The question in this article’s title reads like a claim waiting to be confirmed, so it is worth answering the honest version of it up front: current research does not establish that the “Glow” peptide blend enhances collagen synthesis in humans. What the literature actually contains is a body of preclinical and cosmetic-formulation data on the blend’s individual components — principally the copper tripeptide GHK-Cu, with supporting roles for BPC-157 and TB-500 (a thymosin beta-4 fragment) — alongside an almost total absence of controlled human trials on the finished three-peptide combination itself. Those are very different things, and conflating them is the most common error in the popular writing on this compound.
Glow is a fixed-ratio research blend, not a licensed drug or an approved cosmetic active. It is sold by research-chemical vendors as a lyophilized powder “for laboratory research use only,” and it has never been evaluated as a unit in a registered clinical trial. So the useful framing is not “does Glow work?” but rather “what does the mechanistic and preclinical evidence for its ingredients suggest, how strong is that evidence, and what enormous gaps remain between a fibroblast dish and a measurable change in a living person’s dermal collagen?” This article walks through the origin of the blend, the collagen biology that “enhancement” would actually require, the proposed mechanism of each component, the honest evidence level, comparisons to related blends, the research models used, safety signals, handling considerations in a research setting, the human-evidence gap, and the regulatory status.
Throughout, the goal is calibration rather than promotion. Some of the underlying signals — especially for GHK-Cu — are genuinely interesting and reproducible in cell culture. But an interesting in-vitro signal is a hypothesis about human physiology, not a demonstration of it. Readers evaluating this compound in a research context, and certainly anyone tempted to read cosmetic promise into it, should keep that distinction firmly in view. For the practical parameters vendors report, see the dosagepeptide.com GLOW (70 mg vial) research protocol page; this article addresses the science behind the premise.
What the Glow Blend Is and Where It Came From
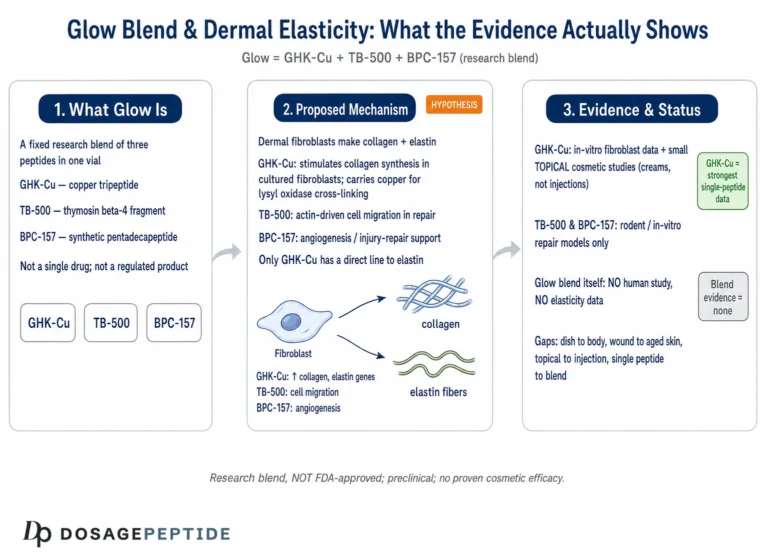
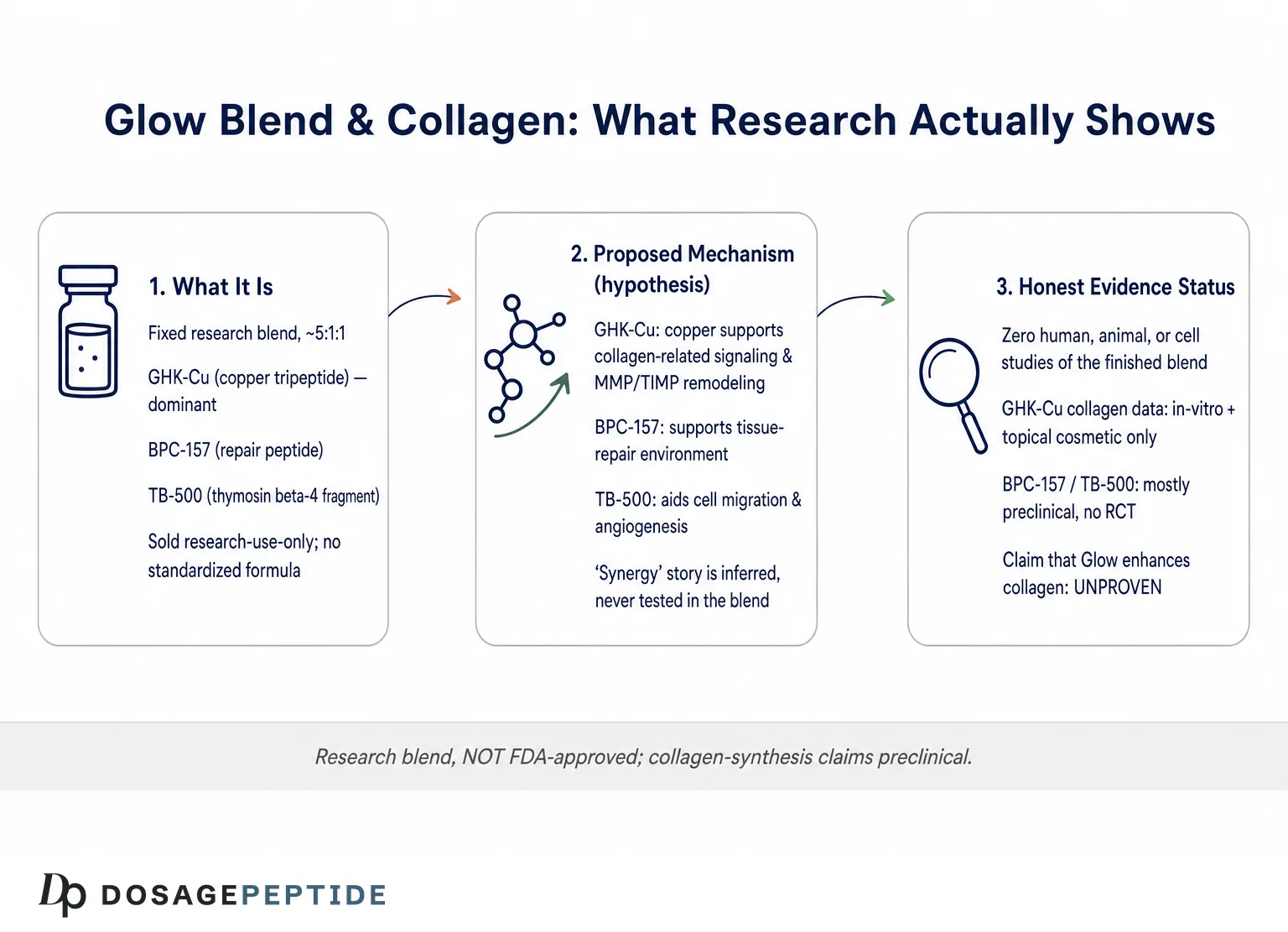
“Glow” is a marketing name applied by research-chemical suppliers to a fixed combination of three peptides delivered together in a single vial. The composition is broadly consistent across vendors: GHK-Cu (the dominant component by mass), BPC-157, and TB-500, typically freeze-dried without fillers. Reported total vial loads vary — some list a 70 mg vial and others a 50 mg vial — and the internal ratio is most often described as roughly 5:1:1 (GHK-Cu : BPC-157 : TB-500), for example 50 mg GHK-Cu with 10 mg each of BPC-157 and TB-500.1 That ratio matters, because it means the blend is overwhelmingly a copper-peptide product with two smaller “repair peptide” additions rather than an equal-parts cocktail.
None of the three peptides is a novel invention of the blend’s marketers; each has its own decades-long research lineage. GHK — glycyl-L-histidyl-L-lysine — was isolated from human plasma by Loren Pickart in 1973 and later characterized as a copper(II)-binding tripeptide, giving the complexed form written GHK-Cu.2 BPC-157 is a synthetic pentadecapeptide (15 amino acids) corresponding to a partial sequence within a protein found in human gastric juice; it is studied chiefly as a cytoprotective and soft-tissue “healing” peptide.7 TB-500 is a synthetic fragment of thymosin beta-4 (Tβ4), a 43-amino-acid actin-sequestering peptide expressed in nearly all mammalian cell types and studied for wound repair and angiogenesis.8 The blend, in other words, gathers three separately researched molecules under a single cosmetic-sounding label.
