Peptide storage guidance for reconstituted tesamorelin is one of the most consequential and least-appreciated variables in a research program, because the moment a lyophilized tesamorelin cake meets its diluent, every degradation pathway that freeze-drying had frozen in place reactivates at once. This reference examines the stability science of tesamorelin — a 44-amino-acid growth hormone–releasing hormone (GHRH) analog — from the perspective of what actually happens to the molecule during storage and handling: how the dry powder behaves versus the solution, which chemical degradation routes dominate (deamidation, methionine oxidation, aggregation, and surface adsorption), and how temperature, light, diluent choice, pH, and container material each move the needle. Throughout, material discussed here is framed as research-use-only; the approved tesamorelin product (Egrifta) is a distinct, quality-controlled pharmaceutical and nothing below is human dosing or medical advice.
What is tesamorelin, and why does its structure matter for stability?
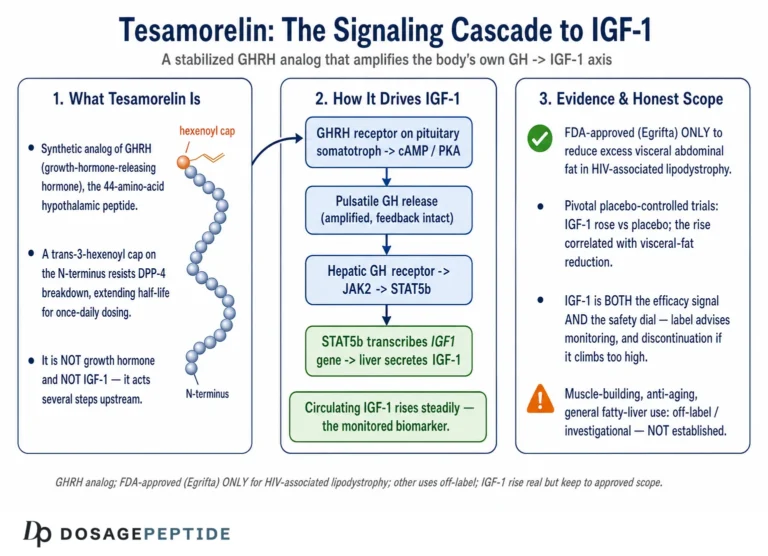
Tesamorelin is a synthetic analog of endogenous human growth hormone–releasing hormone, comprising the full 44-residue hGRF(1–44) sequence with a single N-terminal modification. It is chemically designated N-(trans-3-hexenoyl)-[Tyr1]-hGRF(1–44)-NH2 acetate. Two structural features distinguish it from native GHRH and directly govern both its pharmacology and its stability profile: a trans-3-hexenoic acid moiety attached at the N-terminus, and C-terminal amidation. The hexenoyl cap sterically protects the molecule against rapid cleavage by dipeptidyl peptidase-4 (DPP-4) and serum peptidases, extending plasma half-life without altering receptor binding, while the C-terminal amide further reduces exopeptidase susceptibility.[1]
The free-base molecular weight is approximately 5,136 daltons (the acetate salt form is closer to 5,579 Da, reflecting an average of roughly 7.4 acetate counter-ions per peptide), and the molecular formula of the acetate is C221H366N72O67S • x C2H4O2.[2] That single sulfur atom is not incidental — it belongs to a methionine residue, and methionine is one of the two most oxidation-prone amino acids in any peptide. The full amino acid sequence (N→C) is: Tyr-Ala-Asp-Ala-Ile-Phe-Thr-Asn-Ser-Tyr-Arg-Lys-Val-Leu-Gly-Gln-Leu-Ser-Ala-Arg-Lys-Leu-Leu-Gln-Asp-Ile-Met-Ser-Arg-Gln-Gln-Gly-Glu-Ser-Asn-Gln-Glu-Arg-Gly-Ala-Arg-Ala-Arg-Leu-NH2. Reading that sequence tells a chemist immediately where the molecule is vulnerable: a methionine at position 27 (Met27), multiple asparagine and glutamine residues (Asn8, Asn35, and a cluster of Gln), and a high proportion of basic residues (arginine and lysine) that make the peptide cationic at neutral pH — a property that promotes adsorption to negatively charged glass surfaces.
For a grounding in tesamorelin’s identity, receptor biology, and research context beyond stability, see our companion overview of what tesamorelin is and how it works. The remainder of this article assumes that background and focuses on the storage, stability, and handling science.
