The question of how Melanotan II “modulates MC1 signaling in pigmentation research” carries a quiet assumption worth surfacing before we examine the biology: that the compound’s relationship to the melanocortin-1 receptor (MC1R) is clean, specific, and well characterized in the way an approved dermatologic drug’s would be. It is not. Melanotan II is a synthetic, non-selective melanocortin agonist that has never been approved by any major regulator for tanning, pigmentation, or any other use, and its human pigmentation data amount to a handful of small early-phase studies from the 1990s.1 What follows is therefore not a product monograph but an honest map of what is genuinely known about the receptor pharmacology, what is inferred from closely related molecules, and where the evidence simply runs out.
The honest framing matters because MC1R signaling in pigmentation is, in fact, one of the better-understood cascades in cutaneous biology — the cyclic-AMP–driven pathway that pushes melanocytes toward brown-black eumelanin has been dissected in molecular detail.2 Melanotan II plugs into the top of that cascade by mimicking the natural ligand, α-melanocyte-stimulating hormone (α-MSH). But two things separate the receptor biology from any claim of a safe, useful tanning agent. First, Melanotan II does not engage MC1R alone; it is a broad agonist across the melanocortin receptor family, which is precisely why its real-world use produces nausea, blood-pressure changes, spontaneous erections, and appetite effects alongside pigmentation.13 Second, chronically driving melanocyte signaling in an uncontrolled, self-administered setting has generated a disturbing case literature of darkening and changing moles, eruptive dysplastic nevi, and melanoma diagnoses in users.1011 This article keeps both the mechanistic elegance and the safety reality in view at once.
To do that properly, we will separate three molecules that popular writing constantly blurs: the natural hormone α-MSH; the FDA-approved, MC1R-selective analog afamelanotide (Melanotan I, marketed as Scenesse); and the unapproved, non-selective research chemical Melanotan II. They share a pharmacophore and a pigmentation mechanism, but they differ sharply in selectivity, evidence, and regulatory standing — and conflating them is the single most common error in this space.
What Melanotan II Is, Structurally and Historically
Melanotan II is a synthetic cyclic heptapeptide analog of α-MSH, the endogenous 13-residue melanocortin peptide cleaved from proopiomelanocortin (POMC).1 The design retains the message sequence that all melanocortin peptides share — the core His-Phe-Arg-Trp motif responsible for receptor recognition and activation — but truncates the natural peptide and locks it into a ring through a lactam bridge between residues, a cyclization that dramatically increases both metabolic stability and receptor potency compared with the linear parent.1 Where native α-MSH is rapidly degraded and modestly potent, the cyclic constraint of Melanotan II holds the pharmacophore in a bioactive conformation, producing a “superpotent” agonist that outlasts and outperforms the natural ligand at the receptor.
The compound emerged from melanoma-prevention research at the University of Arizona in the late 1980s and early 1990s. The original scientific logic was reasonable and, in its own terms, public-health oriented: if a peptide could stimulate the skin’s own protective eumelanin without requiring ultraviolet (UV) exposure, it might reduce the DNA-damaging sun exposure that people with fair skin accumulate while trying to tan. Two related molecules came out of that program — melanotan-I (the linear [Nle&sup4;-D-Phe&sup7;]-α-MSH, later developed as afamelanotide) and the cyclic melanotan-II.14 The two then diverged completely. Melanotan-I was carried forward through legitimate pharmaceutical development toward a narrow, well-defined indication and eventually earned FDA approval as afamelanotide.8 Melanotan II was never developed into an approved product; instead it escaped into the grey market, sold online and through gyms and tanning salons as an unregulated “tanning injection.”9
It is worth dwelling on that fork in the road, because it bears directly on the question this article asks. The pigmentation research on Melanotan II is thin and old precisely because the molecule was abandoned as a pharmaceutical candidate; its non-selectivity made it a poor drug even as it made it a potent tanning agent. The molecule that actually reached patients — afamelanotide — is the selective one. So when someone asks how Melanotan II modulates MC1R signaling “in pigmentation research,” the accurate answer involves a small foundational literature on the compound itself, a much larger and more rigorous literature on the receptor and on its selective cousin, and a cautionary case literature generated almost entirely by unregulated human use rather than by controlled study. For readers tracing the broader evidence base, this site’s companion analysis of what the scientific evidence says about Melanotan II and dermatologic disease follows how these melanocortin compounds are distinguished in the literature.
The Melanocortin System and the Place of MC1R
To understand what “MC1 signaling” means, one has to place MC1R within its family. The melanocortin system comprises five G-protein-coupled receptors, MC1R through MC5R, each with a distinct tissue distribution and physiological role, and all activated by peptides derived from POMC (α-, β-, and γ-MSH and adrenocorticotropic hormone, ACTH).2 MC1R is expressed principally on melanocytes in the skin and hair follicle and governs pigmentation. MC2R is the adrenal ACTH receptor driving cortisol production. MC3R and MC4R are concentrated in the central nervous system and regulate energy balance, appetite, and, relevantly, sexual function and autonomic tone. MC5R has roles in exocrine gland function.2
This anatomy is the key to everything that follows. A perfectly MC1R-selective agonist would, in principle, stimulate pigmentation and little else. A non-selective agonist that also hits MC3R and MC4R will additionally provoke central and autonomic effects — nausea, flushing, blood-pressure shifts, appetite suppression, and penile erection — regardless of the user’s pigmentation intent. Melanotan II is firmly in the second category. Its documented ability to cause spontaneous erections and nausea in the very first human study is not an incidental quirk; it is the predictable signature of a molecule that activates MC4R and MC3R alongside MC1R.1 Two of this site’s companion articles examine those off-target axes in their own right — one on whether Melanotan II influences erectile performance mechanistically and one on its possible role in hypoactive sexual desire disorder — both of which trace back to the same non-selectivity that complicates its pigmentation profile.
