Walk into any supplement aisle or scroll any research-peptide catalog and you will meet vitamin B12 wearing at least four different chemical costumes: cyanocobalamin, methylcobalamin, hydroxocobalamin, and adenosylcobalamin. Marketing copy tends to divide these into a tidy morality tale — the “natural, active, superior” methylcobalamin versus the “synthetic, cyanide-containing, inferior” cyanocobalamin. The underlying biochemistry, and the clinical trial record that actually tests these forms head-to-head, tell a considerably more nuanced story. This article works through the chemistry of the four cobalamins, which enzymes each one serves, how they are absorbed, converted, retained, and excreted, what the cyanide question really amounts to in context, and whether the form you choose meaningfully changes the biological outcome for most purposes.
Throughout, the framing is educational and research-oriented rather than medical advice. Vitamin B12 in its injectable and oral forms is used in clinical medicine to correct a well-defined deficiency; nothing here is a recommendation to self-treat, and dosing or diagnosis decisions belong with a qualified clinician. What we can do rigorously is separate what the evidence supports from what the marketing asserts.
What is vitamin B12 and why does its chemical form matter at all?
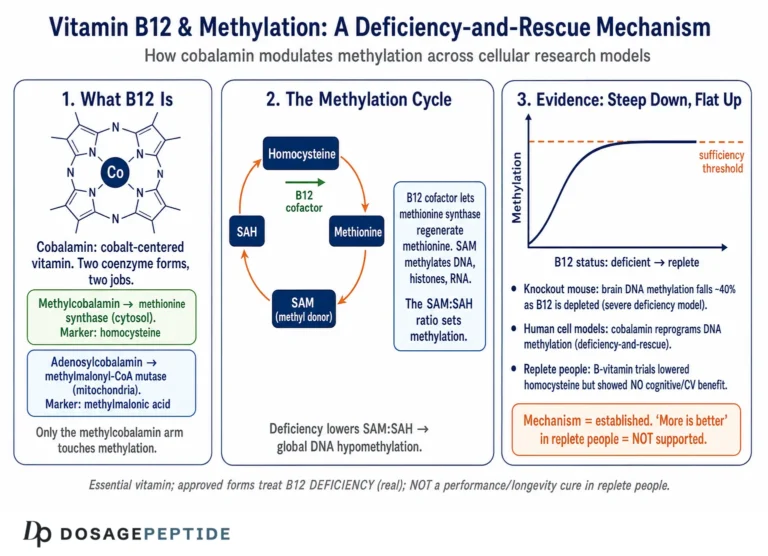
Vitamin B12 is the collective name for a family of large, cobalt-containing molecules called cobalamins. The core structure is a corrin ring — a modified porphyrin-like macrocycle — with a cobalt atom held at its center. Below the cobalt sits a dimethylbenzimidazole nucleotide “tail.” Above the cobalt is a variable position, the so-called upper axial ligand or “beta” position, and it is entirely this single attachment point that distinguishes the four forms from one another. Attach a cyanide group and you have cyanocobalamin; a methyl group gives methylcobalamin; a hydroxyl group gives hydroxocobalamin; and a 5′-deoxyadenosyl group gives adenosylcobalamin.[1]
Only two of these are biologically active coenzymes inside human cells: methylcobalamin and adenosylcobalamin. Cyanocobalamin and hydroxocobalamin are best understood as precursor or “storage/transport-friendly” forms that the body converts into the two active coenzymes. That single fact — that the body interconverts these molecules through a shared processing pathway — is the pivot on which the entire “which form is best” debate turns, and we will return to it repeatedly.
Vitamin B12 cannot be synthesized by plants or animals; it is produced only by certain bacteria and archaea, which is why the vitamin ultimately enters the human food chain through animal products and microbial fermentation. Because human requirements are tiny (measured in micrograms) but the consequences of deficiency are severe — megaloblastic anemia and potentially irreversible neurological injury — the vitamin occupies an outsized place in both clinical medicine and the supplement market.[2]
It is worth pausing on why cobalamin is structurally so unusual, because that unusualness is what gives the different forms their distinct behavior. The corrin ring is one of the most complex small-molecule cofactors in all of biology — its biosynthesis by microbes requires around thirty enzymatic steps — and at its heart is a cobalt–carbon bond in the two active coenzymes. The cobalt–carbon bond (cobalt to the methyl group in methylcobalamin, cobalt to the deoxyadenosyl carbon in adenosylcobalamin) is one of only a handful of naturally occurring organometallic bonds in human biochemistry. This bond is what the coenzymes exploit: methionine synthase transfers the entire methyl group off methylcobalamin’s cobalt, while methylmalonyl-CoA mutase homolytically cleaves adenosylcobalamin’s cobalt–carbon bond to generate a highly reactive radical that drives its rearrangement chemistry. The upper ligand is therefore not a cosmetic label; it defines whether the molecule can perform chemistry at all, and how fragile that chemistry is.
The four forms also differ in a property people rarely think about: their oxidation and reactivity. The cobalt atom can sit in three oxidation states — Co(III), Co(II), and the powerfully nucleophilic Co(I) — and cobalamin’s ability to cycle through these states is what lets it participate in both methyl-transfer and radical chemistry. Cyanocobalamin holds cobalt firmly in the Co(III) state with a tightly bound, electron-withdrawing cyanide, which is precisely why it is so stable and so inert until the cell reduces it. The active coenzymes, by contrast, must be reactive to do their jobs, and reactivity is the enemy of shelf stability — a trade-off that runs through the entire comparison.
The two jobs B12 actually does in the body
For all the complexity of its chemistry, cobalamin has exactly two enzymatic jobs in human physiology, and understanding them explains why two active forms exist rather than one.