The rationale offered for combining them is a “regenerative synergy” story: GHK-Cu is cast as the extracellular-matrix and collagen driver, BPC-157 as the tissue-repair and angiogenic supporter, and TB-500 as the cell-migration and vascularization agent, so that together they supposedly cover more of the wound-healing cascade than any one alone. This is a plausible-sounding hypothesis and nothing more. There is no published study demonstrating that this specific 5:1:1 combination produces additive or synergistic collagen effects, that the components do not interfere with one another (copper chelation chemistry is not trivially compatible with arbitrary co-formulation), or that the combined pharmacokinetics resemble the sum of the parts. The synergy narrative is an inference drawn from separate single-agent literatures, not a finding about Glow.
| Component | Class / size | Origin | Primary research theme | Typical share of blend |
|---|---|---|---|---|
| GHK-Cu | Copper-bound tripeptide (Gly-His-Lys) | Isolated from human plasma, 1973 | ECM/collagen signaling, wound repair | ~5 parts (dominant) |
| BPC-157 | Pentadecapeptide (15 aa) | Partial sequence from gastric juice protein | Cytoprotection, tendon/soft-tissue repair | ~1 part |
| TB-500 | Fragment of thymosin beta-4 (43 aa peptide) | Synthetic Tβ4-derived | Cell migration, angiogenesis | ~1 part |
It is also worth naming what Glow is not. It is not an FDA-approved medicine, not a cleared cosmetic active with a monograph, and not a compound with a standardized, quality-controlled formulation. Purity, exact ratio, copper-loading state, and endotoxin content vary between suppliers and are attested (when at all) by vendor certificates of analysis rather than by an independent regulatory body. For readers wanting background on the lead ingredient specifically, dosagepeptide.com maintains an explainer, What is GHK-Cu? Mechanism, Benefits, Risks & How to Use, which situates the copper peptide within the broader research context that the Glow blend borrows from.
The Collagen Synthesis Pathway: What “Enhancement” Would Actually Require
To judge whether any compound “enhances collagen synthesis pathways,” it helps to be precise about what those pathways are, because the phrase is often used loosely. Collagen is the dominant structural protein of skin, tendon, and connective tissue, and its production is a multi-step, tightly regulated process. Dermal fibroblasts transcribe the collagen genes (chiefly COL1A1, COL1A2 for type I and COL3A1 for type III), translate procollagen chains, hydroxylate proline and lysine residues in reactions that require vitamin C and, critically, are influenced by copper-dependent enzymes, assemble triple helices, secrete procollagen, cleave the propeptides, and cross-link the fibrils extracellularly via lysyl oxidase — itself a copper-dependent enzyme.2 Net collagen content in tissue reflects the balance between this synthetic arm and the degradative arm, which is governed largely by matrix metalloproteinases (MMPs) and their tissue inhibitors (TIMPs).
“Enhancement,” therefore, could in principle mean several distinct things, and they are not interchangeable. It could mean increasing transcription of collagen genes; increasing the amount of collagen protein deposited; shifting the MMP/TIMP balance toward net accumulation; improving the quality or cross-linking of the collagen laid down; or producing a clinically measurable change in skin thickness, elasticity, or wrinkle parameters. A compound might move an early upstream marker (say, COL1A1 mRNA in a dish) without ever producing the downstream endpoint that people actually care about (visibly firmer skin). The measurement chosen dictates how impressive the result sounds, which is exactly why evidence-cautious reading demands attention to which node of the pathway a given study actually touched.
