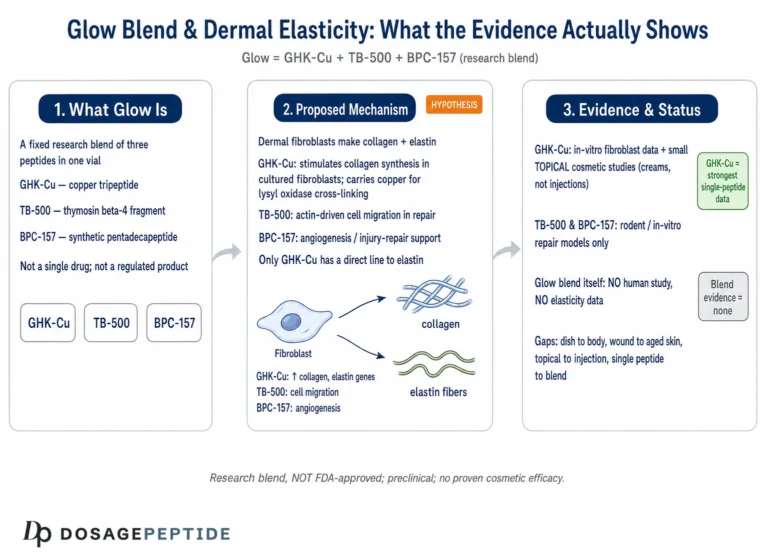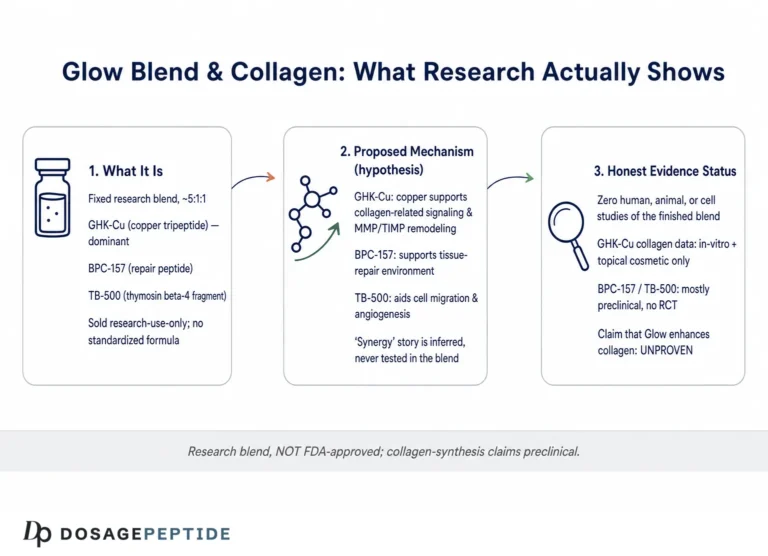
Search the phrase “glow peptide” and you will find it attached to promises that outrun the science: luminous skin in weeks, collagen “switched back on,” years erased from the face. The Glow blend is a real research compound, but the honest story is narrower and more interesting than the marketing. Glow is a three-peptide research mixture that combines GHK-Cu (copper tripeptide-1), BPC-157 (a stable gastric pentadecapeptide fragment), and TB-500 (a synthetic fragment of thymosin beta-4), typically supplied together in a single lyophilized research vial.1 Each of those three molecules has an individual literature trail. Glow, as a fixed blend, does not.
That distinction matters for anyone reading this page. When people ask “why does science support Glow for skin brightening and anti-aging,” they are usually blending together three separate bodies of evidence and treating the sum as if it applied to the finished product. It does not, at least not in the way a clinical claim would require. The strongest human evidence sits with topical GHK-Cu, a copper peptide studied in cosmetic dermatology for more than two decades. The evidence for injected BPC-157 and TB-500 in skin is almost entirely preclinical, drawn from rodent wound-healing models and cell culture. And there is, as of this writing, no published human trial of the Glow blend itself as a brightening or anti-aging intervention. It is a research compound, not an FDA-approved drug.11
This article walks through what the underlying science does and does not establish: the origin and composition of each peptide, the molecular mechanisms that give rise to the “glow” hypothesis, the actual level of evidence for skin outcomes, how Glow compares with related blends such as KLOW and Tri-Heal, the research models used to study these molecules, the safety record, handling in a research setting, the substantial human-evidence gap, and the current regulatory status in the United States. The goal is not to sell a story but to let you calibrate the claims against the primary literature.
What the Glow Blend Is and Where Its Peptides Come From
The Glow blend is best understood as three independently discovered peptides packaged for convenience, not as a single engineered molecule. Understanding where each component originated helps explain why the “skin brightening and anti-aging” framing gets applied to it, and why that framing is only partly earned.
GHK-Cu (copper tripeptide-1) is the oldest and most studied of the three. The tripeptide glycyl-L-histidyl-L-lysine (GHK) was first isolated by Loren Pickart in the 1970s from human plasma, where its concentration declines with age, from roughly 200 ng/mL in young adults to about 80 ng/mL by the sixth decade of life.1 GHK has a high affinity for copper(II) ions, and the resulting GHK-Cu complex is the biologically active species most often studied in skin. Decades of work by Pickart and colleagues established GHK-Cu as a signal peptide that participates in wound repair, extracellular-matrix remodeling, and antioxidant defense, and it became a mainstay ingredient in cosmetic dermatology.1,2 It is the component of Glow with genuine human cosmetic data behind it.