The first job takes place in the cytoplasm. Methylcobalamin is the coenzyme for methionine synthase, the enzyme that transfers a methyl group from 5-methyltetrahydrofolate to homocysteine, regenerating methionine and tetrahydrofolate.[3] This reaction sits at the crossroads of the folate cycle and the methylation cycle. Methionine is the precursor of S-adenosylmethionine (SAM), the universal methyl donor for DNA, RNA, proteins, phospholipids, and neurotransmitters. When methionine synthase stalls for lack of B12, homocysteine accumulates (a marker of deficiency), folate becomes trapped in its methyl form (the “methyl-folate trap,” which explains why B12 deficiency produces a folate-responsive-looking anemia), and methylation reactions throughout the body are throttled.
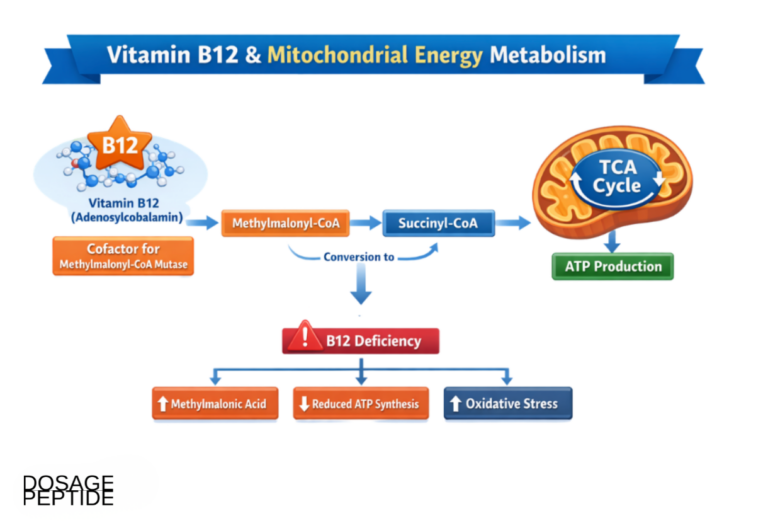
The second job takes place in the mitochondria. Adenosylcobalamin is the coenzyme for methylmalonyl-CoA mutase, which rearranges methylmalonyl-CoA into succinyl-CoA.[4] This step is essential for metabolizing the products of certain amino acids (isoleucine, valine, methionine, threonine) and odd-chain fatty acids, feeding their carbon skeletons into the citric acid cycle. When this enzyme lacks adenosylcobalamin, methylmalonic acid (MMA) accumulates — which is precisely why serum or urinary MMA is the most specific laboratory marker of true cobalamin deficiency.[2]
So the body needs methylcobalamin for one reaction and adenosylcobalamin for the other. Neither cyanocobalamin nor hydroxocobalamin directly participates in either reaction. Instead, whatever form enters the cell is stripped of its upper ligand and rebuilt into whichever coenzyme is needed, where it is needed. Any honest comparison of B12 forms has to reckon with this: the cell is going to remodel the molecule regardless of which version you supply.
How do the four cobalamin forms differ chemically?
Each form is defined by that upper axial ligand, but the ligand also confers distinct physical and pharmacological properties — stability, color, light sensitivity, and how tightly the molecule holds together in solution.
| Form | Upper ligand | Status in the body | Key property | Typical use |
|---|---|---|---|---|
| Cyanocobalamin (CNCbl) | Cyanide (–CN) | Synthetic precursor; not a natural coenzyme | Most chemically stable; best studied | Oral supplements, injectable deficiency correction, food fortification |
| Methylcobalamin (MeCbl) | Methyl (–CH₃) | Active coenzyme for methionine synthase | Light-sensitive; converts to hydroxocobalamin on exposure | Oral/sublingual supplements, injectables in some countries |
| Hydroxocobalamin (OHCbl) | Hydroxyl (–OH) | Natural transport/storage form; not a coenzyme itself | Very stable; longest plasma retention; binds cyanide avidly | Injectable deficiency treatment; high-dose cyanide-poisoning antidote |
| Adenosylcobalamin (AdoCbl) | 5′-deoxyadenosyl | Active coenzyme for methylmalonyl-CoA mutase | Light-sensitive; the dominant intracellular storage coenzyme | Some combination “active B12” supplements |
Cyanocobalamin: the synthetic workhorse
Cyanocobalamin is the form you are most likely to encounter, and it exists in medicine and supplements for a specific reason: it is the most stable and the most extensively characterized cobalamin. The cyanide ligand binds cobalt tightly, making the molecule resistant to light and oxidative degradation relative to the other forms, which is why it is the standard for pharmaceutical manufacturing and food fortification.[6]
Cyanocobalamin does not occur meaningfully in nature; it is largely an artifact of the purification process (cyanide was historically used to extract and crystallize the vitamin, and cobalamins scavenge trace cyanide readily). Because it is not a coenzyme, cyanocobalamin must be de-cyanated inside the cell and then converted to methylcobalamin and adenosylcobalamin before it does any metabolic work.[5] This extra step is real, but as we will see it is a step the cell performs routinely and efficiently.
Methylcobalamin: the active methylation coenzyme
Methylcobalamin is one of the two forms that actually functions as a coenzyme, driving methionine synthase and therefore the remethylation of homocysteine. This is the biochemical basis for its “active form” branding. The important caveat is that methylcobalamin is chemically fragile: it is light-sensitive and converts spontaneously to hydroxocobalamin at room temperature in solution when exposed to white light, even in protected conditions over time.[6] Its status as the “active” form is genuine at the enzyme level, but that does not automatically translate to superiority as a supplement, because supplemented methylcobalamin still undergoes intracellular processing rather than plugging directly into the enzyme intact.
Hydroxocobalamin: the long-acting natural form
Hydroxocobalamin is the form closest to what circulates and is stored in the body. It is not itself an enzyme cofactor, but it is a natural transport/storage species, it is highly stable, and — crucially — it is retained in plasma far longer than cyanocobalamin after injection.[7] That extended retention is why hydroxocobalamin is the preferred injectable in much of Europe: fewer injections are needed to maintain status. Hydroxocobalamin also has a second, entirely separate clinical identity as a high-dose intravenous antidote for cyanide poisoning, which we discuss below.