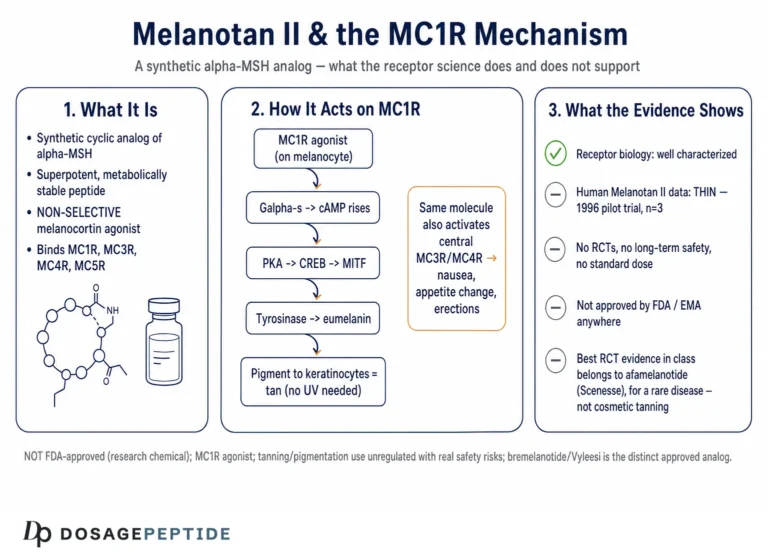
MC1R itself is a Gs-coupled receptor. When an agonist binds, the receptor changes conformation, activates the stimulatory G protein, and switches on adenylate cyclase, raising intracellular cyclic AMP (cAMP).2 That single second-messenger step is the hinge on which the entire pigmentation response turns, and it is where the next section picks up.
How MC1R Signaling Drives Pigmentation: the cAMP–MITF–Tyrosinase Cascade
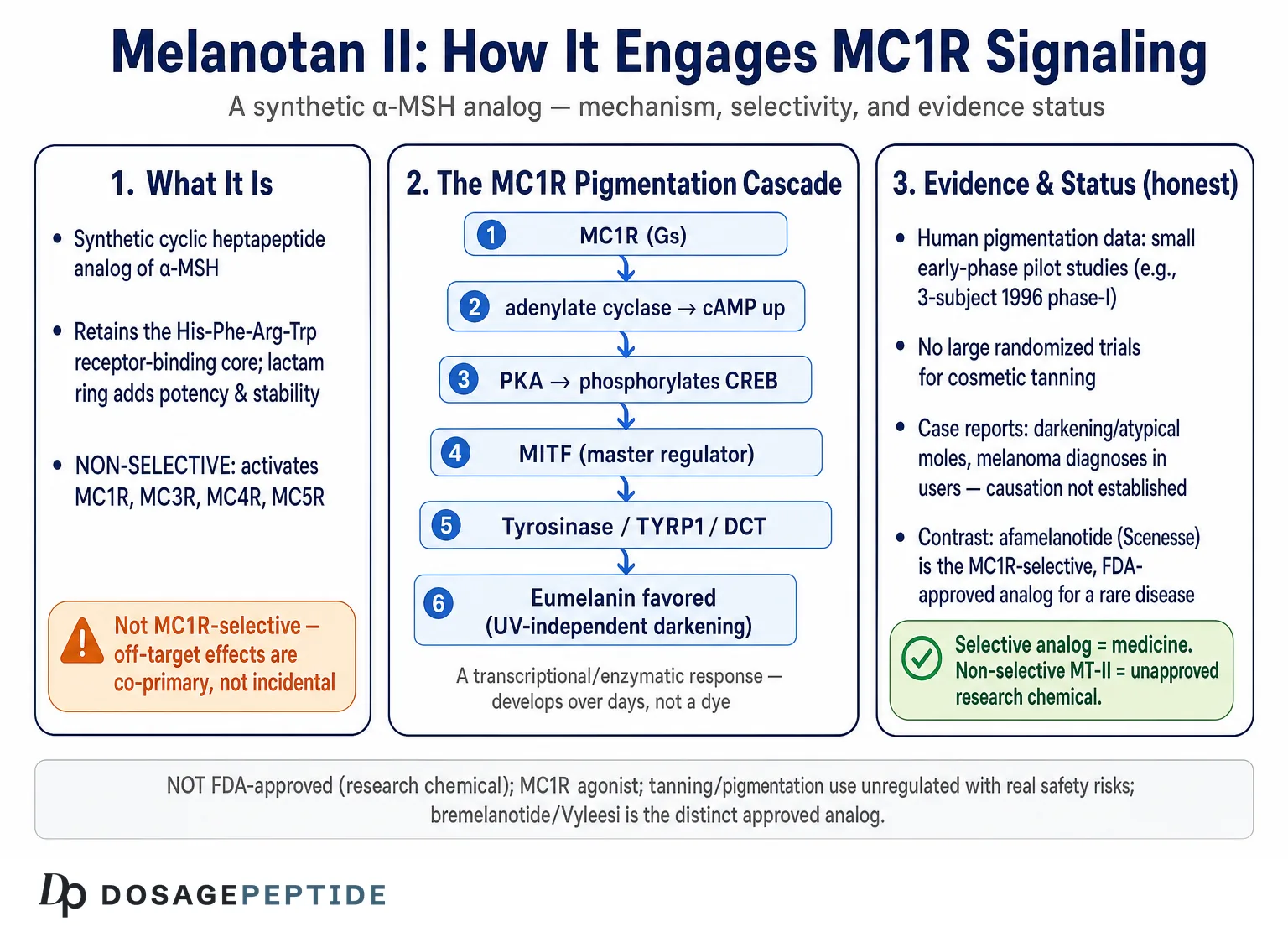
The pigmentation cascade downstream of MC1R is one of the most thoroughly characterized signaling pathways in dermatology, and Melanotan II acts entirely at its front door. The sequence runs as follows. Agonist binding to MC1R activates Gs, which stimulates adenylate cyclase and raises cAMP. Elevated cAMP activates protein kinase A (PKA), which phosphorylates the transcription factor CREB (cAMP response element-binding protein). Phosphorylated CREB, in turn, drives transcription of the master regulator of melanocyte identity and function, microphthalmia-associated transcription factor (MITF).2 MITF then upregulates the enzymatic machinery of melanin synthesis — most importantly tyrosinase (TYR), the rate-limiting enzyme, along with tyrosinase-related protein 1 (TYRP1) and dopachrome tautomerase (DCT/TYRP2).2 The net result is increased production of melanin within melanosomes, which are then transferred to surrounding keratinocytes, darkening the skin.