BPC-157 is a synthetic 15-amino-acid peptide. Its sequence corresponds to a partial fragment of a larger protein, “body protection compound,” originally identified in human gastric juice, and it was characterized beginning in the early 1990s by Predrag Sikiric and colleagues at the University of Zagreb.5,6 In animal models it has been described as cytoprotective and pro-angiogenic, promoting new blood-vessel formation and accelerating healing of tendon, muscle, gut, and skin injuries.5,9 Its inclusion in a “glow” blend rests on the idea that improved local perfusion and tissue repair could support skin quality, an idea that is mechanistically plausible but not demonstrated for cosmetic endpoints in humans.
TB-500 is a synthetic peptide corresponding to the actin-binding region of thymosin beta-4 (Tβ4), a naturally occurring 43-amino-acid protein that is the principal G-actin-sequestering molecule in mammalian cells.4 The commonly cited TB-500 sequence (acetylated Ac-LKKTETQ) reproduces the seven-residue actin-binding motif spanning roughly residues 17 to 23 of the parent protein, the segment shown to be essential for its angiogenic activity.4 Full-length thymosin beta-4 has been advanced into human clinical trials for indications such as dry-eye disease and dermal wounds by biotechnology developers, but TB-500 the research fragment is not the same regulated drug product, and it is not FDA-approved.
Put together, the three peptides share a common theme: each is connected, in some model system, to tissue repair, angiogenesis, or extracellular-matrix biology. That shared theme is why they are co-formulated and why the blend gets marketed for skin. But shared themes in mechanism do not equal proven, additive benefit in a finished product. A blend of three repair-associated peptides is a reasonable research hypothesis; it is not, on its own, evidence that the combination brightens or rejuvenates human skin. The Glow 70 mg blend protocol page describes how these three are supplied together in a single research vial, and it is careful to state that the combination itself is not clinically validated.
The Molecular Mechanism Behind the “Glow” Claim

The “glow” hypothesis is a mechanistic argument stitched together from three separate stories. To evaluate it honestly, it helps to look at what each peptide is proposed to do at the cellular level, and then ask whether those mechanisms would actually converge on “brighter, younger-looking skin.”
GHK-Cu is the mechanistic centerpiece. In cell and tissue studies it stimulates fibroblasts and promotes synthesis of collagen, elastin, and the glycosaminoglycans and proteoglycans (including decorin) that give the dermis structure and hydration.1 It appears to modulate the balance between matrix metalloproteinases (MMPs) and their tissue inhibitors (TIMPs), meaning it can influence both the buildup and the controlled remodeling of the extracellular matrix.1 GHK-Cu also carries copper, an essential cofactor for lysyl oxidase (which cross-links collagen and elastin) and for superoxide dismutase (an antioxidant enzyme), and it has independent antioxidant and anti-inflammatory activity in cultured cells.1,2 The most striking, and most frequently overstated, finding is genomic: analyses using the Broad Institute’s Connectivity Map reported that GHK altered expression of a very large fraction of assayed human genes, with one analysis describing effects on thousands of genes and a resetting of expression patterns toward those associated with healthier tissue states.2 That is a real and provocative dataset, but it comes from cultured cell lines exposed to the peptide, not from human skin measured in a trial, and it says nothing directly about “brightening.”
BPC-157’s proposed contribution is vascular and cytoprotective. In preclinical work it upregulates vascular endothelial growth factor receptor 2 (VEGFR2) signaling and engages the nitric-oxide pathway, promoting endothelial cell proliferation, migration, and new vessel formation in injury models.5,9 The logic for skin is that better microcirculation and faster resolution of micro-injury could, in principle, support the environment in which fibroblasts do their work. This is a plausible supporting role, but the evidence is from tendon, gut, and muscle injury models and from angiogenesis assays such as the chick chorioallantoic membrane, not from human facial-skin studies.
TB-500 acts on the actin cytoskeleton. By sequestering monomeric G-actin, thymosin beta-4 regulates the actin dynamics that drive cell migration; its actin-binding motif is required for its pro-angiogenic effect, and in dermal wound-healing assays the parent protein accelerates keratinocyte and endothelial migration, increases collagen deposition, and reduces inflammation.4 Cell migration and angiogenesis are exactly the processes needed to close a wound, which is why Tβ4 has been studied as a wound-healing agent.
Now the honest synthesis. Notice what is missing from all three mechanisms: none of them is primarily a pigment mechanism. “Skin brightening” in dermatology usually refers to reducing hyperpigmentation, evening tone, and lowering melanin deposition. The mechanistic case for Glow is really a case about the dermal matrix, vascularity, and repair, i.e., firmness, thickness, fine-line depth, and healing, with “brightening” appearing indirectly through improved matrix quality, better light reflection from smoother skin, and reduction of mottled pigmentation seen in some GHK-Cu cosmetic studies.3 In other words, the mechanistic story supports a plausible anti-aging / skin-quality hypothesis far more than a direct brightening one, and even the anti-aging mechanism is best documented for topical GHK-Cu, not for an injected three-peptide blend. The mechanisms are real; the leap from mechanism to guaranteed cosmetic outcome is where marketing outpaces evidence.