Adenosylcobalamin: the mitochondrial coenzyme
Adenosylcobalamin is the second active coenzyme, serving methylmalonyl-CoA mutase in the mitochondria, and it is actually the predominant form of stored cobalamin in human tissues such as the liver. Like methylcobalamin, it is light-sensitive and readily converts to hydroxocobalamin on exposure to light.[6] Adenosylcobalamin appears in some “active B12” or “dibencozide” supplements, sometimes paired with methylcobalamin on the logic that supplying both active coenzymes covers both enzymatic jobs. Whether that logic holds up against the interconversion evidence is the central question of this article.
Which enzymes does each form actually serve?
The marketing shorthand — “methylcobalamin for the brain, adenosylcobalamin for energy” — maps loosely onto the two enzymes but oversimplifies what happens after you swallow or inject any form of the vitamin. The decisive point, established by cobalamin biochemistry, is that the cell does not use whichever form you deliver as-is. Instead, essentially all incoming cobalamin funnels through a single intracellular processing hub.
The MMACHC processing hub
Once cobalamin enters a cell (delivered on the transport protein transcobalamin and released from lysosomes), a cytosolic protein called MMACHC (the CblC protein) acts as a universal “gatekeeper.” It removes whatever upper ligand the incoming molecule carries. According to the mechanistic review by Obeid and colleagues, MMACHC performs flavin-dependent decyanation of cyanocobalamin, glutathione-dependent dealkylation of methylcobalamin and adenosylcobalamin, and handles hydroxocobalamin through reduction — and all of these routes converge on the same intermediate, a reduced cob(II)alamin.[7]
From that common cob(II)alamin intermediate, the cell then builds methylcobalamin in the cytoplasm (for methionine synthase) or transports the cobalamin into mitochondria and builds adenosylcobalamin (for methylmalonyl-CoA mutase). In other words, the methyl group you paid extra for on a methylcobalamin supplement is stripped off, and a new methyl group is attached at the point of use — and the same is true for the adenosyl group on adenosylcobalamin. The cell manufactures the coenzyme it needs, when and where it needs it, from a stripped-down common precursor.
This is why the elaborate “which form feeds which enzyme” framing collapses under scrutiny. Supplying methylcobalamin does not preferentially load methionine synthase, and supplying adenosylcobalamin does not preferentially load the mutase, because both are dismantled to the same intermediate before being rebuilt. The Obeid review states the implication directly: because the active forms follow the same intracellular processing route as cyanocobalamin, supplementing methylcobalamin or adenosylcobalamin is unlikely to be advantageous compared with cyanocobalamin.[8]
What this means for the “active form is better” claim
The claim that active forms are inherently superior rests on an intuitive but flawed assumption: that a supplement molecule slots directly into the target enzyme. It does not. There is no cellular shortcut by which oral methylcobalamin bypasses MMACHC and hands its methyl group straight to methionine synthase. Recognizing this dissolves most of the theoretical case for active-form superiority. What remains — and it is a legitimate remaining question — is whether differences in absorption, plasma retention, or excretion between forms produce a practical difference in how much cobalamin ultimately reaches tissues. That is an empirical question, and the evidence there is genuinely mixed, which we turn to next.
A telling natural experiment: inherited processing defects
Human genetics provides an unintended experiment that reinforces just how central the MMACHC hub is. There is a family of inborn errors of cobalamin metabolism, labeled cblA through cblG and cblJ, each caused by a defect in a specific step of intracellular cobalamin handling. The cblC disorder — a defect in MMACHC, the very gatekeeper protein that removes upper ligands — is the most common of these and produces combined elevation of both homocysteine and methylmalonic acid, because the cell cannot generate either active coenzyme. The clinically important point for the forms debate is this: children with cblC defects respond to hydroxocobalamin, not to a diet or supplement richer in “active” forms, because the problem is downstream of ingestion. If pre-formed methylcobalamin or adenosylcobalamin could simply bypass the processing machinery, these disorders would be trivially treatable by feeding the active coenzymes — and they are not. That real-world observation is among the strongest lines of evidence that supplemented active forms do not skip the shared processing route.[7]
How is vitamin B12 absorbed, and does the form change that?
To evaluate absorption differences, you first need the normal physiology. B12 absorption is one of the more elaborate processes in human nutrition, involving multiple binding proteins and a specific receptor in the distal small intestine.
The intrinsic-factor pathway
Dietary B12, bound to food protein, is released by stomach acid and pepsin and initially picked up by haptocorrin (R-protein) in saliva and gastric juice. In the duodenum, pancreatic enzymes degrade haptocorrin, transferring cobalamin to intrinsic factor (IF), a glycoprotein secreted by gastric parietal cells. The IF–B12 complex travels to the terminal ileum, where it binds the cubam receptor, is internalized, and the cobalamin is eventually released and loaded onto transcobalamin for delivery to tissues.[1]
This IF-dependent route is efficient but saturable: a single physiological dose absorbs only a couple of micrograms at most, regardless of how much more is present. It is also the route that fails in pernicious anemia (autoimmune loss of intrinsic factor), after gastrectomy or ileal resection, and to varying degrees with the atrophic gastritis and acid-suppressing medication use common in older adults.
The passive-diffusion pathway and why high oral doses work
Alongside the IF route, roughly 1% of an oral dose is absorbed by simple passive diffusion across the intestinal mucosa, and this pathway is independent of intrinsic factor.[9] This is the entire basis for high-dose oral therapy: if you give 1,000–2,000 µg orally, then even 1% passive absorption delivers 10–20 µg — far more than the roughly 2–4 µg daily requirement — which is why high-dose oral B12 can maintain and even correct deficiency in many patients who lack intrinsic factor entirely.
Critically, the passive-diffusion route does not depend on the upper axial ligand. Whether the molecule is cyanocobalamin or methylcobalamin, the corrin core diffuses across the mucosa similarly. Any difference in oral bioavailability between forms is therefore likely to be modest and is not driven by a fundamental difference in the absorption mechanism.