Copper is a recurring thread here, and it explains much of the mechanistic interest in GHK-Cu specifically. Lysyl oxidase, the enzyme that cross-links collagen and elastin into mature, load-bearing fibers, requires copper as a cofactor. Prolyl and lysyl hydroxylases, and superoxide-handling systems relevant to the fibroblast microenvironment, also intersect with copper and iron chemistry. The hypothesis that a copper-delivering peptide could support collagen maturation is thus biologically coherent — copper is a genuine rate-relevant micronutrient in this pathway. Coherence, however, is not sufficiency: delivering copper is not the same as being copper-limited, and most well-nourished tissue is not starved for copper. A mechanism that could matter only matters if the system is actually operating below the ceiling the mechanism would raise.
There is a further subtlety that undermines simple “more collagen is better” thinking. Healthy dermal remodeling is not maximal synthesis; it is balanced turnover. Runaway collagen deposition is the pathology of fibrosis and scarring, not the signature of youthful skin. The most-cited GHK-Cu mechanism is precisely that it appears to modulate both arms — upregulating MMP-1 and MMP-2 (which clear damaged collagen) while also upregulating TIMP-1 (which protects new collagen) — i.e., remodeling rather than one-directional accumulation.4 This is a more sophisticated and more plausible story than “peptide makes more collagen,” but it also means that translating a dish-level “increase in collagen” into a promise about human skin is genuinely fraught. The pathway is a balance, and balances resist crude push.
Finally, the delivery problem sits underneath all of this. Most of the mechanistic collagen data on GHK-Cu comes from fibroblasts bathed directly in defined peptide concentrations, or from topical cosmetic formulations engineered with penetration enhancers or nanocarriers. The Glow blend, by contrast, is marketed for reconstitution and injection in a research context. Whether a subcutaneously injected copper-peptide blend reaches dermal fibroblasts at the picomolar-to-nanomolar concentrations that are optimal in vitro, in intact skin, over a sustained enough period to shift matrix biology, is simply not established. The pathway can be real and the compound can bind copper and the delivery can still fail to reproduce the in-vitro condition. Keep that chain of “ifs” in mind for every mechanism described below.
Proposed Molecular Mechanisms of Each Component
Because Glow is a combination, its proposed mechanism is really three overlapping stories. The GHK-Cu component carries most of the collagen-specific rationale. In cultured fibroblasts, GHK-Cu has been reported to stimulate collagen synthesis, with the classic 1988 work of Maquart and colleagues describing stimulation beginning between 10-12 and 10-11 M and peaking near 10-9 M, independent of any change in cell number — that is, a signaling effect rather than simply more cells making baseline collagen.3 Later work extended this to elastin, glycosaminoglycans, proteoglycans (including dermatan sulfate and decorin), and the MMP/TIMP remodeling balance already described.4 The proposed upstream driver is copper delivery to copper-dependent processes plus modulation of transcriptional programs.
The most dramatic mechanistic claim for GHK-Cu comes from gene-expression profiling. Pickart and Margolina, drawing on Broad Institute Connectivity Map data, reported that GHK-Cu shifts the expression of a large fraction of assayed human genes — on the order of roughly a third at a ≥50% change threshold in that dataset — and framed the peptide as a broad “resetting” signal toward a more regenerative, less inflammatory transcriptional state, including modulation of NF-κB inflammatory signaling and TGF-β-linked repair pathways.2 This is striking, but it must be read with care: a Connectivity Map signature is a high-throughput screen of a cell line exposed to a compound, not evidence of a coordinated beneficial effect in human skin. Very broad gene-expression changes are as consistent with nonspecific stress responses as with targeted regeneration. The breadth of the signal is a reason for interest and equally a reason for caution.
BPC-157’s proposed mechanism is only loosely collagen-specific. In tendon-fibroblast studies, BPC-157 promoted ex-vivo outgrowth, cell survival under stress, and migration, with the effect linked to activation of the FAK-paxillin pathway and to induction of F-actin formation; a separate study reported upregulation of the growth-hormone receptor in tendon fibroblasts, potentially sensitizing them to endogenous growth hormone.5,6 Additional preclinical work invokes nitric-oxide signaling, VEGFR2 activation, and angiogenesis. These mechanisms plausibly support a repair-permissive environment — more fibroblast migration and better vascularization — but note that “supports the healing milieu” is not the same as “directly drives dermal collagen synthesis,” and essentially all of it is animal or cell data.
TB-500 / thymosin beta-4 acts principally as a G-actin sequestering peptide, regulating the actin cytoskeleton that underlies cell motility. In the foundational dermal study, thymosin beta-4 applied to full-thickness rat wounds increased reepithelialization by around 42% at day 4 and up to 61% at day 7 versus saline, with histology showing enhanced angiogenesis, increased collagen deposition, and faster wound contraction.8 The proposed collagen relevance is thus indirect: by accelerating angiogenesis and cell migration into a wound, Tβ4 creates conditions under which fibroblasts deposit matrix more readily. Again, the primary readout is wound closure in animals, with collagen deposition as a secondary histological observation, not a mechanistic demonstration that Tβ4 upregulates collagen transcription in healthy human dermis.
Put together, the combined mechanistic hypothesis for Glow is that GHK-Cu supplies the copper-dependent, matrix-modulating collagen signal while BPC-157 and TB-500 improve the vascular and cellular environment in which that signal plays out. It is internally consistent as a story. What it is not is a validated pharmacology: no published work maps the actual molecular behavior of the three peptides together, at Glow’s ratio, in any tissue. Every arrow in the combined diagram is imported from a single-agent study conducted under different conditions.