Crucially, the type of melanin produced depends on the strength and duration of MC1R signaling. Melanocytes make two broad classes of pigment: eumelanin, the brown-black polymer that is photoprotective and absorbs UV efficiently, and pheomelanin, the reddish-yellow pigment that is a poorer sunscreen and can even generate reactive oxygen species under UV.2 Strong, sustained MC1R–cAMP signaling biases the melanocyte toward eumelanin; weak or absent signaling — as occurs with loss-of-function MC1R variants — leaves pheomelanin as the default, producing the fair-skinned, freckled, red-haired, UV-sensitive, melanoma-prone phenotype.2 This eumelanin/pheomelanin switch is the pigmentation biology that a melanocortin agonist is, in principle, exploiting: by supplying a potent, long-acting agonist, Melanotan II pushes the cAMP signal high enough to favor eumelanin synthesis independent of UV exposure.
Several features of this mechanism deserve emphasis for anyone reasoning about Melanotan II specifically. First, the effect is fundamentally a transcriptional and enzymatic one that takes time and depends on the melanocyte’s synthetic capacity; it is not a dye. This is why the early human studies reported pigmentation developing over days to a week or more after dosing rather than immediately.14 Second, because MITF also influences melanocyte proliferation and survival, chronic pharmacological drive of this pathway is not biologically trivial — it is stimulating the same axis whose dysregulation is central to melanocytic neoplasia, a point we return to under safety.7 Third, the pathway’s dependence on cAMP means the response is heavily modulated by the individual’s own MC1R genotype: the same dose of agonist will produce different downstream signaling in a person carrying functional versus loss-of-function receptor variants.2 Readers who want the pathway vocabulary — MITF, tyrosinase, eumelanin, POMC — laid out term by term can consult the site’s peptide and pigmentation glossary.
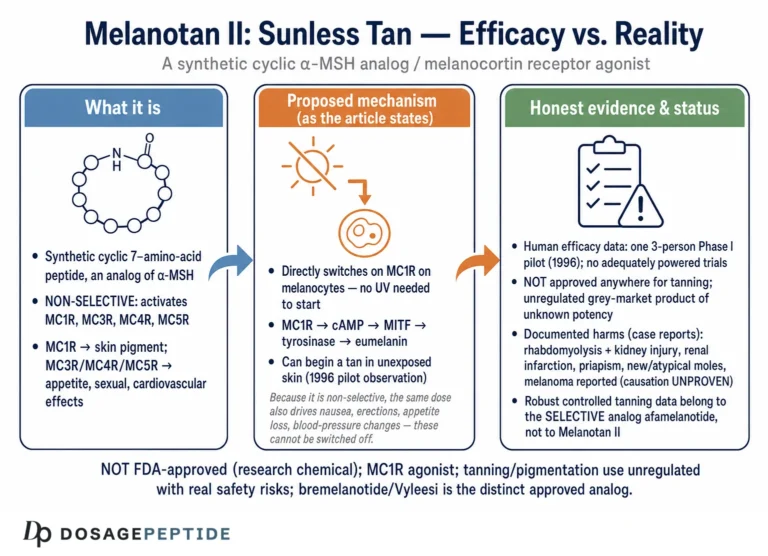
It is illuminating to contrast this pharmacological route with how natural, UV-induced tanning works, because the difference explains both the appeal and the concern surrounding Melanotan II. Physiological tanning is a DNA-damage response: ultraviolet radiation injures keratinocyte DNA, stabilizes the tumor-suppressor p53, and drives keratinocytes to transcribe POMC and secrete α-MSH, which then acts in a paracrine fashion on neighboring melanocyte MC1R to raise eumelanin.2 In that natural loop, pigment production is downstream of, and proportional to, actual UV exposure and its attendant DNA damage — the tan is, in effect, a delayed alarm. A melanocortin agonist short-circuits this loop entirely. Melanotan II supplies the MC1R signal directly and continuously, without the upstream UV insult, which is exactly why proponents frame it as a way to build protective pigment “before” sun exposure. The catch is twofold: the pigment produced still does not confer complete photoprotection, and users frequently combine the agonist with sunbeds or sun to accelerate visible results, reintroducing the very UV damage the mechanism was notionally meant to avoid — a combination that recurs conspicuously in the melanoma case reports.10
A further mechanistic nuance concerns receptor regulation over time. Like other G-protein-coupled receptors, MC1R is subject to desensitization and internalization following sustained agonist exposure, and the melanogenic response is not linear or indefinite; the melanocyte’s synthetic capacity, receptor availability, and feedback regulation all shape how much pigment a given dosing schedule ultimately yields.2 This is one reason the durable, controlled-release delivery used for afamelanotide differs so fundamentally from the intermittent bolus injections typical of grey-market Melanotan II use: the pharmacokinetics of exposure, not just the receptor pharmacology, govern the pigmentary outcome. The table below summarizes the cascade step by step, which is the clearest way to see exactly where an exogenous agonist like Melanotan II intervenes and what it does not control.
| Step | Molecular event | Relevance to Melanotan II |
|---|---|---|
| Ligand binding | Agonist engages MC1R via His-Phe-Arg-Trp core | Melanotan II acts here, mimicking α-MSH with higher potency/stability1 |
| G-protein coupling | Gs activates adenylate cyclase | Same as natural ligand; non-selective across MC receptors2 |
| Second messenger | cAMP rises intracellularly | Magnitude depends on individual MC1R genotype2 |
| Kinase step | PKA activated; phosphorylates CREB | Not directly targeted by the peptide |
| Transcription | CREB drives MITF expression | MITF also governs melanocyte proliferation/survival7 |
| Enzyme induction | MITF upregulates TYR, TYRP1, DCT | Tyrosinase is rate-limiting for melanin2 |
| Pigment output | Eumelanin synthesis favored over pheomelanin | The intended photoprotective, tanning endpoint2 |
Where Melanotan II Sits: a Non-Selective Superagonist
The defining pharmacological fact about Melanotan II — and the one most often omitted from marketing material — is that it is not an MC1R drug. It is a broad melanocortin agonist that activates MC1R, MC3R, MC4R, and MC5R, distinguishing it sharply from afamelanotide, whose activity is functionally centered on MC1R.23 This non-selectivity is not a subtle laboratory detail; it is the reason the compound produces the constellation of systemic effects that dominate its real-world use.