What the Human Evidence Actually Shows for GHK-Cu
If any part of Glow has earned the phrase “science supports,” it is GHK-Cu, and even here the evidence is cosmetic-grade rather than drug-grade. It is worth being precise about what has and has not been demonstrated, because this is the strongest card the blend holds.
The most cited human data come from small, controlled cosmetic studies of topical GHK-Cu on facial and body skin. In a frequently referenced 12-week facial study, women with photodamaged skin who applied a GHK-Cu-containing cream showed improvements in skin laxity, clarity, and firmness, reductions in fine lines and wrinkle depth, increases in skin density and thickness on ultrasound, and reduced mottled hyperpigmentation compared with baseline and control preparations.3 A separate line of work compared copper-peptide creams against established actives: in a thigh-skin biopsy study, GHK-Cu was reported to increase collagen production in a larger proportion of treated women than vitamin C or retinoic acid comparators.1 There is also older clinical work on copper-peptide formulations improving re-epithelialization in wound settings such as diabetic ulcers and post-surgical (including laser-resurfaced) skin.1
Reviews summarizing this literature, including recent aesthetic-dermatology overviews, conclude that GHK-Cu is one of the most extensively studied cosmetic carrier/signal peptides and has become a common ingredient for anti-aging, anti-wrinkle, and hydration claims.2,13 That is a fair characterization. But several caveats are non-negotiable for an evidence-cautious reading:
| What the GHK-Cu evidence supports | Important limitation |
|---|---|
| Improvements in fine lines, firmness, density on ultrasound | Measured for topical cream/serum, not the injected Glow blend |
| Increased collagen synthesis in biopsy studies | Small samples, often industry-sponsored cosmetic studies |
| Reduced mottled pigmentation in some cohorts | Not a dedicated, powered “brightening” endpoint vs. a standard agent |
| Broad gene-expression modulation | Derived from cell-line data, not human skin outcomes2 |
| Wound re-epithelialization benefit | Different clinical context than cosmetic anti-aging |
The single most important caveat is the delivery route. Nearly all supportive human GHK-Cu data come from topical application at cosmetic concentrations, not from reconstituted, injected peptide, and certainly not from a fixed blend that also contains BPC-157 and TB-500. Route of administration changes pharmacokinetics, local concentration, and safety considerations entirely. A cream applied to the face and a subcutaneously administered research blend are not interchangeable, and evidence for one does not transfer to the other. It is legitimate to say GHK-Cu has real cosmetic support; it is not legitimate to say that support has been demonstrated for the Glow blend as sold or for injected use.
It is also worth stating plainly that most GHK-Cu cosmetic studies are small (dozens of participants), of short duration (typically 12 weeks), and frequently sponsored by ingredient or product manufacturers. That does not make them worthless, controlled cosmetic studies are how the industry evaluates actives, but it does place them well below the bar of a large, independent, randomized clinical trial with pre-registered endpoints. The correct summary is “promising and repeatedly observed for topical use,” not “clinically proven anti-aging drug.”
One more nuance deserves emphasis because it is the crux of the “brightening” question. In the photoaging studies, when investigators noted improvement in pigmentation, they generally reported it as reduced “mottled hyperpigmentation” or a lower overall photoaging score, endpoints that lump uneven tone together with texture, laxity, and fine lines.3 That is not the same as a controlled trial of GHK-Cu against a recognized depigmenting agent such as hydroquinone, azelaic acid, or a retinoid, measured with an instrument like a mexameter for melanin index. So while it is fair to say GHK-Cu formulations have been associated with a more even complexion in some cohorts, it is not accurate to say GHK-Cu is an established brightening agent in the dermatological sense. The mechanism that most plausibly produces any perceived “glow” is indirect: a denser, better-hydrated, smoother dermal surface reflects light more evenly, which reads to the eye as radiance even when melanin content has not meaningfully changed. That is a real and legitimate cosmetic effect, but it is a texture-and-matrix effect wearing a brightening label, and the distinction matters when someone is choosing an intervention specifically to treat pigmentation.
What the Evidence Shows for BPC-157 and TB-500 in Skin
The other two thirds of Glow rest on a much thinner evidentiary footing when the question is specifically about skin appearance in humans. Both BPC-157 and TB-500 have genuinely interesting preclinical repair literatures, but almost none of it addresses cosmetic brightening or facial anti-aging, and almost none of it is in humans.
BPC-157. The bulk of the published evidence is preclinical, drawn overwhelmingly from rodent injury models.5,9,11 In these studies BPC-157 has been reported to accelerate healing of skin wounds and burns, tendon and ligament injuries, muscle tears, and gastrointestinal lesions, and to promote angiogenesis via VEGFR2 and nitric-oxide-dependent mechanisms.5,9 A 2024 literature-and-patent review catalogs this breadth while explicitly noting that clinical translation remains limited.9 On the human side, the most substantive data are older Phase II inflammatory-bowel-disease trials of a related BPC-157 formulation (PL-14736) conducted by a Croatian pharmaceutical company; these are cited as showing tolerability, but the full trial reports are not readily indexed in major databases, which sharply limits independent verification.6,11 Crucially, none of this is cosmetic. There is no controlled human study showing that injected BPC-157 brightens skin or reduces facial wrinkles. Independent reporting has characterized BPC-157 as a peptide with large claims and comparatively scant high-quality human evidence.11
TB-500 / thymosin beta-4. The parent protein, thymosin beta-4, has a legitimate preclinical wound-healing profile: in dermal assays it promotes keratinocyte and endothelial migration, angiogenesis, collagen deposition, and reduced inflammation, and its actin-binding motif is required for angiogenic activity.4 Full-length Tβ4 has been investigated in human trials for dermal and ocular indications by biotech developers, which is the closest thing to human data in this family. However, TB-500 as sold for research is a synthetic fragment, not the identical clinical drug product, and the leap from “Tβ4 accelerates wound closure in animals” to “TB-500 rejuvenates aging facial skin in people” is unsupported. There is no published, controlled human trial of TB-500 for cosmetic anti-aging or brightening.