What head-to-head absorption studies show
The direct comparative data are limited and not entirely consistent. Some absorption measurements suggest cyanocobalamin is taken up slightly more efficiently at the point of ingestion than methylcobalamin, with reported figures on the order of roughly 49% versus 44% at low doses in some studies — a small difference. Reviews consistently caution that between-form differences in bioavailability at typical supplement doses are small and may be clinically insignificant, and that host factors such as age, genetics, and gut health dominate the outcome far more than the choice of ligand.[10]
The Obeid review adds an important honest caveat: rigorous data comparing low doses (≤10 µg) of the different forms for absorption, bioavailability, and intracellular processing are simply sparse, so confident claims of superiority in either direction outrun the evidence.[7]
Why the absorption ceiling matters more than the ligand
There is a structural reason to expect the form to be a minor variable in oral supplementation: the intrinsic-factor route saturates at a low ceiling. Because IF-mediated uptake absorbs only on the order of 1.5–2 µg from a single dose no matter how much you take, the incremental cobalamin from a large oral tablet comes overwhelmingly from the ligand-indifferent passive-diffusion route. This has two consequences. First, splitting a daily requirement across the day (or taking B12 with food) can slightly improve total uptake through the saturable route, which is a dosing-schedule effect that dwarfs any ligand difference. Second, once you move to the high-dose oral or injectable regimens used to actually treat deficiency, you are working almost entirely in the passive/parenteral regime where the corrin core — identical across all four forms — is what crosses the barrier. The practical takeaway is that whether a product is cyanocobalamin or methylcobalamin is a smaller lever on your B12 status than whether you took an adequate dose, took it consistently, and had a functioning absorption pathway.
Food B12, fortification, and the pseudovitamin problem
A related point that the form debate often ignores is the difference between true cobalamin and inactive “analogues.” Some foods and supplements — notably many algae products such as spirulina — contain corrinoids that resemble B12 on some assays but are biologically inactive in humans; these are collectively called pseudovitamin B12. Laboratory work has shown that pseudovitamin B12 does not effectively support the cobalamin-dependent enzymes methylmalonyl-CoA mutase and methionine synthase in mammalian cells, which is why relying on such sources can leave a person deficient despite apparently “adequate” intake.[4] This reframes the whole question usefully: the distinction that genuinely determines biological activity is not cyanocobalamin-versus-methylcobalamin (both are true, active-in-vivo cobalamins) but true cobalamin versus inactive analogue. For food-fortification and supplementation, cyanocobalamin is the workhorse specifically because it is a stable, unambiguously bioavailable true cobalamin — a far more important property than which upper ligand it happens to carry.
Do the forms differ in retention and excretion?
If absorption is roughly comparable, the next question is what happens to the vitamin after it enters the circulation. Here the forms genuinely differ, and this is the strongest evidence-based argument that form can matter — though mostly in the injectable, not the oral, context.
The retention argument for methylcobalamin
The claim that methylcobalamin is “better retained” traces largely to older work, notably a 1973 study by Okuda and colleagues in the Journal of Laboratory and Clinical Medicine, which reported that after administration of methylcobalamin more radioactivity accumulated in the liver over eight hours than with cyanocobalamin, consistent with gradual tissue conversion and retention of the methyl form, and that cyanocobalamin was cleared in the urine more readily.[11] The comparative review by Obeid and colleagues summarizes this same body of retention data, noting that the body tends to retain methylcobalamin somewhat better while cyanocobalamin is more readily excreted, but treats it as of uncertain clinical importance.[7]
These retention differences are real but should be kept in proportion. They are measured against a backdrop in which B12 has no established upper tolerable intake level precisely because the body excretes what it does not need, and because it has substantial hepatic stores (enough to buffer deficiency for years). A somewhat higher urinary loss of an abundant, non-toxic, well-stored vitamin is not obviously clinically meaningful when the amount retained still vastly exceeds requirements.
Hydroxocobalamin’s superior plasma retention
The clearest and best-established retention advantage belongs not to methylcobalamin but to hydroxocobalamin. Because hydroxocobalamin binds tightly to plasma cobalamin-binding proteins, an intramuscular dose is retained in plasma longer and excreted in urine less than an equivalent dose of cyanocobalamin.[7] By contrast, methylcobalamin that is not bound to specific cobalamin-binding proteins is likely to be freely filtered by the kidney, so free methylcobalamin and cyanocobalamin may actually have similar plasma turnover. The upshot is that when injection frequency matters, hydroxocobalamin — not methylcobalamin — is the form with the robust pharmacokinetic case, which is exactly why European practice favors it for maintenance dosing.
Which form is the most stable, and does that matter for you?
Stability is where cyanocobalamin has an unambiguous, uncontested advantage, and it explains much of why it dominates manufacturing.
All cobalamins are sensitive to light to some degree, but the active coenzyme forms are the most fragile. Methylcobalamin and adenosylcobalamin are both very light-sensitive and are readily converted to hydroxocobalamin by exposure to white light; methylcobalamin will even convert spontaneously to hydroxocobalamin at room temperature in aqueous or methanol solution when protected from light.[6] Cyanocobalamin is far more robust, and hydroxocobalamin is the most stable of all — both are the forms used in commercial preparations for exactly that reason.[6]
Even cyanocobalamin degrades under sunlight: reported losses of cyanocobalamin after two hours of sun exposure range from roughly 15–21% at higher concentrations up to 56–82% at more dilute concentrations, underscoring that dilute B12 in clear solution is vulnerable and should be protected from light.[6] The practical implications are real: a methylcobalamin product is more likely to have partially degraded to hydroxocobalamin by the time it reaches you, especially if handled or stored carelessly, whereas cyanocobalamin better survives the supply chain. For anyone reconstituting a lyophilized research vial, light protection and prompt use matter more for the labile active forms than for cyanocobalamin. Our general peptide reconstitution guide covers the handling and storage practices that keep light-sensitive compounds intact after mixing.