How does tesamorelin act on the growth hormone axis?
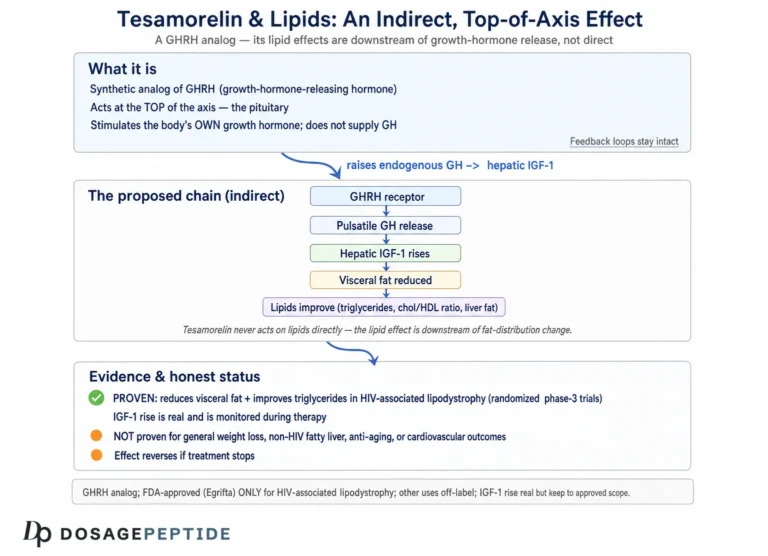
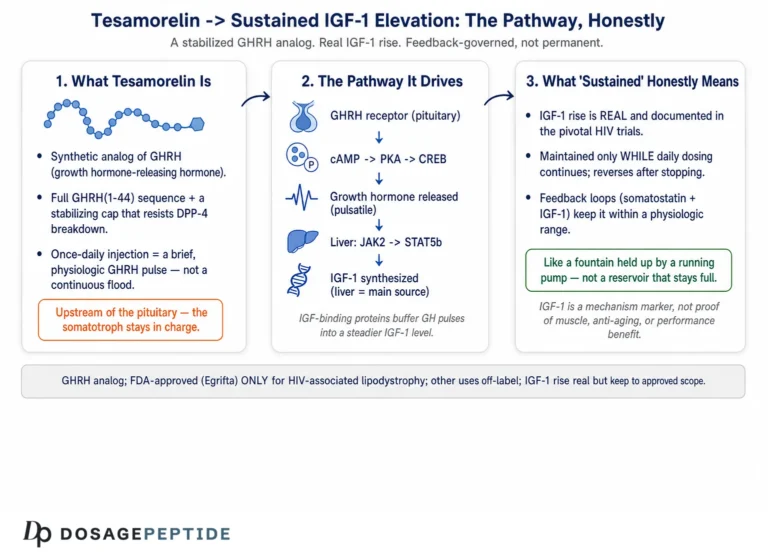
Mechanistically, tesamorelin is a GHRH-receptor (GHRH-R) agonist. GHRH-R is a class B (secretin-family) G-protein-coupled receptor expressed predominantly on somatotroph cells of the anterior pituitary. Binding activates adenylyl cyclase via the stimulatory G-protein Gs, raising intracellular cyclic AMP, activating protein kinase A, and driving both the synthesis and the calcium-dependent pulsatile release of endogenous growth hormone (GH). The released GH acts on hepatocytes and peripheral tissues through the GH receptor and the JAK2–STAT5 pathway, stimulating production of insulin-like growth factor-1 (IGF-1) and its principal carrier IGF-binding protein-3 (IGFBP-3).[1] Because tesamorelin works upstream by amplifying the body’s own pulsatile GH secretion rather than replacing GH directly, it largely preserves the physiologic feedback architecture — somatostatin tone and IGF-1 negative feedback still restrain the axis — and IGF-1 therefore serves as the standard downstream pharmacodynamic marker of on-target activity in research.
This mechanistic detail is precisely why stability matters at the molecular level. GHRH-R recognition depends on tesamorelin adopting an amphipathic alpha-helix in which specific residues project toward the receptor-binding cleft. The N-terminal region is critical for receptor activation, and the central helix — which contains Met27 — contributes to binding affinity and helical stability. An oxidized methionine or a deamidated asparagine introduces a charge or steric change that can unwind local helix and reduce GHRH-R affinity, so a solution can lose biological signal well before it loses measurable peptide mass. A crude total-nitrogen or total-peptide assay would call such a sample “intact” while a receptor-binding or IGF-1-induction assay would show it had partly failed — the central reason activity-relevant analytics, not mass alone, define real stability.