The very first human study made this vivid. In Dorr and colleagues’ 1996 pilot phase-I evaluation — a single-blind, placebo-controlled study in three healthy male volunteers receiving low subcutaneous doses — two subjects developed measurable increases in facial, upper-body, and buttock pigmentation by reflectance and visual assessment about a week after dosing. But alongside the intended pigmentation, the investigators recorded mild nausea at most dose levels and, strikingly, a “stretching and yawning complex” that correlated with the onset of spontaneous penile erections lasting one to five hours.1 Those non-pigmentary effects are MC3R/MC4R-mediated central and autonomic responses. In other words, from the earliest controlled human data, Melanotan II never behaved as a pure pigmentation agent; it behaved as what it is — a pan-melanocortin agonist that happens to tan the skin as one of several simultaneous actions.
Contrast this with the natural ligand and the selective analog. Endogenous α-MSH is a relatively weak, short-lived MC1R agonist under tight physiological control. Afamelanotide is engineered and developed as a functionally MC1R-directed agent delivered as a controlled-release subcutaneous implant under medical supervision for a specific disease.8 Melanotan II occupies the worst-of-both-worlds position for a would-be tanning product: more potent and longer-acting than the natural hormone, but less selective and entirely unsupervised in practice. The following comparison makes the distinctions concrete.
| Molecule | Structure | Receptor selectivity | Regulatory status |
|---|---|---|---|
| α-MSH (endogenous) | Linear 13-residue POMC peptide | Broad melanocortin ligand; physiologically regulated | Natural hormone |
| Afamelanotide (Melanotan-I) | Linear [Nle&sup4;-D-Phe&sup7;]-α-MSH tridecapeptide | Functionally MC1R-directed | FDA-approved (Scenesse) for EPP8 |
| Melanotan II | Cyclic (lactam-bridged) heptapeptide | Non-selective: MC1R, MC3R, MC4R, MC5R | Not approved anywhere; grey-market9 |
| Bremelanotide (Vyleesi) | Cyclic heptapeptide (MT-II analog/metabolite) | Melanocortin agonist, MC4R-oriented | FDA-approved for HSDD in premenopausal women3 |
One further point of genuine scientific interest belongs here: bremelanotide, the FDA-approved drug Vyleesi for hypoactive sexual desire disorder, is a close relative of Melanotan II — essentially a deaminated derivative arising from the same chemistry — developed deliberately toward the MC4R sexual-function axis rather than pigmentation.3 That a legitimate drug was carved out of the same molecular neighborhood by steering toward one receptor arm underscores the central theme: the melanocortin family rewards selectivity, and Melanotan II’s lack of it is exactly why it remained a research chemical rather than becoming a medicine.
What the Pigmentation Research Actually Shows
Having established the mechanism, the honest question is how much of Melanotan II’s pigmentation effect has actually been demonstrated in humans, and at what level of rigor. The answer is sobering: the controlled human pigmentation literature on this specific compound is small, old, and early-phase, and it was never followed by the large randomized trials that would establish efficacy and safety for a tanning indication.
The foundational study remains the 1996 Dorr pilot phase-I trial described above: three subjects, subcutaneous dosing, pigmentation confirmed by quantitative reflectance in two of them, published in Life Sciences.1 It genuinely established proof of concept — that a melanocortin agonist can produce measurable tanning in humans without UV — but three subjects cannot characterize dose-response, durability, inter-individual variability, or safety in any meaningful population sense. The companion pharmacokinetic and pigmentation work on the sister compound melanotan-I (afamelanotide) by Ugwu and colleagues in 1997 similarly involved three male volunteers and established that subcutaneous dosing was fully bioavailable and produced significant, weeks-long tanning of the forehead, arms, and neck.4 These small University of Arizona studies are the empirical bedrock, and they are appropriately described as pilot pharmacology, not as evidence of a safe consumer tanning method.
Two features of that early data are worth extracting because they are so often lost in popular summaries. First, the pigmentation was genuinely UV-independent and durable on the scale of weeks: in the melanotan-I work, tanning of the forehead, arms, and neck peaked around a week after a short dosing course yet persisted for roughly three weeks, consistent with the fact that the response reflects newly synthesized melanin rather than a transient effect.4 Second, the doses that produced tanning were low and weight-based, and even at those low doses the non-pigmentary effects (nausea, erections) appeared — meaning there was never a clean “pigmentation-only” dose window identified in humans.1 That absence of a selective therapeutic window is precisely the kind of finding that, in orthodox drug development, argues against advancing a non-selective compound and in favor of engineering a selective analog instead.
A related gap follows directly from this thin evidence base: because no regulator ever evaluated Melanotan II for pigmentation, there is no established, validated dose for tanning — no defined maximum safe dose, no evidence-based dosing interval, and no course length grounded in controlled human data. The low, weight-based doses used in the 1996 pilot were chosen for an exploratory study in three people, not to define a safe consumer regimen, and even those doses produced systemic effects.1 Any dosing figure circulating in grey-market or online-forum contexts is therefore an extrapolation rather than an evidence-based recommendation, which is itself a core reason the compound cannot honestly be described as having a known therapeutic window or a characterized dose-response for human tanning.
What is striking is what did not follow for Melanotan II. There is no published large randomized controlled trial of the compound for cosmetic tanning, no long-term safety cohort, and no regulatory dossier establishing an approved indication. The rigorous late-stage clinical development in this melanocortin/pigmentation space went to the selective analog: afamelanotide accumulated multicenter randomized placebo-controlled trial evidence — including the two-trial program reported by Langendonk and colleagues in the New England Journal of Medicine in 2015 — but for the narrow indication of increasing pain-free light exposure in erythropoietic protoporphyria (EPP), a rare photodermatosis, not for cosmetic tanning.8 That trial showed afamelanotide increased pain-free sun-exposure time and improved quality of life with an acceptable adverse-event profile, and it supported the drug’s FDA approval in 2019.8
The contrast could not be sharper and it must be stated plainly to avoid overstating Melanotan II’s evidence base: the compound with the robust randomized-trial pigmentation evidence (afamelanotide) is the selective, approved, medically supervised one used for a defined disease; the compound people actually inject to tan (Melanotan II) rests on tiny pilot studies plus an accumulating case literature of harm. Borrowing afamelanotide’s clinical credibility to imply that Melanotan II is a validated tanning agent is a category error. For a focused look at the disease-prevention angle specifically, this site’s companion piece on what the evidence says about Melanotan II and dermatologic disease examines that premise in its own right.