Injection versus oral: does route matter more than form?
A recurring theme is that the variables people fixate on (which cobalamin) are frequently less important than the variables they overlook (route, dose, and whether absorption physiology is intact). The oral-versus-injection question is a good illustration, because it has been tested in randomized trials.
What the trial evidence says
A Cochrane systematic review identified randomized controlled trials comparing oral with intramuscular B12 in deficient patients. Across the trials, high-dose oral B12 (commonly 1,000 µg/day) produced serum B12 levels with no clinically relevant difference from intramuscular injection, and one trial using 2,000 µg/day even showed higher levels favoring the oral route.[12] A large pragmatic non-inferiority trial in primary care (Project OB12) similarly supported oral replacement as a reasonable strategy for many patients.[13] The reviewers noted the trials were relatively small and short and that patient-important clinical outcomes (not just blood levels) deserve better study — an appropriate note of caution — but the direction of evidence is that high-dose oral therapy can substitute for injections in many, though not all, situations.
When route genuinely matters
Route becomes decisive in specific circumstances: severe neurological involvement (where rapid, guaranteed repletion is prudent), profound malabsorption, poor adherence to daily oral dosing, or clinical instability. In those settings injectable B12 offers assured delivery independent of daily oral compliance. Notably, most injectable B12 in the United States is cyanocobalamin, while European practice leans toward hydroxocobalamin for its longer retention — a difference in form driven by pharmacokinetics and local approval history rather than by any demonstrated superiority of one active coenzyme over another.
Formulation, concentration, and handling of injectable B12
The injectable-versus-oral distinction also intersects with the form question in a practical way that is easy to overlook. FDA-approved cyanocobalamin injection is standardized at 1,000 µg/mL, and typical loading-and-maintenance schedules are built around that concentration — for example, frequent doses during initial correction, tapering to periodic maintenance, with lifelong dosing where malabsorption is permanent.[16] Because cyanocobalamin is chemically robust, these commercial solutions tolerate the manufacturing, sterilization, and storage that a light-sensitive active form handles less gracefully. A methylcobalamin injectable, by contrast, demands more careful light protection throughout its life cycle, and any partial photodegradation converts it toward hydroxocobalamin — which, ironically, is itself a perfectly usable form, but not the one printed on the label.
For readers working with lyophilized research vials rather than pre-mixed pharmaceutical ampoules, the handling implications compound. A powdered cobalamin is relatively stable, but once reconstituted into aqueous solution it becomes vulnerable to both light and, for the active forms, spontaneous conversion at room temperature. Reconstituted B12 should be shielded from light, kept refrigerated, and used within a sensible window rather than stored indefinitely in a clear container on a bench. If you are reviewing a specific injectable regimen, our B12 10 mg vial dosage protocol lays out the reconstitution math and handling considerations for the vial format commonly used in research settings, the reconstitution guide covers the light-protection and diluent choices that keep labile compounds intact, and the dosage calculator helps translate a target microgram dose into an injection volume.
The cyanocobalamin–cyanide question: how worried should anyone be?
No discussion of B12 forms is complete without addressing the elephant in the room: cyanocobalamin contains a cyanide group, and “cyanide” is an alarming word. Putting it in context requires distinguishing the alarming label from the actual quantities and physiology.
The quantities involved
Each molecule of cyanocobalamin carries one cyanide ion, which is released when the molecule is de-cyanated inside the cell. But the amount of cyanide involved is minuscule. A typical supplement or therapeutic dose delivers cobalamin in the microgram-to-milligram range, and the cyanide moiety is a small fraction of the molecule’s mass. Because cyanide’s atomic weight is roughly 2% of cyanocobalamin’s, even a large 1,000 µg dose liberates on the order of 20 µg of cyanide — and a routine daily supplement of a few micrograms liberates a fraction of a microgram. To put that in perspective, cyanogenic foods eaten in ordinary quantities, and especially tobacco smoke, deliver cyanide loads that dwarf what any reasonable B12 dose contributes.
The resulting free cyanide is therefore trivial compared with dietary sources encountered routinely — cyanogenic compounds in foods like almonds, lima beans, flaxseed, stone-fruit kernels, and cassava, and, far more significantly, the sustained cyanide load carried by smokers. The body detoxifies low levels of cyanide efficiently, principally via the mitochondrial enzyme rhodanese, which combines cyanide with a sulfur donor to form thiocyanate for urinary excretion. This detoxification pathway has ample spare capacity for the amounts in question. For a person with normal detoxification capacity and normal renal function, the cyanide released from cyanocobalamin is simply not a meaningful toxicological concern, which is why regulatory bodies have never treated it as a safety limit on the vitamin.[14]
The legitimate exceptions
There are, however, real populations in which cyanocobalamin is reasonably avoided, and these are worth stating precisely rather than generalizing into blanket fear.
- Leber hereditary optic neuropathy (LHON) and tobacco-alcohol amblyopia. In these mitochondrial optic neuropathies, impaired cyanide detoxification and heightened optic nerve vulnerability mean that even the small cyanide load from cyanocobalamin is best avoided; hydroxocobalamin is the preferred form because it binds rather than releases cyanide.[15]
- Advanced renal impairment. Because thiocyanate (the detoxification product) is cleared renally, people with significantly impaired kidney function have a theoretical case for preferring hydroxocobalamin, especially at high or repeated doses.
- Heavy smokers. Smokers already carry a chronic cyanide burden, so avoiding an additional (small) source is a defensible, if minor, consideration.
These exceptions are the kernel of truth inside the “cyanide is bad” messaging. They are genuine but narrow. They do not support the broad claim that cyanocobalamin is unsafe for the general population, for whom decades of use and an enormous evidence base show it to be highly effective and well tolerated.