The table below is a candid summary of where each Glow component actually stands for skin appearance endpoints specifically.
| Component | Best evidence for skin appearance | Evidence level |
|---|---|---|
| GHK-Cu | Topical cosmetic studies: wrinkles, firmness, density, some pigmentation1,3 | Small human cosmetic trials (topical) |
| BPC-157 | Rodent skin/wound healing; angiogenesis assays5,9 | Preclinical / animal + in vitro |
| TB-500 (Tβ4 fragment) | Animal dermal wound-healing; parent protein in some human wound/eye trials4 | Preclinical for the fragment; limited human data for parent protein |
| Glow (the blend) | No published human cosmetic trial of the combination | None specific to the blend |
The takeaway is not that these peptides are inert, the repair biology is real and reproducible in animals, but that the specific claim “Glow brightens and rejuvenates human skin” is an extrapolation across route, species, and endpoint. For readers who want to understand the individual repair peptides in more depth, the BPC-157 + TB-500 blend protocol and the TB-500 and BPC-157 research stack pages describe how those two are studied together in a repair-focused context, which is where their literature is strongest.
How Glow Compares With Related Peptide Blends
Glow does not exist in isolation; it sits within a small family of multi-peptide “repair and rejuvenation” research blends that share overlapping ingredients. Comparing them clarifies what Glow is actually optimized for and where the marketing logic comes from.
The closest relative is KLOW, a four-peptide research blend that adds KPV (a tripeptide fragment of alpha-melanocyte-stimulating hormone with anti-inflammatory activity in models) to the GHK-Cu / BPC-157 / TB-500 base. A representative KLOW formulation is supplied as an 80 mg vial containing GHK-Cu 50 mg, BPC-157 10 mg, KPV 10 mg, and TB-500 10 mg. The conceptual division of labor promoted for KLOW is that GHK-Cu drives matrix remodeling and copper delivery, BPC-157 supports angiogenesis and perfusion, TB-500 supports cell migration and actin regulation, and KPV adds an anti-inflammatory dimension. Glow, by contrast, is the three-peptide version without KPV. The practical implication is that Glow is weighted toward matrix and vascular repair, while KLOW layers on an additional anti-inflammatory rationale. Neither has published human trials as a finished blend. Readers comparing the two can consult the KLOW dosage and reconstitution guide and the KLOW 80 mg vial protocol for how the four-peptide version is handled in a research context.
A second relative is Tri-Heal, typically formulated as TB-500 25 mg + BPC-157 10 mg + KPV 10 mg. Tri-Heal drops GHK-Cu entirely and is oriented toward tissue repair and inflammation rather than skin cosmesis, which underscores an important point: the presence or absence of GHK-Cu is essentially what makes a blend a “skin/anti-aging” blend versus a “repair” blend, because GHK-Cu is the component with the cosmetic-dermatology literature. The Tri-Heal protocol page reflects that repair-first orientation.
| Blend | Typical composition | Primary rationale | GHK-Cu present? |
|---|---|---|---|
| Glow | GHK-Cu + BPC-157 + TB-500 (e.g., 70 mg vial) | Skin quality / matrix + vascular repair | Yes |
| KLOW | GHK-Cu 50 + BPC-157 10 + KPV 10 + TB-500 10 (80 mg) | Skin + repair + anti-inflammatory | Yes |
| Tri-Heal | TB-500 25 + BPC-157 10 + KPV 10 | Tissue repair / inflammation | No |
Two honest observations follow from the comparison. First, the differences between these blends are combinatorial, not the result of head-to-head studies; no controlled research has compared Glow versus KLOW versus a single peptide for a skin endpoint, so any claim that one is “better for glow” is theoretical. Second, adding more peptides to a vial increases the number of unstudied interactions, not the strength of evidence. A four-peptide blend is not four times as validated as a one-peptide product; if anything, each additional component makes the finished mixture harder to study and to characterize. From an evidence standpoint, the standalone topical GHK-Cu literature remains the most rigorous thing in this entire family, and it applies to none of these injected blends directly.
Research Models and Methodology Behind the Claims
Evaluating “why science supports” any of this requires understanding how the underlying studies were done, because the model largely determines how far a finding can be generalized. The Glow-relevant literature spans four broad methodological tiers, and readers should mentally tag every claim with the tier it came from.
Tier 1: In vitro and biochemical studies. Much of the mechanistic story, GHK-Cu stimulating fibroblast collagen synthesis, copper serving as an enzymatic cofactor, thymosin beta-4 sequestering G-actin, BPC-157 modulating VEGFR2, comes from cultured cells and cell-free biochemistry.1,4,5 These experiments are powerful for establishing plausible mechanism and dose-response at the molecular level, but a cultured fibroblast in a dish is not intact, aged, sun-exposed human skin. In vitro potency routinely fails to translate to clinical benefit.