MC1R Polymorphism: Why the Same Peptide Tans People Differently
A genuinely interesting dimension of “MC1 signaling in pigmentation research” — and one where the receptor biology is more solid than the Melanotan II data — is the role of MC1R genetic variation. MC1R is among the most polymorphic genes in humans, and its variants explain much of the natural diversity in skin and hair color and in UV sensitivity.2 Loss-of-function variants (the so-called “red-hair color” or RHC alleles) produce receptors that couple poorly to cAMP, biasing melanocytes toward pheomelanin and yielding fair skin, red or blond hair, freckling, poor tanning ability, and elevated melanoma risk.2
This matters for a melanocortin agonist in two ways that pull in opposite directions. On one hand, the people most motivated to use a chemical tanning agent are often exactly those who tan poorly through UV — fair-skinned individuals, some of whom carry loss-of-function MC1R variants. On the other hand, a receptor that couples poorly to its G protein will, by definition, transduce an agonist’s signal less efficiently; the downstream cAMP rise a given dose of Melanotan II produces is genotype-dependent, so the response is neither uniform nor fully predictable across users.2 The early studies, with their two-of-three responders, hint at exactly this inter-individual variability even before genotype is considered.1
There is a deeper and more cautionary layer. The same fair-skinned, RHC-variant population that responds unevenly to the agonist is also the population at highest baseline melanoma risk.27 Pharmacologically driving a melanocyte signaling pathway — one intimately tied to melanocyte proliferation and to melanoma biology — in precisely the individuals with the greatest melanocytic vulnerability is a combination that should invite caution rather than confidence. This is not a hypothetical concern layered on afterward; it flows directly from the receptor biology. MITF, the transcription factor at the heart of the pigmentation cascade, is also a lineage-survival oncogene in melanoma, and α-MSH/MC1R signaling is a recognized node in melanocyte homeostasis whose dysregulation is implicated in malignant transformation.7 The mechanism that tans is not cleanly separable from the mechanism that, when dysregulated, can drive neoplasia.
Beyond Pigmentation: the Off-Target Melanocortin Effects
Because Melanotan II is non-selective, any honest account of its “MC1 signaling” has to acknowledge that the user never experiences MC1 signaling in isolation. The same injection that raises melanocyte cAMP simultaneously engages central and autonomic melanocortin receptors, and the resulting effects are well documented.
The most consistently reported acute effects are nausea (sometimes with vomiting), facial flushing, appetite suppression, and spontaneous penile erections in men — the last two reflecting MC4R/MC3R activity in the hypothalamus and related circuits.1 Yawning and stretching, again seen in the original phase-I study, are classic centrally mediated melanocortin phenomena.1 These effects are dose-related and, in the grey-market setting, unpredictable because the injected material is of uncertain concentration and purity.
The erectogenic and libido-modulating actions are prominent enough that they became the basis of a separate, legitimate drug-development path — bremelanotide/Vyleesi — and this site treats those axes in dedicated companion articles. The relevant point for pigmentation research is simply that these are not side effects in the trivial sense; they are co-primary pharmacology. A compound cannot be evaluated as a “tanning peptide” as though the sexual, gastrointestinal, and cardiovascular actions were separable noise. They are the direct consequence of the same non-selectivity that makes the molecule a poor pharmaceutical candidate.
Cardiovascular effects deserve particular note. Melanocortin signaling influences autonomic tone and blood pressure, and case reports describe both acute sympathomimetic-type presentations and blood-pressure changes in users.56 In one documented case, a previously normotensive man developed hypertension after months of subcutaneous Melanotan II, with imaging revealing a renal infarction.6 These are not pigmentation phenomena at all, yet they are inseparable from real-world use of the compound.
Safety Signals in the Pigmentation Context
If the mechanistic story is elegant, the safety story is where restraint becomes non-negotiable, because here the concerns bear directly on the pigmentary target tissue itself. Chronic stimulation of melanocytes carries theoretical and, increasingly, empirical risk, and the evidence — while limited to case reports and small series — points in a consistent and worrying direction.
The most pigmentation-specific concern is the behavior of melanocytic nevi (moles). Users and clinicians have repeatedly observed that existing moles darken and that new pigmented lesions appear during Melanotan use, changes that develop within weeks.9 A case report described eruptive dysplastic (atypical) nevi following melanotan use, and dysplastic nevi are recognized melanoma precursors.10 More alarming are the melanoma diagnoses. Ong and Bowling reported melanotan-associated melanoma in situ.11 Hjuler and Lorentzen documented cutaneous melanoma in a 20-year-old woman with fair skin who had used Melanotan II in combination with sunbeds.10 These are individual cases, and causation cannot be established from case reports — but the temporal association, combined with the plausible mechanism (chronic pharmacological drive of a melanocyte proliferation/survival pathway), is exactly the kind of signal that responsible science does not dismiss.7
It is essential to be candid about the limits of this evidence in both directions. No epidemiological study has quantified any relative risk of melanoma from Melanotan II, and no controlled trial has compared cancer rates between users and non-users; the severe outcomes are documented in case reports arising from unregulated use where dose and product quality are uncontrolled.9 So one cannot state that Melanotan II causes melanoma. But one equally cannot claim it is safe for the skin, and the biologically coherent worry — that stimulating melanocytes in high-risk, fair-skinned people who are also using UV sources is precisely the wrong intervention — stands unrefuted. The prudent reading is that anyone using this compound would warrant careful dermatologic surveillance of pigmented lesions, and that the compound’s pigmentary “benefit” and its pigmentary risk arise from the same mechanism.