What the Evidence Actually Shows — and at What Level
Here is the crux, stated plainly: the evidence for the Glow blend as a collagen-enhancing intervention in humans is essentially absent, and the evidence for its components is heavily weighted toward preclinical and cosmetic-formulation data rather than rigorous clinical efficacy trials. Sorting the literature by strength is the single most useful thing a reader can do.
The strongest component evidence belongs to GHK-Cu, and even that is mixed in quality. On the robust end, the in-vitro collagen-stimulation finding is old, reproducible, and mechanistically characterized.3 There are also cosmetic clinical data: a study of GHK-Cu delivered in nanocarriers to facial skin reported reductions in wrinkle volume and depth versus a control serum,4 and a separate, often-cited 12-week trial of a GHK-Cu facial cream in women with photoaged skin reported measurable improvements in skin density, thickness, and appearance versus vehicle,13 with an independent pilot study using histologic and ultrastructural analysis likewise finding that a copper-binding peptide cream enhanced dermal collagen synthesis in a subset of treated subjects.14 These are real human data — but they test topical cosmetic formulations of GHK-Cu alone, with cosmetic endpoints (wrinkle imaging, skin density), typically in modest sample sizes and often industry-associated. They are meaningfully relevant to “does topical copper peptide improve skin appearance,” and only tangentially relevant to “does an injected three-peptide blend enhance collagen synthesis.”
For BPC-157 the clinical evidence base is strikingly thin. A 2024–2025 systematic review screening more than 500 records found only a tiny number of clinical studies among overwhelmingly preclinical work — on the order of a single clinical study among roughly three dozen included, the rest being animal experiments — and reviewers have repeatedly noted that there is no published, peer-reviewed, randomized, placebo-controlled human efficacy trial with accessible results for any indication.9,10 A small intravenous safety pilot and scattered case reports are essentially the extent of the human data. For TB-500 specifically (as distinct from pharmaceutical thymosin beta-4 eye drops), controlled human efficacy data are likewise absent; the human clinical program for Tβ4 has centered on ophthalmic formulations for dry eye and neurotrophic keratitis, not on injected TB-500 for skin collagen.11
| Claim | Best available evidence | Evidence level |
|---|---|---|
| GHK-Cu stimulates collagen synthesis in fibroblasts | Maquart 1988 and later in-vitro work | Moderate (reproducible in vitro) |
| Topical GHK-Cu improves skin appearance | Small cosmetic clinical studies, alone, topical | Low–moderate (small, cosmetic endpoints) |
| BPC-157 aids soft-tissue repair | Animal/cell studies; ~1 clinical study in reviews | Low (preclinical, no RCT) |
| TB-500 promotes wound healing/collagen deposition | Rodent wound models; Tβ4 eye-drop trials | Low (animal + non-skin clinical) |
| The Glow blend enhances human collagen synthesis | No trials of the blend exist | None (unproven premise) |
The most important row in that table is the last one. There are zero controlled trials — indeed zero published studies of any kind — testing the finished Glow blend for collagen synthesis or any other endpoint in humans. Everything asserted about Glow is extrapolated from single-agent literatures, mostly preclinical, conducted with different formulations, routes, and doses. So the accurate summary is: a suggestive-to-moderate in-vitro and topical-cosmetic signal for one of the three ingredients, thin preclinical signals for the other two, and nothing at all on the combination. That is not a foundation for claiming the blend “enhances collagen synthesis pathways” in any clinically meaningful sense.
How Glow Compares to Its Individual Parts and to Related Blends
A fair comparison starts by noting that the “value proposition” of any blend is convenience and a synergy hypothesis, not superior evidence. On the evidence axis, the single agents actually beat the blend, because at least the single agents have been studied individually, whereas the combination has not been studied at all. If a researcher’s question is specifically about collagen biology, isolated GHK-Cu is the better-characterized tool: its concentration-response in fibroblasts is defined, its topical cosmetic data exist, and its mechanism is not confounded by two co-administered peptides. Adding BPC-157 and TB-500 introduces variables without adding collagen-specific evidence.
Against the standalone repair pairing of BPC-157 with TB-500 — a widely discussed “recovery” duo — Glow simply layers GHK-Cu on top. The BPC-157/TB-500 combination is itself researched only preclinically, and the rationale for stacking those two is soft-tissue and injury repair rather than dermal collagen or “skin glow.” Readers interested in that pairing’s logic can consult dosagepeptide.com’s explainer, BPC-157 + TB-500 Blend Explained: Why Researchers Stack Them, and the corresponding BPC-157 + TB-500 (10 mg blend) research protocol. The point of comparison is that Glow’s distinctive ingredient, relative to that duo, is the copper peptide — which is where essentially all of its collagen-specific (and cosmetic) rationale comes from.
The closest sibling to Glow is KLOW, which adds a fourth peptide — KPV, a tripeptide (lysine-proline-valine) derived from the C-terminal region of alpha-MSH with anti-inflammatory research interest — to the same GHK-Cu/BPC-157/TB-500 base, often as an 80 mg vial (50/10/10/10).1 KLOW’s marketing rationale is that KPV further dampens inflammatory signaling, but it shares Glow’s fundamental limitation: no published trials of the four-peptide combination exist either. The dosagepeptide.com KLOW dosage protocol guide lays out the reported parameters for that variant. Choosing between Glow and KLOW is a choice between two unproven combinations differing by one anti-inflammatory tripeptide, not a choice between graded strengths of evidence.
| Product | Peptides | Stated rationale | Evidence on the combination itself |
|---|---|---|---|
| GHK-Cu (single) | GHK-Cu | ECM/collagen signaling | Best-characterized single agent (in vitro + topical cosmetic) |
| BPC-157 + TB-500 | 2 peptides | Soft-tissue recovery | Preclinical only; no RCT |
| Glow | GHK-Cu + BPC-157 + TB-500 | Regenerative “synergy” | None (no studies of the blend) |
| KLOW | Glow + KPV | Adds anti-inflammatory KPV | None (no studies of the blend) |
The honest comparative conclusion is counterintuitive to the marketing: the more peptides a product stacks, the less direct evidence exists for the exact thing being sold, because combinations are studied far less than their parts. Convenience and a synergy story trade against evidentiary clarity. For a researcher, that argues for isolating variables — studying GHK-Cu alone if collagen is the question — rather than reaching for the multi-peptide blend, whose collagen claim rests entirely on borrowed, single-agent, mostly preclinical data.