Tier 2: Genomic / systems-biology analyses. The widely cited GHK gene-expression findings used the Connectivity Map, a database of transcriptional signatures from cell lines exposed to compounds. The analyses reported that GHK influenced a large fraction of assayed genes and nudged expression toward “healthier” patterns.2 This is genuinely interesting hypothesis-generating work, but it is a computational/transcriptomic signal in cell lines, not a demonstration of a clinical outcome. When you see “GHK modulates thousands of genes,” read it as “GHK is transcriptionally active in cell culture,” not “GHK reverses aging in your skin.”
Tier 3: Animal models. The BPC-157 and TB-500 repair literatures live largely here, primarily rodent wound, tendon, muscle, and gut injury models, plus angiogenesis assays like the chick chorioallantoic membrane.5,9 Animal models are essential and often quantitatively rigorous (vessel density, tensile strength, histology), but they involve acute injury in young healthy animals, high relative doses, and species differences in skin and metabolism. Wound-healing acceleration in a rat is not evidence of cosmetic rejuvenation in an aging human face.
Tier 4: Human studies. These are the scarcest and most valuable, and they are unevenly distributed across the blend. For GHK-Cu there are small controlled cosmetic studies of topical formulations with instrumented endpoints (ultrasound, profilometry, high-resolution imaging).1,3 For BPC-157 there are older, poorly-indexed IBD trials of a related formulation.6 For thymosin beta-4 there are developer-run trials of the full-length protein in wound and eye indications. For the Glow blend as a product, there are none. A methodologically honest reader weights human data most heavily and notices that the human data do not cover the actual product or the actual cosmetic claim.
Two methodological problems recur across the cosmetic literature specifically and deserve flagging. The first is sponsorship and small samples: many GHK-Cu cosmetic studies enroll a few dozen participants over 12 weeks and are funded by product manufacturers, which introduces both statistical fragility and potential bias.3 The second is endpoint mismatch: “brightening” is rarely a pre-registered, powered primary endpoint measured against an established depigmenting agent; it more often appears as a secondary observation (“reduced mottled pigmentation”) folded into a broader photoaging score. Neither problem invalidates the work, but both mean the appropriate confidence level is “suggestive,” not “established.” When the methodology is this heterogeneous, the phrase “science supports” should always be qualified by “at which tier, in which species, by which route.”
Safety and Tolerability in the Research Record
Because Glow is used as an injectable research compound rather than a topical cosmetic, safety deserves careful, non-promotional treatment. The available safety information is fragmentary and comes mostly from the individual peptides, studied in contexts that do not match how the blend is actually used.
GHK-Cu. In topical cosmetic use, GHK-Cu has a long track record and is generally well tolerated at cosmetic concentrations, with occasional local irritation or contact sensitivity reported. The important, and often ignored, safety variable is copper. GHK-Cu delivers copper, and while copper is an essential trace element, it is also a redox-active metal; systemic or repeated parenteral copper exposure is a different risk profile from a copper-peptide cream, and it has not been characterized for the doses and routes used with injected blends. Reviews emphasize GHK-Cu’s antioxidant behavior in models, but that does not license an assumption of safety for injected, repeated dosing of a copper-containing peptide.1,2
BPC-157. Preclinical studies consistently report low acute toxicity, and the older human IBD trials of a related formulation were reported as tolerable, with no toxicity noted in the trials referenced within these papers.5,6 However, “no toxicity reported in limited studies” is not the same as an established human safety profile. There are no long-term human safety data, no characterization of effects on angiogenesis in unwanted contexts (a theoretical concern for any pro-angiogenic agent, for example regarding occult tumors), and independent reporting has highlighted exactly this gap between confident marketing and thin human safety evidence.11 The FDA’s own review process has repeatedly flagged BPC-157 for insufficient safety characterization (discussed in the regulatory section below).
TB-500 / thymosin beta-4. Full-length thymosin beta-4 has been administered in human trials with a generally acceptable tolerability signal in those specific settings, but TB-500 the research fragment has not undergone the same formal safety evaluation, and its pro-angiogenic and pro-migratory activity carries the same theoretical cautions as any tissue-remodeling agent.4
Several blend-specific safety realities compound the individual uncertainties:
| Safety consideration | Why it matters for Glow |
|---|---|
| No blend-level safety study | Interactions among three peptides at these ratios are uncharacterized |
| Injection route | Introduces infection, injection-site reaction, and sterility risks absent from topical use |
| Copper load | Repeated parenteral copper exposure is not the same as a cosmetic cream |
| Research-grade sourcing | Purity, endotoxin, and actual composition vary; a Certificate of Analysis mitigates but does not equal pharmaceutical GMP |
| Pro-angiogenic activity | Theoretical concern in the presence of undiagnosed neoplasia or proliferative disease |
The responsible summary is that the individual peptides have reassuring but incomplete safety signals in their studied contexts, and the blend as used, injected, combined, at research-grade purity, has no formal safety evaluation at all. Absence of reported harm in small, short studies is not evidence of long-term safety. This is a research compound; it is not a product that has cleared the safety review a drug or an approved cosmetic would require.