Hydroxocobalamin as a cyanide antidote — the same chemistry, inverted
There is an elegant irony worth appreciating. The very property that makes cyanocobalamin the “cyanide-containing” form — cobalamin’s avidity for cyanide — is what makes hydroxocobalamin a life-saving antidote for cyanide poisoning. Given intravenously at high doses (grams, not micrograms), hydroxocobalamin binds free cyanide stoichiometrically and rapidly to form cyanocobalamin, which is then excreted harmlessly in the urine. This is an FDA-approved use, marketed as Cyanokit, and it is the modern first-line antidote for cyanide toxicity, including smoke-inhalation victims.[16] So cobalamin both “carries” cyanide (as cyanocobalamin) and “captures” it (as hydroxocobalamin) — a reminder that the same chemistry reads as a hazard or a therapy entirely depending on quantity and context.
What about MTHFR, methylation, and the case for methylated B12?
A major driver of the methylcobalamin market is the popular narrative around MTHFR gene polymorphisms. The reasoning goes: people with reduced-activity MTHFR variants (such as C677T) have impaired conversion of folate to its active 5-methyltetrahydrofolate form, struggle with methylation, and therefore need “pre-methylated” nutrients — methylfolate and methylcobalamin — to bypass the bottleneck.
Where the logic is sound and where it overreaches
The MTHFR-and-methylfolate part of this story has a stronger basis than the MTHFR-and-methylcobalamin part. MTHFR is the enzyme that makes methylfolate, so providing methylfolate directly does plausibly bypass a reduced-activity MTHFR enzyme.[17] But MTHFR does not act on cobalamin. Methylcobalamin is generated inside the cell by methionine synthase during its catalytic cycle, using the methyl group from methylfolate — it is not produced by MTHFR, and a defective MTHFR does not impair the cell’s ability to methylate cobalamin. So the claim that MTHFR carriers specifically need methylcobalamin (as opposed to any adequate B12 source) does not follow from the enzymology, because, as established above, whichever cobalamin form you supply is stripped and rebuilt intracellularly anyway.
Trials that combine methylfolate, vitamin B6, and methylcobalamin do lower homocysteine and can benefit selected populations, but these effects are largely attributable to correcting folate/B12 status and to the methylfolate component, and they do not isolate a unique benefit of methylcobalamin over an equivalent dose of another well-absorbed B12 form.[18] In short: the case for methylfolate in MTHFR carriers is reasonable; the case for methylcobalamin specifically, over adequate cyanocobalamin or hydroxocobalamin, is not well supported by the underlying biochemistry.
How is B12 deficiency actually diagnosed and treated?
Because “which form” only matters once you have decided to supplement, it helps to anchor the discussion in how deficiency is recognized and corrected — a domain where the evidence base is mature and where form choice is genuinely secondary.
Recognizing deficiency
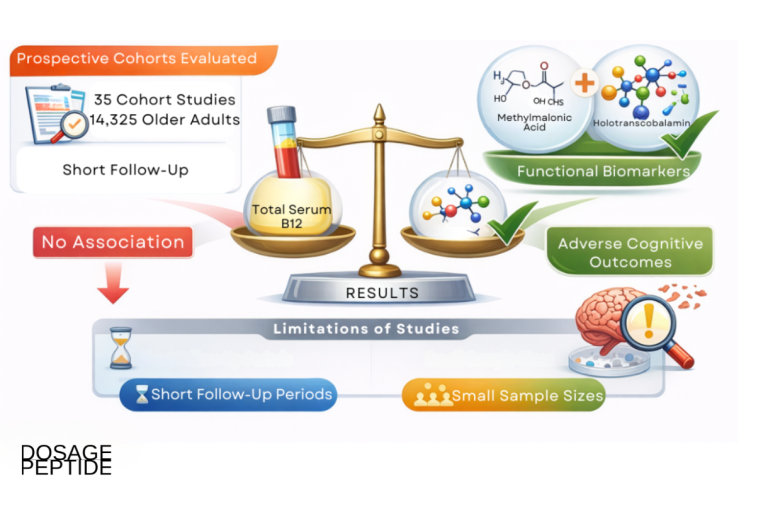
Classic B12 deficiency produces megaloblastic (macrocytic) anemia and a spectrum of neurological and neuropsychiatric features — peripheral neuropathy, subacute combined degeneration of the spinal cord, cognitive changes, and mood disturbance — some of which can become irreversible if correction is delayed.[2] Serum B12 alone is an imperfect test; a substantial fraction of people with subclinical deficiency have “normal” serum B12. This is why elevated methylmalonic acid (the specific marker, reflecting the stalled mutase reaction) and elevated homocysteine (also elevated in folate deficiency) are used as more sensitive confirmatory markers, and why holotranscobalamin (the metabolically active fraction) is increasingly used.[19]
Treatment and the secondary role of form
Correction is achieved with either high-dose oral B12 or intramuscular injections, titrated to the cause and severity, with lifelong therapy in irreversible malabsorption such as pernicious anemia. Standard injectable regimens (for example, frequent loading doses followed by maintenance every few weeks to months) are well established for both cyanocobalamin and hydroxocobalamin.[16] Across these regimens, the form is a secondary decision: cyanocobalamin has the largest evidence base and corrects deficiency reliably; hydroxocobalamin offers longer retention and fewer injections; and both restore B12-dependent enzyme function once inside the cell. If you want to understand where B12 sits alongside other commonly studied research compounds and their reconstitution requirements, the related NAD+ vial dosage protocol and the site glossary provide additional reference context.
Does B12 form matter for cognition, mood, and energy?
Because vitamin B12 is frequently marketed and researched in the cognitive-and-mood arena, it is worth examining whether the choice of form has any special relevance there — and separating the well-established biology from the aspirational claims.