Research Models and Methodology Behind the Claims
Understanding how the underlying studies were done is essential to weighting them, because the model determines what a result can and cannot mean. The GHK-Cu collagen literature rests heavily on cell-culture models: primary human dermal fibroblasts (or, in some studies, irradiated or aged fibroblasts) exposed to defined peptide concentrations, with readouts such as collagen and elastin protein, hydroxyproline content, MMP/TIMP gene and protein expression, and proliferation.3,4 The strength of this design is mechanistic control — you can isolate a concentration-response curve. Its limitation is that a monolayer of fibroblasts bathed in peptide is a radically simplified stand-in for intact, vascularized, immunologically active human skin. Effects that appear at 10-9 M in a dish may never be reproduced by an injected or topical dose in vivo, where absorption, distribution, protein binding, and clearance all intervene.
The cosmetic clinical studies use a different methodology: human volunteers apply a topical GHK-Cu formulation, and outcomes are assessed by instrumental skin imaging (wrinkle volume/depth, skin density by ultrasound, elasticity) over weeks.4,13 These are genuine human data and closer to a real endpoint, but they carry their own caveats: small sample sizes, cosmetic (appearance) rather than histological (biopsy-confirmed collagen) endpoints in many cases, frequent industry sponsorship, formulation-specific results (a particular cream or nanocarrier, not the peptide in isolation), and short durations. A wrinkle-imaging improvement is a legitimate cosmetic outcome but a weak proxy for “enhanced collagen synthesis pathways” at the tissue level.
The BPC-157 and TB-500 evidence leans even more heavily on animal models: rodent tendon, muscle, gut, and skin-wound experiments, plus ex-vivo tissue explants and cell-migration assays.5,8,9 Rodent wound-healing models are informative for hypothesis generation but notoriously over-optimistic as predictors of human efficacy; rodent skin heals differently from human skin (more contraction, looser attachment), and the injury contexts studied (acute surgical or chemical wounds) differ from the chronic, low-grade “aging” context that skin-collagen marketing invokes. The methodological distance between “Tβ4 accelerated closure of a full-thickness rat wound” and “an injected blend increases collagen in healthy adult human dermis” is very large.
Two systematic methodological red flags recur across this field. First is publication and author concentration: much of the BPC-157 literature originates from a small number of research groups, and independent replication is limited — a pattern reviewers explicitly flag when cautioning against over-reading the animal data.9,10 Second is the gap between surrogate and clinical endpoints. Many “positive” findings are early surrogate markers — mRNA levels, phosphorylation states, histology scores — rather than the outcomes a person would notice. Surrogate markers frequently fail to translate into clinical benefit, and the history of dermatology and regenerative medicine is littered with in-vitro “collagen boosters” that did nothing measurable in controlled human trials.
The methodological bottom line for Glow specifically is that the blend has never been the subject of any of these study types. There is no cell-culture study of the three peptides combined, no animal study of the blend, and no human study. So even the modest, model-limited evidence that exists for the parts cannot be assumed to carry over, because combination effects (synergy, antagonism, altered stability, competition for uptake or copper) are precisely the things that single-agent studies cannot capture. The methodology supporting Glow’s headline claim is, in the strictest sense, not the study of Glow at all.
Safety and Tolerability Signals
Safety discussion here must be framed carefully, because “no serious problems reported” in a lightly studied compound is very different from “demonstrated to be safe.” For GHK-Cu, the topical cosmetic safety record is reassuring within its narrow domain: the copper in topical formulations is chelated to the peptide and used locally in small amounts, systemic copper toxicity from cosmetic use has not been reported in the literature, and the most common adverse events described are transient local irritation, redness, or tingling, with true allergic contact reactions considered relatively uncommon.4 That record, however, is about topical products, generally studied over weeks to a few months, with cosmetic-level exposure. It does not automatically extend to repeated subcutaneous injection of a higher-mass copper-peptide blend.
Copper load is the specific consideration that distinguishes an injected copper-peptide blend from a topical cream. Because Glow is GHK-Cu-dominant, repeated injection delivers copper directly past the skin barrier, and total copper burden becomes a relevant variable — particularly hypothetically in anyone with disordered copper metabolism (Wilson’s disease, Menkes disease) where copper handling is pathological.2 There is no controlled human data defining a safe cumulative injected copper dose for this use, no toxicokinetic study of the blend, and no long-term safety follow-up. The absence of reported harm reflects an absence of study, not a positive demonstration of safety at the exposures the blend implies.
For BPC-157, the human safety database is genuinely minimal: a small intravenous pilot reported tolerability without serious adverse events in a very small number of subjects, and scattered case reports have not flagged consistent serious harms — but this is nowhere near the scale needed to characterize a safety profile.9,10 Regulators’ concern has centered partly on impurities in unregulated synthesized material rather than on a proven intrinsic toxicity, which is a different and important point: much of the practical risk of research-grade peptides is manufacturing quality (endotoxin, residual solvents, incorrect sequence, incorrect copper loading), not the idealized molecule. For TB-500, injected human safety data are essentially absent; the reassuring ophthalmic Tβ4 safety data apply to eye drops, not systemic injection.11
Then there is the combination itself. No one has studied the safety of these three peptides administered together at Glow’s ratio. Drug–drug interaction, additive immunogenicity, and formulation-stability concerns (copper chemistry interacting with the other peptides, or with the reconstitution solvent over time) are unstudied. Injectable products also carry the generic, non-trivial risks of any self-prepared injection: infection, injection-site reactions, and contamination if sterile technique or product sterility is imperfect. None of these are exotic; they are the ordinary hazards that make unsupervised use of unapproved injectables inadvisable. The candid safety summary is: limited and mostly topical/preclinical reassurance for the ingredients, no safety data on the blend, real theoretical concerns around cumulative copper and product quality, and no regulatory safety oversight.