Handling and Reconstitution in a Research Context
Glow is supplied as a lyophilized (freeze-dried) powder in a sealed multi-milligram vial, and how it is handled in a laboratory setting affects both the integrity of any experiment and basic sterility. This section is descriptive of documented research practice; it is not a use recommendation and not medical advice.
Reconstitution is the process of dissolving the dry peptide into a liquid, most commonly bacteriostatic water (sterile water containing 0.9% benzyl alcohol, which suppresses microbial growth over a multi-use period). Documented research protocols for a 70 mg Glow vial describe reconstituting with roughly 3 mL of bacteriostatic water, which is chosen to balance a workable concentration against injection volume in animal or in-vitro handling. The reconstitution volume determines concentration: at 70 mg in 3 mL, the solution is about 23.3 mg/mL of total peptide, and a stated research increment of roughly 0.1 mL would correspond to about 2.33 mg (2330 mcg) of combined peptide. The Glow protocol page walks through this arithmetic and the corresponding syringe-unit conversions in detail; the point here is simply that concentration is a function of the water added, and getting it wrong changes every downstream number.
Good handling practice in the research literature and vendor documentation typically emphasizes a few consistent points:
- Gentle reconstitution. The diluent is directed against the vial wall rather than jetted directly onto the powder, and the vial is swirled, not shaken, because vigorous agitation can shear and denature peptides and generate foam.
- Cold storage. Lyophilized vials are generally stored frozen or refrigerated; once reconstituted, solutions are kept refrigerated (typically 2 to 8 degrees Celsius) and protected from light, with a limited in-use window.
- Sterility and single-source diluent. Alcohol-swabbing the stopper, using sterile technique, and drawing from a bacteriostatic-water source reduce contamination risk during repeated access.
- Certificate of Analysis. Reputable research suppliers provide a batch COA reporting purity (commonly by HPLC) and identity (commonly by mass spectrometry). Because research-grade material is not held to pharmaceutical GMP, a current COA is the main available check on what is actually in the vial.
Concentration errors are the most common and consequential handling mistake in this context. Because the same milligram of powder can be dissolved in anywhere from 1 mL to several milliliters of water, two researchers can prepare vials that differ several-fold in strength while both believing they are following “the protocol.” This is precisely why documented protocols specify both the reconstitution volume and the resulting per-unit content, and why a blend, which contains three peptides at fixed but non-obvious ratios, is harder to reason about than a single-peptide vial. There is no way to independently confirm the ratio of the three peptides in a reconstituted solution without analytical equipment, which again places heavy weight on the supplier’s Certificate of Analysis.
A special note for a copper-containing blend: GHK-Cu solutions often carry a characteristic blue tint from the copper(II) complex, and copper peptides can be sensitive to pH and to certain excipients. The visual cue is expected chemistry, not a defect, but it is another reminder that this is a reactive, metal-bearing molecule rather than an inert cosmetic. None of these handling details make the compound clinically validated; they simply describe how researchers preserve material integrity. Reconstitution technique cannot manufacture efficacy or safety that the underlying evidence does not support.
Limitations and the Human-Evidence Gap
This is the section that most directly answers a skeptical reader, and it deserves to be blunt. The gap between what is claimed for Glow and what has been demonstrated is wide, and it is worth naming each part of that gap explicitly.
No trial of the actual product. The single largest limitation is that there is no published, controlled human trial of the Glow blend, at any dose, for brightening or anti-aging. Every supportive citation you will encounter is about one component, usually in a different formulation, route, or species. Building a product claim from three separate literatures and presenting the sum as evidence for the whole is a logical error known as the fallacy of composition. Three ingredients each with some support do not yield a supported blend.
Route mismatch. The best human evidence in this entire space, the GHK-Cu cosmetic studies, is topical.1,3 The blend is used by injection. Topical anti-aging data cannot be transferred to an injectable protocol; the pharmacokinetics, tissue exposure, and safety considerations are fundamentally different.
Endpoint mismatch. “Brightening” is a specific dermatological outcome (reduced hyperpigmentation, more even tone). The mechanistic strengths of these peptides are in matrix repair, angiogenesis, and cell migration. Where pigmentation improvements appear, they are usually secondary observations within broader photoaging scores, not primary endpoints tested against a standard depigmenting agent.3 The word “brightening” in the marketing is doing more work than the data justify.
Species and model limitations. The BPC-157 and TB-500 repair data are dominated by acute-injury rodent models in young, healthy animals.5,9 Cosmetic anti-aging is a chronic, low-grade process in older human skin. These are different biological problems, and acceleration of acute wound closure does not predict slowing of chronic photoaging.
Study quality and independence. Where human cosmetic data exist for GHK-Cu, samples are small, durations short, and sponsorship frequently commercial.3 For BPC-157, the most-cited human trials are old and not readily indexed for independent scrutiny.6,11 None of this reaches the standard of a large, independent, pre-registered randomized controlled trial.
