secretion. Psychoneuroendocrinology. 1995.
- Bondarenko TI, Maïboroda EA, Mikhaleva II, Prudchenko IA. Mechanism of delta-sleep inducing peptide geroprotective activity. Adv Gerontol. 2011;24(1):80–92.
- Dick P, Grandjean ME, Tissot R. Successful treatment of withdrawal symptoms with delta sleep-inducing peptide, a neuropeptide with potential agonistic activity on opiate receptors. Neuropsychobiology. 1983;10(4):205–208.
- Popovich IG, et al. Effect of delta-sleep inducing peptide-containing preparation Deltaran on biomarkers of aging, life span and spontaneous tumor incidence in female SHR mice. Mech Ageing Dev. 2003.
- Voïtenkov VB, Popovich IG, Zabezhinskiï MA, et al. Effect of delta-sleep inducing peptide preparation Deltaran on longevity, physiological functions, and carcinogenesis in mice. Adv Gerontol. 2009;22(4):646–654.
- Tukhovskaya EA, Ismailova AM, Shaykhutdinova ER, et al. Delta Sleep-Inducing Peptide Recovers Motor Function in SD Rats after Focal Stroke. Molecules. 2021;26(17):5173.