The mechanistic link between B12 and the nervous system is real and well characterized. B12-dependent methionine synthase feeds the methylation cycle that produces S-adenosylmethionine, which the brain uses to methylate neurotransmitters, phospholipids, and myelin components; and the mutase reaction keeps methylmalonic acid from accumulating (elevated MMA and abnormal fatty-acid handling are implicated in the demyelinating injury of B12 deficiency). This is why frank deficiency causes measurable neuropsychiatric harm — peripheral neuropathy, subacute combined degeneration, cognitive slowing, and depressed mood — and why correcting a genuine deficiency can meaningfully improve neurological symptoms.[2]
What the evidence does not establish is that one form outperforms another for these outcomes, or that supplementing B12 in already-replete people improves cognition or mood. The neurological benefit tracks with correcting deficiency, not with the ligand on the molecule. Because any adequately delivered cobalamin restores methionine-synthase and mutase activity through the same intracellular route, the “methylcobalamin is better for the brain” claim has no mechanistic foundation once you account for interconversion. The honest position is that B12 status matters a great deal for neurological and psychiatric health, the form matters little, and B12 is not a demonstrated cognitive enhancer in people who are not deficient. This is precisely the kind of claim where marketing has run ahead of the trial evidence, and where an evidence-first reader should keep the two separate.
How should you actually choose a B12 form?
If the research does not crown a universal winner, how does a scientifically literate reader make a rational choice? The answer is to match the form to the specific situation rather than to a slogan. The table below distills the evidence-based logic.
| Situation or priority | Most rational form | Why |
|---|---|---|
| General oral supplementation / correcting typical deficiency | Cyanocobalamin | Most stable, cheapest, largest evidence base, reliably effective |
| Minimizing injection frequency (maintenance) | Hydroxocobalamin | Longest plasma retention, lower urinary loss |
| Leber hereditary optic neuropathy / tobacco-alcohol amblyopia | Hydroxocobalamin | Avoids the cyanide moiety; binds rather than releases cyanide |
| Significant renal impairment or heavy smoking | Hydroxocobalamin | Reduces an already-elevated cyanide/thiocyanate burden |
| Acute cyanide poisoning (a separate indication entirely) | Hydroxocobalamin (high-dose IV) | FDA-approved antidote; scavenges cyanide as cyanocobalamin |
| Preference for an “active/natural” form | Methylcobalamin / adenosylcobalamin | Legitimate coenzymes; reasonable but not demonstrably superior; less stable |
Notice what this table does not say: it does not identify any common situation in which methylcobalamin is clearly the correct choice over the alternatives on efficacy grounds. The active forms are defensible options for those who prefer them, but the affirmative case for paying more for them, or for believing they work fundamentally better inside the body, is not supported by the interconversion biochemistry or the comparative trial record.
So which B12 form does the research actually favor?
Pulling the threads together, an honest, evidence-weighted verdict looks like this.
For most people and most purposes, the form matters far less than the marketing implies. Because every cobalamin is stripped to a common intermediate and rebuilt into the needed coenzyme intracellularly, the theoretical case for “active-form superiority” largely dissolves. The mechanistic review by Obeid and colleagues concludes plainly that there is insufficient evidence that the benefits of methylcobalamin or adenosylcobalamin override those of cyanocobalamin or hydroxocobalamin in terms of bioavailability, biochemical effects, or clinical efficacy.[7]
Cyanocobalamin has the strongest overall evidence base and practical profile. It is the most stable, the most studied, the least expensive, and it reliably corrects deficiency. Its cyanide content is a non-issue for the general population and a genuine but narrow concern for specific groups.
Hydroxocobalamin has the best-supported pharmacokinetic advantage — longer plasma retention and fewer injections — and is the rational choice where cyanide avoidance matters (LHON, heavy smokers, significant renal impairment) or where reducing injection frequency is valuable. It is also, separately, the definitive high-dose cyanide antidote.
Methylcobalamin and adenosylcobalamin are legitimate active coenzymes but weak supplement differentiators. The retention data modestly favoring methylcobalamin are real but of uncertain clinical importance given B12’s abundant stores and non-toxicity, and their light-sensitivity is a manufacturing and handling liability. The “you need the active/methylated form” argument, including the MTHFR framing, is largely unsupported once you account for intracellular interconversion.
The most defensible summary is not “methylcobalamin is superior” nor “cyanocobalamin is superior,” but rather: adequate delivery of any well-made cobalamin, at a sufficient dose and by an appropriate route, corrects deficiency and restores B12-dependent metabolism. Choose the form to fit the situation — stability and cost favor cyanocobalamin, retention and cyanide-avoidance favor hydroxocobalamin, and the active forms are reasonable but rarely necessary options. Research does not favor a single winner; it favors matching the form to the clinical and practical context, and it does not support paying a premium for “active” forms on the assumption that they work fundamentally better inside the cell.
Frequently Asked Questions
Is methylcobalamin really better absorbed than cyanocobalamin?
The evidence does not support a clear absorption advantage. Some studies actually report slightly higher uptake for cyanocobalamin at the point of ingestion, and reviews conclude that between-form differences at typical supplement doses are small and probably clinically insignificant. Host factors — age, genetics, gut and stomach health, and whether intrinsic factor is present — influence how much B12 you absorb far more than the choice of upper axial ligand does.
Does cyanocobalamin’s cyanide content make it dangerous?
Not for the general population. Each dose releases only a trace of cyanide, far less than routine dietary and tobacco-smoke exposure, and the body detoxifies it efficiently via rhodanese. The legitimate exceptions are narrow: Leber hereditary optic neuropathy, tobacco-alcohol amblyopia, significant kidney impairment, and heavy smokers, for whom hydroxocobalamin is preferred. Decades of use establish cyanocobalamin as effective and well tolerated for most people.
Why do the active coenzyme forms exist if the body converts everything anyway?
The two active forms — methylcobalamin and adenosylcobalamin — are what the enzymes methionine synthase and methylmalonyl-CoA mutase actually use inside cells. But the cell builds them on demand from a common stripped-down intermediate, regardless of which form you ingest. So the coenzymes are essential biochemically, yet supplying them pre-formed as a supplement offers no reliable advantage, because they are dismantled and rebuilt intracellularly like any other form.
Is hydroxocobalamin better than cyanocobalamin for injections?