Overstated genomics. The “GHK modulates thousands of genes / 30-plus percent of the genome” figure is real but frequently deployed to imply proven clinical rejuvenation. It is a cell-line transcriptomic signal, hypothesis-generating rather than outcome-demonstrating.2
It is also worth being explicit about publication and reporting biases that inflate the apparent evidence. Positive cosmetic studies are more likely to be published, promoted, and cited than null results, and vendor and blog content tends to recycle the most favorable framing of the same handful of papers, which creates an illusion of a deep literature when the primary-source base is actually shallow and repetitive. When you trace citations back to their origins, a large share of “Glow is clinically supported” claims collapse into the same small set of GHK-Cu cosmetic studies plus a body of rodent BPC-157 and TB-500 work, none of which tested the blend. Recognizing that echo-chamber effect is part of reading this space honestly.
The intellectually honest position is this: Glow’s individual components have a plausible, mechanistically coherent, and in the case of topical GHK-Cu partially human-validated rationale for supporting skin quality. That is meaningfully more than nothing. But it is far less than “science shows Glow brightens and rejuvenates skin.” The correct verb is “investigational,” and the correct posture is curiosity paired with caution. Anyone claiming certainty about the finished blend’s cosmetic efficacy in humans is ahead of the evidence.
Regulatory Status in the United States
Regulatory status is where the “research compound, not a drug” framing becomes concrete, and it is not optional context, it defines what Glow legally is. The short version: Glow is not an FDA-approved product, and none of its three peptides is an FDA-approved drug for cosmetic or any other indication. It is sold and used as a research chemical, and the underlying peptides sit in a contested regulatory space.
None of the components is FDA-approved as a drug. GHK-Cu is used as a cosmetic ingredient (a different regulatory pathway from drug approval, cosmetics are not “approved” for efficacy in the way drugs are), but injected GHK-Cu is not an approved drug. BPC-157 and TB-500 have no FDA approval for any indication.
The compounding controversy. Much of the recent regulatory action concerns whether these peptides may be used by compounding pharmacies under Section 503A of the Federal Food, Drug, and Cosmetic Act. To be compounded from bulk substance, an ingredient generally must appear on the FDA’s 503A Bulks List, or have a USP/NF monograph, or be a component of an approved drug.7,8 In late 2023, FDA reviewers placed a group of popular peptides, including BPC-157 and TB-500, into “Category 2” of the interim bulk-substances policy, meaning the agency had identified significant safety concerns and insufficient data to support compounding.7,8,10 This effectively signaled that these peptides should not be compounded pending further evaluation.
Recent movement. The regulatory picture is still evolving. In 2026, BPC-157 was removed from Category 2 following withdrawal of its nomination, but it was not moved to Category 1 (the list of substances permitted for compounding), leaving it in a gray zone: not prohibited under that specific category label, but also not affirmatively cleared, and still neither FDA-approved nor covered by a recognized USP monograph.10 BPC-157-related bulk substances have been slated for further consideration at a Pharmacy Compounding Advisory Committee meeting.10 The practical upshot for a reader is that the regulatory status is unsettled and actively under review, which is itself a strong signal that the evidence base is not considered adequate for approval.
| Question | Answer for Glow / its peptides |
|---|---|
| FDA-approved drug? | No, for the blend or any component |
| Approved for anti-aging/brightening? | No |
| On the 503A Bulks List (Category 1)? | No |
| USP/NF monograph? | No recognized monograph for these peptides |
| Legally sold as? | Research-use-only chemical, not for human use |
The bottom line: whatever the mechanistic promise, Glow occupies the “research compound” tier of the regulatory ladder, several rungs below an approved cosmetic and far below an approved drug. That status is not a technicality; it reflects the fact that the safety and efficacy evidence required for approval simply does not exist for these peptides in this use. Reputable research suppliers label the material for laboratory research only and not for human consumption, and that labeling is the accurate legal description of what the product is.
Frequently Asked Questions
Is the Glow peptide blend proven to brighten skin?
No. There is no published, controlled human trial of the Glow blend for brightening or anti-aging. The strongest human evidence in this space is for topical GHK-Cu creams improving photoaging metrics, and even there, pigmentation improvement is usually a secondary finding rather than a dedicated, powered brightening endpoint.1,3 The mechanistic case is more about dermal-matrix quality and repair than about direct pigment reduction. “Investigational,” not “proven,” is the accurate word.
What is actually in Glow?
Glow is a three-peptide research blend of GHK-Cu (copper tripeptide-1), BPC-157, and TB-500 (a thymosin beta-4 fragment), commonly supplied together in a single lyophilized vial such as a 70 mg vial.1,4,5 The related KLOW blend adds a fourth peptide, KPV. The Glow protocol page details the composition and how the blend is reconstituted in a research setting.
Is Glow FDA-approved?
No. Neither the Glow blend nor any of its three peptides is an FDA-approved drug, and it is not approved for anti-aging or brightening. GHK-Cu is used as a cosmetic ingredient (a separate pathway), but injected GHK-Cu, BPC-157, and TB-500 are not approved drugs. BPC-157 and TB-500 have been the subject of FDA compounding review and are not on the permitted Category 1 bulk-substances list.7,8,10 Glow is sold as a research-use-only chemical.
How does Glow differ from KLOW?
KLOW is essentially Glow plus KPV, an anti-inflammatory tripeptide fragment of alpha-MSH. A representative KLOW vial is 80 mg (GHK-Cu 50 + BPC-157 10 + KPV 10 + TB-500 10). Glow is the three-peptide version without KPV, weighted toward matrix and vascular repair. Neither has a published human trial as a finished blend. See the KLOW dosage guide for a direct comparison.