There is also a subtler, behavioral hazard specific to a tanning agent that is worth naming because it compounds the biological risk. The pigment induced by a melanocortin agonist is real melanin, but it does not equate to a high sun-protection factor, and the degree of added photoprotection is limited and not well quantified for cosmetic use. A darker appearance can nonetheless create a false sense of security, encouraging longer unprotected sun or sunbed exposure — the opposite of the risk reduction the original chemopreventive rationale envisioned. In practice, the melanoma case reports overwhelmingly involve users who paired Melanotan II with deliberate UV tanning, so the compound may act less as a substitute for UV than as an accelerant of the whole high-exposure behavior pattern.910 For a fair-skinned individual carrying loss-of-function MC1R variants, that pattern — chemical melanocyte stimulation plus continued UV plus a false sense of protection — layers three distinct risk multipliers on top of an already elevated baseline.27
Beyond the skin, the systemic case literature reinforces caution. Reported serious events include rhabdomyolysis with acute kidney injury after injection, renal infarction, and priapism, generally in the context of grey-market products and self-dosing.56 An additional and under-appreciated hazard follows directly from the mechanism: because melanocortin agonism also affects mucosal melanocytes, there are reports of new oral mucosal pigmentation associated with Melanotan II, and even discussion of mucosal melanoma risk with nasal-spray formulations.12 The table below organizes the principal documented concerns by system and, importantly, by the strength of the underlying evidence.
A hazard category that is easy to overlook precisely because it is not pharmacological deserves explicit mention: the delivery route and the product itself. Because grey-market Melanotan II is self-injected, the Brennan review catalogued blood-borne and skin infections among the reported harms — the predictable consequence of non-sterile technique and reused injecting equipment rather than of the peptide’s receptor activity.9 Compounding this, material sold as “melanotan” is of undocumented identity, concentration, and purity, so a user cannot know how much peptide, or what contaminants, any given vial contains.9 That uncertainty makes the dose-related effects tabulated above impossible to predict in practice and means the sparse safety signals from the small controlled pilot studies cannot be assumed to transfer to real-world, self-administered exposure.
| Concern | System / mechanism | Evidence level |
|---|---|---|
| Nausea, flushing, appetite loss | Central/autonomic MC3R-MC4R | Consistent in phase-I and case reports1 |
| Spontaneous erections | Hypothalamic MC4R/MC3R | Documented from first human study1 |
| Mole darkening / new nevi | MC1R-driven melanocyte activation | Case reports and clinical observation9 |
| Eruptive dysplastic nevi | Melanocyte proliferation | Case report; precursor lesions10 |
| Melanoma (cutaneous, in situ) | MITF/melanocyte pathway drive | Case reports; causation not established1011 |
| Rhabdomyolysis / renal injury | Sympathomimetic-type systemic toxicity | Case reports56 |
| Renal infarction, hypertension | Autonomic/vascular | Case report6 |
| Oral/mucosal pigmentation | Mucosal melanocyte activation | Case report12 |
Selective versus Non-Selective: the Afamelanotide and Bremelanotide Comparison
The clearest way to understand Melanotan II’s place in pigmentation research is to see it against the two approved melanocortin drugs that flank it. The comparison is not academic; it explains why one molecule became a medicine for pigmentation and another did not.
Afamelanotide (Scenesse) is the pigmentation success story of this family. As a functionally MC1R-directed agonist delivered by a bioresorbable subcutaneous implant under specialist supervision, it increases epidermal eumelanin independent of UV and thereby extends the time patients with erythropoietic protoporphyria can spend in light without triggering the excruciating phototoxic reactions that define their disease.8 It earned European approval in 2014 and FDA approval in October 2019 for that narrow indication, on the strength of randomized controlled trials.8 Notably, afamelanotide is not approved or marketed as a cosmetic tanning agent; even the approved MC1R drug is deployed only for a specific medical need, with the pigmentation effect harnessed as photoprotection rather than aesthetics.
Bremelanotide (Vyleesi) is the other approved relative, and it demonstrates the family’s logic from the opposite direction. Rather than steering toward MC1R and pigmentation, its development steered toward the MC4R sexual-desire axis, and it was approved by the FDA in 2019 for acquired, generalized hypoactive sexual desire disorder in premenopausal women, administered by subcutaneous autoinjector before anticipated activity.3 Its documented efficacy is modest — in the pivotal trials roughly a quarter of treated patients met the desire-score threshold versus about a sixth on placebo — and it carries its own melanocortin-class effects including nausea and transient blood-pressure elevation.3 Both approved drugs, in short, are the products of deliberate receptor targeting.
Melanotan II is the untargeted middle. It hits everything the two approved drugs each hit selectively, which is why it produces both tanning and the sexual/autonomic effects at once, and why it never became a controlled medicine for either. Placing it beside its approved cousins is the most honest single frame for the compound: not a novel or promising therapeutic, but the non-selective ancestor from which selective, approved agents were carved. Researchers cataloging how these compounds are distinguished can find the broader melanocortin landscape organized in the site’s peptide research catalog.
Research Models, Methodology, and Laboratory Handling
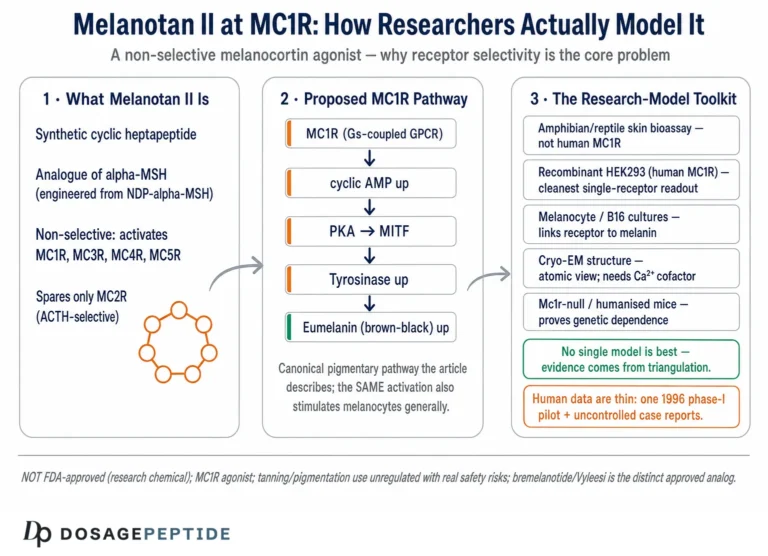
Understanding how MC1R and Melanotan II are actually studied clarifies what the data can and cannot support. The receptor pharmacology is investigated primarily in cell-based systems: MC1R (and the other melanocortin receptors) expressed in heterologous cell lines such as HEK293, where agonist-induced cAMP accumulation is measured directly, and in cultured melanocytes and melanoma cell lines where downstream MITF induction, tyrosinase activity, and melanin content can be quantified.2 These assays are exactly what establish that a peptide is an agonist, its potency, and its receptor selectivity profile, and they are the appropriate tools for characterizing a molecule like Melanotan II. Structure–activity and binding studies, including NMR work on how melanocortin analogs engage MC1R, round out the mechanistic picture.2
Human pigmentation methodology, where it exists for these compounds, has relied on quantitative skin reflectance spectrophotometry to measure melanin density objectively, alongside visual assessment — the approach used in both the Melanotan II and melanotan-I pilot studies.14 Rigorous efficacy methodology, as seen in the afamelanotide EPP program, uses randomized, double-blind, placebo-controlled, multicenter designs with clinically meaningful endpoints such as pain-free light-exposure time and validated quality-of-life instruments.8 The methodological gulf between the two — three-subject pilot pharmacology for Melanotan II versus multicenter RCTs for the selective analog — is itself one of the most important facts a researcher should carry away.