Handling and Reconstitution in a Research Context
In a laboratory research setting — the only setting for which this material is nominally sold — handling and reconstitution matter both for validity and for a specific chemical reason unique to copper peptides. Glow is supplied lyophilized (freeze-dried). Lyophilized peptide is comparatively stable: copper-peptide powder is generally reported stable for many months refrigerated and longer frozen, whereas once reconstituted the working solution is far more perishable.12 Vendors and reconstitution guides typically describe dissolving the powder in bacteriostatic water (which contains ~0.9% benzyl alcohol as a preservative), giving a refrigerated working stability on the order of roughly 3–4 weeks, versus only 24–48 hours if plain sterile water without preservative is used.12
The copper-specific wrinkle is pH and container chemistry. GHK-Cu is reported to be most stable in a mildly acidic window (approximately pH 5.5–6.5); above roughly pH 7, copper dissociation from the peptide accelerates, which matters because the copper is integral to the proposed mechanism. Standard soda-lime glass vials can leach sodium ions over time and raise solution pH, nudging the system toward copper release; and unlike the dry powder, reconstituted solution should not be frozen, because ice-crystal formation can physically damage the peptide.12 For a researcher, these facts translate into concrete controls: use preserved diluent for multi-use vials, refrigerate (do not freeze) the working solution, protect from prolonged light and heat, minimize the interval between reconstitution and use, and treat any color change or precipitate as a reason to discard.
Reported research parameters, which appear on vendor and protocol pages, illustrate the arithmetic without endorsing any use. For a 70 mg Glow vial reconstituted with, say, 3 mL of bacteriostatic water, the total peptide concentration is roughly 23.3 mg/mL; applying the stated 5:1:1 ratio to a reported per-administration figure of about 2,330 mcg implies on the order of 1.67 mg GHK-Cu with about 0.33 mg each of BPC-157 and TB-500 per unit.1 These numbers are experimental parameters reported by suppliers, not validated doses, not clinically justified, and not human-use recommendations. They exist so that a researcher can compute concentrations for laboratory work, and they should be read as measurement bookkeeping rather than as evidence that any particular quantity produces any particular effect.
| Handling factor | Reported practice / value | Why it matters |
|---|---|---|
| Diluent | Bacteriostatic water (benzyl alcohol preservative) | Extends working stability to ~3–4 weeks vs 24–48 h |
| Reconstituted storage | Refrigerate 2–8°C; do not freeze | Freezing damages peptide; heat/light degrade it |
| pH sensitivity | Most stable ~pH 5.5–6.5 | Alkaline drift accelerates copper dissociation |
| Lyophilized storage | Months refrigerated; longer frozen | Dry powder far more stable than solution |
Even meticulous handling, it should be stressed, only preserves the integrity of the material; it does nothing to establish that the material does what is claimed. A perfectly reconstituted, correctly stored, copper-intact solution of an unproven blend is still an unproven blend. Handling rigor is necessary for valid research and irrelevant to the efficacy question. For the fuller set of reported single-agent parameters, dosagepeptide.com’s GHK-Cu (100 mg vial) research protocol page catalogs the copper-peptide figures that the Glow blend inherits.
Limitations and the Human-Evidence Gap
It is worth consolidating the limitations, because they are the heart of an honest answer to the title question. The first and largest is that no study of the Glow blend exists. Every positive statement about the compound is an extrapolation from separate single-agent literatures, and extrapolation across combination, route, dose, formulation, and species is exactly where regenerative-medicine claims most often fail. The synergy hypothesis that justifies the blend has never been tested; it is possible the peptides interfere with one another, compete for uptake, or destabilize the copper complex, and nothing in the literature rules these out.
The second limitation is the model-to-human gap for the ingredients that have been studied. GHK-Cu’s most quotable collagen data are in-vitro; its human data are topical cosmetic studies with appearance endpoints, small samples, and frequent industry ties. BPC-157 and TB-500 rest almost entirely on animal and cell work, with essentially no randomized, placebo-controlled human efficacy trials for the relevant claims.9,10,11 A dish or a rat wound is a hypothesis generator, not a demonstration of human benefit, and the specific human context implied by “collagen synthesis” marketing — chronic dermal aging in healthy adults — is barely represented even in the single-agent literature.
The third limitation is the endpoint problem. Much of the favorable evidence sits at the surrogate level: gene expression, protein levels in culture, phosphorylation of signaling intermediates, histology in animals. Surrogate improvements routinely fail to produce the clinical outcomes people care about, and “enhances collagen synthesis pathways” is a mechanistic-surrogate framing that can be technically defensible for GHK-Cu in a dish while being clinically meaningless for an injected blend in a person. The distance between moving a marker and improving a life is where most of the honesty in this topic lives.
The fourth limitation is quality and consistency of the actual product. Research-grade peptide blends are not standardized: purity, exact ratio, copper-loading state, endotoxin content, and even correct sequence vary between suppliers and are attested (when at all) by self-reported certificates. This means that even if the idealized molecules behaved as hoped, the physical material in a given vial might not match the studied entity — a problem regulators have specifically flagged for peptides in this category.10 Batch-to-batch variability alone can swamp any subtle biological effect.
The candid synthesis is therefore this: the premise embedded in the title — that current research supports Glow as a collagen enhancer — is not supported. What research supports is a narrower and more tentative set of statements: that GHK-Cu can stimulate collagen-related activity in cultured fibroblasts and that topical GHK-Cu formulations can improve some cosmetic skin measures; that BPC-157 and TB-500 show repair-associated effects in animals; and that none of this has been demonstrated for the blend, by injection, in humans, for collagen. The gap between those narrower statements and the title’s implication is the entire point. Treat the compound as an open research question, not a validated intervention.