It has one well-established advantage: hydroxocobalamin binds plasma proteins more tightly, so it is retained longer and excreted less than cyanocobalamin after injection, meaning fewer injections for maintenance. This is why European practice often favors it. It is also preferred when avoiding cyanide matters. Both forms correct deficiency effectively; the choice reflects retention, cyanide considerations, and regional approval history rather than superiority of one coenzyme role.
Do people with MTHFR variants need methylcobalamin specifically?
The enzymology does not support this. MTHFR produces methylfolate, so methylfolate can plausibly bypass a reduced-activity MTHFR enzyme — but MTHFR does not act on cobalamin at all. Methylcobalamin is generated inside cells by methionine synthase, not MTHFR, and any B12 form is interconverted intracellularly. The reasonable MTHFR intervention is methylfolate; the specific need for methylcobalamin over other adequate B12 forms is not well supported.
Can high-dose oral B12 replace injections?
In many cases, yes. Randomized trials and a Cochrane review found that high-dose oral B12 (commonly 1,000–2,000 µg/day) achieves serum levels comparable to intramuscular injection, even in pernicious anemia, because about 1% is absorbed by intrinsic-factor-independent passive diffusion. Injections remain preferable for severe neurological deficiency, profound malabsorption, poor adherence, or clinical instability. This is a clinical decision that depends on the individual and should involve a qualified provider.
Which form is most stable for storage and reconstitution?
Cyanocobalamin is the most stable of the commonly supplemented forms, and hydroxocobalamin is the most stable overall, which is why both dominate pharmaceutical manufacturing. The active forms, methylcobalamin and adenosylcobalamin, are notably light-sensitive and convert to hydroxocobalamin on light exposure. All cobalamins should be protected from light, but this matters most for the labile active forms — keep reconstituted solutions shielded from light and use them promptly.
Is there any risk from taking too much B12?
Vitamin B12 has no established tolerable upper intake level because it has very low toxicity potential; the body stores what it needs and excretes the excess in urine. Large-dose supplementation in long-term trials has not produced serious adverse events attributable to B12 itself. That said, “no toxicity ceiling” is not a reason to megadose indiscriminately, and unexplained high serum B12 can occasionally be a marker of other conditions worth investigating with a clinician.
References
- Vitamin B12 (Cobalamin). StatPearls, NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK559132/
- Langan RC, Goodbred AJ. Vitamin B12 Deficiency: Recognition and Management. Am Fam Physician. 2017. https://www.aafp.org/pubs/afp/issues/2017/0915/p384.html
- Goulding CW, Postigo D, Matthews RG. Cobalamin-Dependent Methionine Synthase Is a Modular Protein with Distinct Regions for Binding Homocysteine, Methyltetrahydrofolate, Cobalamin, and Adenosylmethionine. Biochemistry. 1997;36(26):8082-8091. https://pubs.acs.org/doi/10.1021/bi9705164
- Biological Activity of Pseudovitamin B12 on Cobalamin-Dependent Methylmalonyl-CoA Mutase and Methionine Synthase. PMC7396987. https://pmc.ncbi.nlm.nih.gov/articles/PMC7396987/
- Vitamin B12 — Health Professional Fact Sheet. NIH Office of Dietary Supplements. https://ods.od.nih.gov/factsheets/VitaminB12-HealthProfessional/
- Juzeniene A, et al. Photodegradation of cobalamins in aqueous solutions and in human blood. J Photochem Photobiol B. 2013. https://www.sciencedirect.com/science/article/abs/pii/S1011134413000444
- Obeid R, Fedosov SN, Nexø E. Cobalamin coenzyme forms are not likely to be superior to cyano- and hydroxyl-cobalamin in prevention or treatment of cobalamin deficiency. Mol Nutr Food Res. 2015. PMC4692085. https://pmc.ncbi.nlm.nih.gov/articles/PMC4692085/
- Obeid R, et al. Cobalamin coenzyme forms are not likely to be superior… (PubMed record). PMID 25820384. https://pubmed.ncbi.nlm.nih.gov/25820384/
- Oral Vitamin B12 Replacement for the Treatment of Pernicious Anemia. PMC4993789. https://pmc.ncbi.nlm.nih.gov/articles/PMC4993789/
- Comparative Bioavailability and Utilization of Particular Forms of B12 Supplements. PMC5312744. https://pmc.ncbi.nlm.nih.gov/articles/PMC5312744/
- Okuda K, Yashima K, Kitazaki T, Takara I. Intestinal absorption and concurrent chemical changes of methylcobalamin. J Lab Clin Med. 1973;81(4):557-567. https://www.translationalres.com/article/0022-2143(73)90235-7/abstract
- Wang H, et al. Oral vitamin B12 versus intramuscular vitamin B12 for vitamin B12 deficiency (Cochrane). PMC5112015. https://pmc.ncbi.nlm.nih.gov/articles/PMC5112015/
- Bolaman Z / Sánchez, et al. Oral versus intramuscular vitamin B12 (Project OB12). PMC3403849. https://pmc.ncbi.nlm.nih.gov/articles/PMC3403849/
- Cyanocobalamin. StatPearls, NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK555964/
- Optic neuropathy and chronic cyanide intoxication: a review. PMC1291478. https://pmc.ncbi.nlm.nih.gov/articles/PMC1291478/
- Hydroxocobalamin. StatPearls, NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK557632/
- MTHFR Gene Polymorphisms: A Single Gene with Wide-Ranging Clinical Implications — A Review. PMC12027316. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12027316/
- Effect of Methylfolate, Pyridoxal-5′-Phosphate, and Methylcobalamin on Homocysteine and LDL in MTHFR/MTR/MTRR Polymorphisms: A Randomized Controlled Trial. PMC11173557. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11173557/
- Diagnostic Accuracy of Holotranscobalamin, Vitamin B12, Methylmalonic Acid, and Homocysteine in Detecting B12 Deficiency. PMC7017578. https://pmc.ncbi.nlm.nih.gov/articles/PMC7017578/