On laboratory handling, a brief and strictly educational note is warranted, with the emphasis that this describes standard research-peptide practice and is not a usage recommendation, and that Melanotan II is not an approved product for human use. Melanotan II is typically encountered as a lyophilized powder. As with other research peptides, lyophilized material is generally reconstituted with sterile or bacteriostatic water directed slowly against the vial wall and mixed by gentle swirling rather than shaking, since vigorous agitation can shear peptide bonds; the diluent volume simply sets the concentration. Reconstituted peptide is generally refrigerated and protected from light, heat, and repeated freeze–thaw cycles, all of which degrade peptides. General reconstitution arithmetic and handling principles are laid out on the site’s peptide reconstitution guide. It bears repeating that meticulous handling changes nothing about the evidence and safety picture: a perfectly reconstituted, high-purity vial is still a non-selective, unapproved compound with a real case literature of harm.
Regulatory Status and the Honest Bottom Line
Melanotan II’s regulatory position is unambiguous and frequently misrepresented. It is not approved as a drug for tanning, pigmentation, or any other indication by the U.S. Food and Drug Administration, the European Medicines Agency, or any comparable regulator. It is sold and used almost entirely through unregulated channels — online vendors, gyms, and tanning salons — as products labeled “melanotan,” often of uncertain identity, concentration, and purity.9 National health authorities in several countries have issued specific warnings against melanotan tanning injections, citing both the lack of safety and efficacy data and the reports of adverse events.9
Two clarifications prevent common misunderstandings. First, the existence of FDA-approved melanocortin drugs does not confer legitimacy on Melanotan II. Afamelanotide (Scenesse) is approved for erythropoietic protoporphyria and bremelanotide (Vyleesi) for hypoactive sexual desire disorder; neither approval covers cosmetic tanning, and neither is Melanotan II.38 Borrowing an approved analog’s status to imply Melanotan II is sanctioned is precisely the conflation this article warns against. Second, the phrase “research chemical,” under which Melanotan II is frequently sold, is a marketing and legal framing, not a safety assurance; it signals the absence of medicinal approval and quality control, not the presence of demonstrated safety.
The honest bottom line, then, is this. The question of how Melanotan II modulates MC1 signaling in pigmentation research has a real and mechanistically satisfying answer at the level of receptor biology: it is a potent, stable, cyclic α-MSH analog that activates MC1R’s Gs–cAMP–PKA–CREB–MITF cascade to favor eumelanin synthesis, producing UV-independent tanning.12 But that clean mechanistic sentence must be surrounded by the fuller truth: the compound is non-selective and therefore inseparable from central and autonomic effects; its human pigmentation evidence is limited to tiny pilot studies rather than the randomized trials that validated its selective cousin; it carries a coherent, mechanism-based melanoma concern in exactly the fair-skinned population most drawn to it; and it is unapproved everywhere, with a case literature of serious harm from unregulated use. The elegant mechanism is real. It is not, on the available evidence, a reason to regard Melanotan II as a safe or validated way to change human pigmentation.
Frequently Asked Questions
How exactly does Melanotan II darken skin at the molecular level?
Melanotan II is a cyclic analog of α-MSH that binds and activates the melanocortin-1 receptor (MC1R) on melanocytes. Activated MC1R couples to the Gs protein, stimulating adenylate cyclase and raising cyclic AMP, which activates protein kinase A and phosphorylates the transcription factor CREB. CREB drives expression of MITF, the master melanocyte regulator, which upregulates tyrosinase and related enzymes and biases the cell toward producing brown-black eumelanin rather than reddish pheomelanin.2 The net effect is increased melanin and darker skin, developing over days because it is a transcriptional and enzymatic process, not an immediate dye.1
Is Melanotan II selective for MC1R?
No, and this is central. Melanotan II is a broad melanocortin agonist that activates MC1R, MC3R, MC4R, and MC5R.2 That non-selectivity is why real-world use produces nausea, flushing, appetite suppression, blood-pressure changes, and spontaneous erections alongside pigmentation — effects mediated by MC3R and MC4R in the brain and autonomic system, documented from the very first human study.1 The approved MC1R drug afamelanotide is far more selective, which is one reason it became a medicine and Melanotan II did not.
Is Melanotan II FDA-approved for tanning?
No. Melanotan II is not approved by the FDA, the EMA, or any comparable regulator for tanning, pigmentation, or any other use, and it is sold almost entirely through unregulated channels as a “research chemical” of uncertain purity.9 The FDA-approved melanocortin drugs are different molecules for different indications: afamelanotide (Scenesse) for erythropoietic protoporphyria and bremelanotide (Vyleesi) for hypoactive sexual desire disorder.38
How strong is the human evidence that Melanotan II tans skin?
The controlled human pigmentation evidence for this specific compound is limited to small early-phase pilot work, principally a 1996 phase-I study in three subjects that confirmed tanning by reflectance in two of them.1 There is no large randomized controlled trial of Melanotan II for cosmetic tanning. The robust randomized-trial pigmentation evidence in this family belongs to the selective analog afamelanotide, and only for the rare disease erythropoietic protoporphyria, not for tanning.8
Does Melanotan II cause melanoma?