Regulatory Status
Regulatory status reinforces the caution. None of the three peptides in Glow is an FDA-approved drug for any dermatologic or collagen indication, and the blend as a product has no approval, no monograph, and no recognized standardized formulation anywhere. Glow is sold under “research use only” labeling, which is a marketing and legal category, not a signal of quality or of demonstrated safety and efficacy. Research-use-only material is explicitly not intended for human administration, and that labeling exists precisely because the compound has not cleared the evidentiary bar that human-use products must.
BPC-157’s regulatory history is instructive about the volatility of this space. In 2023, FDA placed BPC-157 into “Category 2” of the substances nominated for use in compounding under Section 503A — the category for bulk drug substances that raise significant safety concerns — effectively signaling that it should not be compounded for human use.10 Reporting in 2026 indicates the nomination was subsequently withdrawn and BPC-157 removed from Category 2, but crucially it was not moved to Category 1 (permitted) either; it remains without FDA approval and without a recognized USP/NF monograph, leaving it in a gray zone that is neither explicitly authorized nor, at that moment, explicitly prohibited.10 The lesson is that regulatory posture here can shift, and “not currently on a prohibition list” is not equivalent to “approved” or “shown safe.”
Thymosin beta-4 is the one component with a genuine clinical-development pathway, but importantly for a distinct, non-cosmetic use and a distinct formulation. A pharmaceutical Tβ4 ophthalmic solution (RGN-259) has been advanced through controlled trials for dry eye disease and neurotrophic keratitis, including placebo-controlled work and later-stage programs.11 That legitimate ophthalmic development says nothing about the safety or efficacy of injected TB-500 in a skin-collagen blend; if anything, it highlights the contrast between a rigorously studied eye-drop indication and the unstudied injectable use implied by Glow. GHK-Cu, for its part, is used lawfully as a cosmetic ingredient in topical products in many jurisdictions, but “permitted in a face cream” is not “approved as an injectable collagen therapy.”
The overall regulatory picture, then, is unambiguous even though it contains moving parts: no approved status for the blend or its components as a collagen treatment, an explicit research-only label that forecloses human-use claims, a recent history of active regulatory scrutiny for at least one ingredient, and no quality oversight of the finished product. For readers, the regulatory status is not a bureaucratic footnote but a direct expression of the evidence gap described throughout this article. The compound sits outside the approval system because it has not generated the evidence that the approval system requires.
It is worth being explicit about how this differs from an approved dermatologic or aesthetic therapy, because the contrast clarifies what “unproven” means in practice. An approved injectable would have a defined manufacturing standard with lot-release testing, a characterized pharmacokinetic and toxicology package, dose-finding studies, adequately powered randomized controlled efficacy trials against a comparator, a formal risk–benefit assessment by a regulator, and post-marketing surveillance for rare harms. The Glow blend has none of these. Its “dosing” figures are vendor-reported experimental parameters rather than clinically justified regimens; its safety rests on inference from topical and preclinical data; and its efficacy for collagen is an untested hypothesis borrowed from single-agent studies. Every one of those missing elements is a place where an apparently promising compound has, historically, turned out to be ineffective or unsafe once actually tested. The regulatory vacuum around Glow is therefore not a technicality that a determined enthusiast can reason past; it is the visible marker of exactly the questions that have never been answered. Reading the compound as an open research question, rather than as an established or even probable collagen therapy, is the position the current evidence actually licenses.
Frequently Asked Questions
Does current research prove that the Glow blend enhances collagen synthesis in people?
No. There are no published studies of the Glow blend itself in humans (or in animals or cell culture), so nothing about the finished combination has been demonstrated. The collagen rationale is extrapolated from separate studies of GHK-Cu, most of which are in-vitro or topical cosmetic work, plus mostly animal data on BPC-157 and TB-500. That is a hypothesis, not proof, and the honest answer to the title question is that current research does not support the claim as stated.2,3,9
Isn’t the GHK-Cu collagen data fairly strong?
The in-vitro collagen-stimulation data for GHK-Cu are genuinely reproducible, and there are small topical cosmetic trials suggesting improved skin appearance.3,4,13 But “reproducible in fibroblast culture” and “helps a face cream’s wrinkle score” are not the same as “an injected blend enhances collagen in human dermis.” The strongest GHK-Cu evidence is for isolated, mostly topical use — not for the Glow blend by injection.
Why combine three peptides if only one is the collagen agent?
The marketing rationale is “synergy”: GHK-Cu for matrix signaling, BPC-157 for tissue repair, TB-500 for angiogenesis and cell migration. It is a plausible story, but no study has tested whether the three actually cooperate, interfere, or destabilize each other at Glow’s ratio. Combining agents generally reduces, rather than increases, the directness of the evidence for the specific product being sold.1,8
How does Glow differ from KLOW?
KLOW is essentially Glow plus a fourth peptide, KPV (a lysine-proline-valine tripeptide derived from alpha-MSH with anti-inflammatory research interest), often as an 80 mg vial.1 Like Glow, the four-peptide KLOW combination has no published trials as a unit. Choosing between them is choosing between two unproven blends, not between different evidence strengths. The dosagepeptide.com KLOW protocol guide covers the reported parameters.
Is the copper in the blend a safety concern?
For topical cosmetic use, systemic copper toxicity has not been reported and the copper is chelated locally.4 But Glow is GHK-Cu-dominant and marketed for injection, which delivers copper past the skin barrier; cumulative copper load becomes a real (if under-studied) consideration, especially hypothetically in anyone with disordered copper metabolism. There is no controlled human safety data defining a safe injected copper dose for this use.2
What is the regulatory status of the Glow blend?
None of the components is FDA-approved as a collagen treatment, and the blend has no approval, monograph, or standardized formulation. It is sold “for research use only,” which forecloses human-use claims. BPC-157 was placed in FDA’s compounding Category 2 in 2023 and later removed without being approved, and thymosin beta-4’s only real clinical program is a pharmaceutical eye drop — not an injectable skin blend.10,11
Can I use topical GHK-Cu instead if I care about skin appearance?