Why is GHK-Cu considered the “anti-aging” part?
GHK-Cu has the most human cosmetic data of the three peptides. In small controlled studies of topical formulations, it has been associated with improvements in fine lines, firmness, skin density on ultrasound, and some pigmentation measures, and in cell studies it stimulates collagen, elastin, and glycosaminoglycan synthesis and modulates thousands of genes.1,2,3 That said, those data are topical and cosmetic-grade, not evidence for the injected blend.
Is BPC-157 in Glow safe?
BPC-157 shows low acute toxicity in animal studies and was tolerated in older human IBD trials of a related formulation, but there are no long-term human safety data, and independent reporting has emphasized the gap between strong claims and thin high-quality human evidence.6,9,11 FDA reviewers previously flagged BPC-157 for safety concerns in the compounding context.7,10 “Reassuring but incomplete” is the honest characterization, and it has not been evaluated as part of this blend.
Can I use the GHK-Cu skin studies to justify injecting Glow?
No, and this is the most common reasoning error. The supportive GHK-Cu evidence is from creams and serums applied to the skin surface, at cosmetic concentrations. Injecting a reconstituted three-peptide blend is a completely different route, dose, and safety context, and topical efficacy data do not transfer to it. There is no human study validating the injected blend for any cosmetic endpoint.
What does the research literature say about dosing and handling?
Documented research protocols describe reconstituting a 70 mg Glow vial with about 3 mL of bacteriostatic water and reference research increments on the order of 2330 mcg of total peptide, with cold storage and sterile technique. These are descriptions of laboratory practice, not medical recommendations. The Glow protocol page and the repair-focused TB-500 and BPC-157 stack page cover reconstitution arithmetic in more depth.
References
- Pickart L, Vasquez-Soltero JM, Margolina A. GHK Peptide as a Natural Modulator of Multiple Cellular Pathways in Skin Regeneration. BioMed Research International. 2015;2015:648108. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC4508379/
- Pickart L, Margolina A. Regenerative and Protective Actions of the GHK-Cu Peptide in the Light of the New Gene Data. International Journal of Molecular Sciences. 2018;19(7):1987. PMID: 29986520. Available at: https://pubmed.ncbi.nlm.nih.gov/29986520/
- Leyden J, Stephens T, Finkey MB, et al. Skin care benefits of copper peptide containing facial cream (12-week clinical evaluation in photodamaged skin). Cosmetic dermatology clinical study data summarized in Pickart et al. (ref. 1). Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC4508379/
- Philp D, Huff T, Gho YS, Hannappel E, Kleinman HK. The actin binding site on thymosin beta4 promotes angiogenesis. FASEB Journal. 2003;17(14):2103-2105. PMID: 14500546. Available at: https://pubmed.ncbi.nlm.nih.gov/14500546/
- Sikiric P, et al. Stable Gastric Pentadecapeptide BPC 157 and Wound Healing. Frontiers in Pharmacology / PMC. 2021. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8275860/
- Sikiric P, et al. Stable gastric pentadecapeptide BPC 157 in trials for inflammatory bowel disease (PL-10, PLD-116, PL14736, Pliva, Croatia) heals ileoileal anastomosis in the rat. PMID: 17713731. Available at: https://pubmed.ncbi.nlm.nih.gov/17713731/
- U.S. Food and Drug Administration. Bulk Drug Substances Used in Compounding Under Section 503A of the FD&C Act. Available at: https://www.fda.gov/drugs/human-drug-compounding/bulk-drug-substances-used-compounding-under-section-503a-fdc-act
- U.S. Food and Drug Administration. Interim Policy on Compounding Using Bulk Drug Substances Under Section 503A. Available at: https://www.fda.gov/media/174456/download
- Gwyer D, et al. Multifunctionality and Possible Medical Application of the BPC 157 Peptide, Literature and Patent Review. PMC. 2025. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11859134/
- U.S. Food and Drug Administration. Meeting of the Pharmacy Compounding Advisory Committee (BPC-157 bulk drug substance review), July 23-24, 2026. Available at: https://www.fda.gov/advisory-committees/advisory-committee-calendar/july-23-24-2026-meeting-pharmacy-compounding-advisory-committee-07232026
- STAT News. BPC-157: The peptide with big claims and scant evidence. February 3, 2026. Available at: https://www.statnews.com/2026/02/03/bpc-157-peptide-science-safety-regulatory-questions/
- Pickart L. The human tri-peptide GHK and tissue remodeling. Journal of Biomaterials Science, Polymer Edition. 2008;19(8):969-988. Summarized in ref. 1. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC4508379/
- Sarbaziha R, et al. Copper Peptides in Regenerative Aesthetic Dermatology. Dermatological Reviews. 2026. Available at: https://onlinelibrary.wiley.com/doi/abs/10.1002/der2.70067
Disclaimer: This article is provided for educational and research-information purposes only. It is not medical advice and is not intended to diagnose, treat, cure, or prevent any disease. The Glow blend and its component peptides (GHK-Cu, BPC-157, TB-500) are investigational research compounds; they are not approved by the FDA for cosmetic, anti-aging, or any therapeutic use, and the products discussed are intended for laboratory research only and not for human consumption. Nothing here should be interpreted as encouraging personal use. Consult a qualified, licensed healthcare professional before making any decision related to your health.