This cannot be stated as established fact, and it cannot be dismissed either. Multiple case reports document darkening moles, eruptive dysplastic nevi (melanoma precursors), and melanoma diagnoses in Melanotan users, and there is a coherent mechanism — chronic pharmacological drive of the MC1R/MITF melanocyte pathway, which is central to melanoma biology.71011 However, no epidemiological study or controlled trial has quantified the risk.9 The prudent interpretation is that the compound warrants serious caution, especially in fair-skinned, high-risk individuals, and that anyone exposed would merit careful dermatologic monitoring of pigmented lesions.
Why is bremelanotide (Vyleesi) approved but Melanotan II is not?
Bremelanotide is a close relative of Melanotan II that was deliberately developed toward the MC4R sexual-function axis and taken through the formal clinical-trial and approval process for a defined indication, hypoactive sexual desire disorder.3 Melanotan II was never developed into an approved product; its non-selectivity made it a poor pharmaceutical candidate, and it entered use through grey-market channels rather than through regulated development. The difference is targeted development and regulatory review, not merely chemistry.
How does MC1R genotype affect the response to Melanotan II?
MC1R is highly polymorphic, and loss-of-function “red-hair color” variants couple poorly to cAMP, producing fair skin, freckling, poor UV tanning, and higher melanoma risk.2 Because the pigmentation response depends on cAMP generated downstream of the receptor, the same dose of a melanocortin agonist will transduce differently across genotypes, contributing to variable and unpredictable responses. This is compounded by the fact that the fair-skinned population most likely to seek chemical tanning is also the population at highest melanoma risk.27
What are the non-pigmentary risks reported with Melanotan II?
Beyond the skin, case reports describe rhabdomyolysis with acute kidney injury after injection, renal infarction with new hypertension, priapism, and sympathomimetic-type systemic toxicity, generally in the setting of unregulated products and self-dosing.56 There are also reports of new oral and mucosal pigmentation.12 These reflect the compound’s broad melanocortin activity and the uncontrolled quality of grey-market material, and they are inseparable from real-world use.
How is Melanotan II handled in a research laboratory setting?
As a lyophilized powder, it is reconstituted with sterile or bacteriostatic water using gentle technique (swirl, do not shake), stored refrigerated after reconstitution, and protected from light, heat, and freeze–thaw cycles — standard research-peptide practice described on educational reconstitution pages.4 Careful handling preserves peptide integrity but has no bearing on the compound’s non-selectivity, its lack of approval, or the documented safety concerns; it is not a usage recommendation.
References
- Dorr RT, Lines R, Levine N, et al. Evaluation of melanotan-II, a superpotent cyclic melanotropic peptide in a pilot phase-I clinical study. Life Sci. 1996;58(20):1777-1784. PMID: 8637402. https://pubmed.ncbi.nlm.nih.gov/8637402/
- Wolf Horrell EM, Boulanger MC, D’Orazio JA. Melanocortin 1 Receptor: Structure, Function, and Regulation. Front Genet. 2016;7:95. PMID: 27303435; PMCID: PMC4885833. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4885833/
- U.S. Food and Drug Administration. VYLEESI (bremelanotide injection) prescribing information; Initial U.S. Approval 2019. https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/210557s000lbl.pdf
- Ugwu SO, Blanchard J, Dorr RT, et al. Skin pigmentation and pharmacokinetics of melanotan-I in humans. Biopharm Drug Dispos. 1997;18(3):259-269. PMID: 9113347. https://pubmed.ncbi.nlm.nih.gov/9113347/
- Nelson ME, Bryant SM, Aks SE. Melanotan II injection resulting in systemic toxicity and rhabdomyolysis. Clin Toxicol (Phila). 2012;50(10):1169-1173. PMID: 23121206. https://pubmed.ncbi.nlm.nih.gov/23121206/
- Peters I, Hadimeri H, Ohlsson S, et al. Melanotan II: a possible cause of renal infarction: review of the literature and case report. CEN Case Rep. 2020;9(2):159-161. PMCID: PMC7148395. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7148395/
- Dall’Olmo L, Papa A, Surdo NC, et al. Alpha-melanocyte stimulating hormone (α-MSH): biology, clinical relevance and implication in melanoma. J Transl Med. 2023;21(1):562. PMCID: PMC10463388. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10463388/
- Langendonk JG, Balwani M, Anderson KE, et al. Afamelanotide for Erythropoietic Protoporphyria. N Engl J Med. 2015;373(1):48-59. PMID: 26132941. https://pubmed.ncbi.nlm.nih.gov/26132941/
- Brennan R, Wells JSG, Van Hout MC. An unhealthy glow? A review of melanotan use and associated clinical outcomes. Perform Enhanc Health. 2014;3(2):78-92. https://www.sciencedirect.com/science/article/abs/pii/S2211266915000055
- Hjuler KF, Lorentzen HF. Melanoma associated with the use of melanotan-II. Dermatology. 2014;228(1):34-36. PMID: 24355990. https://pubmed.ncbi.nlm.nih.gov/24355990/
- Ong S, Bowling J. Melanotan-associated melanoma in situ. Australas J Dermatol. 2012;53(4):301-302. PMID: 22724573. https://pubmed.ncbi.nlm.nih.gov/22724573/
- Changes in Oral Mucosa Associated with Melanotan II Injections: A Case Report. Life (Basel). 2026. PMCID: PMC12942211. https://pmc.ncbi.nlm.nih.gov/articles/PMC12942211/
- U.S. Food and Drug Administration. SCENESSE (afamelanotide) implant, for subcutaneous use — prescribing information; Initial U.S. Approval October 2019 for erythropoietic protoporphyria. https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/210797s000lbl.pdf
Educational and research-use disclaimer: This article is provided solely for scientific and educational purposes. Melanotan II is not approved by the FDA, EMA, or any comparable regulator for tanning, pigmentation, or the treatment, cure, or prevention of any disease, and it is a non-selective melanocortin agonist commonly sold through unregulated channels of uncertain quality. Documented concerns include nausea and blood-pressure effects, systemic toxicity, and darkening or changing melanocytic nevi with melanoma reported in case literature; anyone exposed would warrant careful dermatologic monitoring. The distinct, FDA-approved melanocortin analogs afamelanotide (Scenesse) and bremelanotide (Vyleesi) are different molecules approved only for specific medical indications, not for cosmetic tanning. Nothing here is medical advice or a recommendation for human use. Readers should consult qualified professionals and applicable regulations before making any decisions.