This article is educational and not advice to use any product. That said, the human evidence that exists is specifically for topical GHK-Cu cosmetic formulations, not for the injected blend, so the topical single agent is the better-studied entity for skin-appearance questions.4,13,14 Any decision about cosmetic products should be made with a qualified clinician and based on the specific formulation’s own data.
Why do so many articles online sound more positive than this one?
Much online writing conflates in-vitro or animal findings on the ingredients with proven human benefit of the blend, cites vendor material, or reports surrogate markers (gene expression, culture collagen) as if they were clinical outcomes. Evidence-cautious reading separates “a marker moved in a dish” from “a person got a measurable benefit,” and on that standard the blend’s collagen claim is unproven.2,9,10
References
- Composition and reported research parameters for GLOW and KLOW peptide blends (GHK-Cu / BPC-157 / TB-500 [+ KPV]), vendor and protocol listings. Simple Peptide, BioLongevity Labs, and dosagepeptide.com blend pages. https://simplepeptide.com/product/ghk-cu-bpc-157-tb-500-glow-blend/ ; https://www.dosagepeptide.com/peptide-blends/glow-70-mg-vial-dosage-protocol/
- Pickart L, Margolina A. Regenerative and Protective Actions of the GHK-Cu Peptide in the Light of the New Gene Data. Int J Mol Sci. 2018;19(7):1987. PMC6073405. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6073405/
- Maquart FX, Pickart L, Laurent M, et al. Stimulation of collagen synthesis in fibroblast cultures by the tripeptide-copper complex glycyl-L-histidyl-L-lysine-Cu2+. FEBS Lett. 1988;238(2):343–346. https://www.sciencedirect.com/science/article/pii/001457938880509X
- Effects of GHK-Cu on MMP and TIMP Expression, Collagen and Elastin Production, and Facial Wrinkle Parameters (human dermal fibroblast and topical volunteer study). J Aging Sci. https://www.walshmedicalmedia.com/open-access/effects-of-ghkcu-on-mmp-and-timp-expression-collagen-and-elastin-production-and-facial-wrinkle-parameters-2329-8847-1000166.pdf
- Chang CH, Tsai WC, Lin MS, Hsu YH, Pang JHS. The promoting effect of pentadecapeptide BPC 157 on tendon healing involves tendon outgrowth, cell survival, and cell migration. J Appl Physiol. 2011;110(3):774–780. https://journals.physiology.org/doi/full/10.1152/japplphysiol.00945.2010
- Chang CH, Tsai WC, et al. Pentadecapeptide BPC 157 enhances the growth hormone receptor expression in tendon fibroblasts. Molecules. 2014. https://www.researchgate.net/publication/268790268
- Multifunctionality and Possible Medical Application of the BPC 157 Peptide — Literature and Patent Review. PMC11859134. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11859134/
- Malinda KM, Sidhu GS, Mani H, et al. Thymosin beta4 accelerates wound healing. J Invest Dermatol. 1999;113(3):364–368. https://pubmed.ncbi.nlm.nih.gov/10469335/
- Vasireddi N, Hahamyan H, Salata MJ, et al. Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review. HSS J. 2025. doi:10.1177/15563316251355551. https://journals.sagepub.com/doi/abs/10.1177/15563316251355551
- U.S. Food and Drug Administration. Certain Bulk Drug Substances for Use in Compounding That May Present Significant Safety Risks (503A Category 2; BPC-157 nomination history). https://www.fda.gov/drugs/human-drug-compounding/certain-bulk-drug-substances-use-compounding-may-present-significant-safety-risks
- Sosne G, et al. RGN-259 (thymosin β4) ophthalmic solution clinical trials for dry eye disease and neurotrophic keratitis (Phase II/III). Nature Sci Rep 2018;8:10322; PMC9820614. https://www.nature.com/articles/s41598-018-28861-5 ; https://pmc.ncbi.nlm.nih.gov/articles/PMC9820614/
- GHK-Cu stability, reconstitution, and storage practices (bacteriostatic water, pH 5.5–6.5 stability window, refrigerated working solution). Palmetto Peptides / SeekPeptides handling references. https://palmettopeptides.com/blogs/news/05-ghk-cu-storage-handling-stability
- Leyden JJ, Stephens T, Finkey MB, Barkovic S. Skin care benefits of copper peptide containing facial cream. Poster presentation, American Academy of Dermatology 60th Annual Meeting, 2002 (12-week study in women with photoaged skin; instrumental ultrasound/profilometry improvements in skin density, thickness, and wrinkle parameters versus vehicle). Summarized in Pickart L, Margolina A, Int J Mol Sci 2018;19(7):1987. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6073405/
- Abdulghani AA, Sherr A, Shirin S, et al. Effects of topical creams containing vitamin C, a copper-binding peptide cream and melatonin compared with tretinoin on the ultrastructure of normal skin — a pilot clinical, histologic, and ultrastructural study. Dis Manag Clin Outcomes. 1998;1(4):136–141. doi:10.1016/S1088-3371(98)00011-4. https://www.semanticscholar.org/paper/30a364b77183ae029822a4e48059c7e042040aa8
Educational and research-use disclaimer: This article is provided for educational and scientific-literacy purposes only. The Glow peptide blend is an unapproved research compound; it is not an FDA-approved drug, is not a proven cosmetic or medical treatment, and is labeled for laboratory research use only. Nothing here is medical advice or a recommendation to obtain, prepare, or administer any peptide, and no statement should be read as claiming that Glow, or its components, diagnoses, treats, cures, prevents, or enhances any condition or physiological process in humans. Evidence for collagen-related effects is preclinical or, for isolated topical GHK-Cu, limited and cosmetic; the finished blend has not been studied in humans. Consult a qualified, licensed healthcare professional before making any health decision.