What is the regulatory status of tesamorelin in 2026?
Tesamorelin is an FDA-approved active pharmaceutical ingredient. It was first approved in the United States in 2010 under the trade name Egrifta for the reduction of excess visceral abdominal fat in adults with HIV-associated lipodystrophy.[2] As of 2025–2026 the approved formulation landscape has evolved: on March 25, 2025 the FDA approved the F8 formulation, marketed as Egrifta WR, which requires only weekly reconstitution and less than half the injection volume of the earlier daily-reconstitution formulations; it became commercially available in September 2025 and is gradually replacing the F4 Egrifta SV product.[3]
The critical distinction for a research context: the approved products are manufactured, formulated, packaged, and quality-controlled to pharmaceutical specifications, and their labels carry indication-specific dosing. Research-grade tesamorelin sold for laboratory use is not the approved drug — it is not FDA-approved for human therapeutic use, is intended for in-vitro and non-clinical research only, and is not manufactured to the same finished-product controls. Everything in this article describing storage and handling is written for that research-use-only material. Where the approved-product label provides stability data, we cite it because it is the highest-quality public source on how this specific molecule behaves — but the label’s handling instructions apply to the finished pharmaceutical, not to bulk research powder.
Why are lyophilized peptides so much more stable than solutions?
Tesamorelin, like nearly all research peptides, is supplied as a lyophilized (freeze-dried) powder for one overriding reason: water is the medium in which almost every chemical degradation reaction proceeds. Remove the water and you remove the reaction medium. Lyophilization is a three-stage process — freezing, primary drying (sublimation of ice under vacuum), and secondary drying (desorption of bound water) — that reduces residual moisture to a low single-digit percentage, transforming a labile solution into a comparatively inert amorphous solid.[4]
In the dried glassy state, molecular mobility is drastically restricted. Hydrolysis of the peptide backbone requires water; deamidation requires water and mobility; oxidation, while it can occur in the solid state, is slowed by the absence of a solvation shell and reduced diffusion of dissolved oxygen. The practical consequence is a difference of orders of magnitude in shelf life: a properly lyophilized peptide with sub-1% residual moisture, stored cold and dark, can remain within specification for years, whereas the same molecule in aqueous solution at room temperature may lose meaningful potency within hours to days.
What is residual moisture, and why is it the second most important quality attribute?
After chemical purity, residual moisture content is arguably the single most important attribute of a lyophilized peptide, because it directly controls how “solid” the solid really is. The glass transition temperature (Tg) of the dried cake must remain comfortably above the storage temperature; if Tg falls to or below storage temperature, the amorphous matrix softens or collapses, molecular mobility returns, and degradation accelerates. Residual moisture is the dominant plasticizer: as moisture rises, Tg falls. Formulation scientists report that the difference between roughly 1% and 3% residual moisture can be the difference between a multi-year and a several-month shelf life for otherwise identical material.[4] This is also why an unsealed or repeatedly opened vial in a humid environment degrades faster than the label suggests — the powder is hygroscopic and pulls water from ambient air, raising moisture and lowering Tg with each exposure.
What roles do lyoprotectants and bulking agents play?
Freeze-drying itself is a stress. Ice-crystal formation concentrates the peptide and any buffer salts into the freeze-concentrate, exposing the molecule to pH shifts and high local ionic strength, and the drying step removes the hydration shell that stabilizes native conformation. Excipients mitigate these stresses through two distinct functions: cryoprotection (protection during freezing) and lyoprotection (protection during drying). No single excipient optimally serves both, which is why formulators frequently use binary systems. Among sugars, trehalose is generally regarded as superior to sucrose, glucose, and dextran as a cryoprotectant, because it forms a stable glassy matrix and can hydrogen-bond to the peptide in place of water (the “water-replacement” hypothesis).[5] Bulking agents such as mannitol give the cake mechanical structure. Research-grade tesamorelin may be supplied as a relatively pure salt with minimal excipient, whereas the approved product includes a defined excipient system (for example, mannitol as a bulking agent) — another reason research powder and finished drug should not be assumed to behave identically.
What are the main degradation pathways of reconstituted tesamorelin?
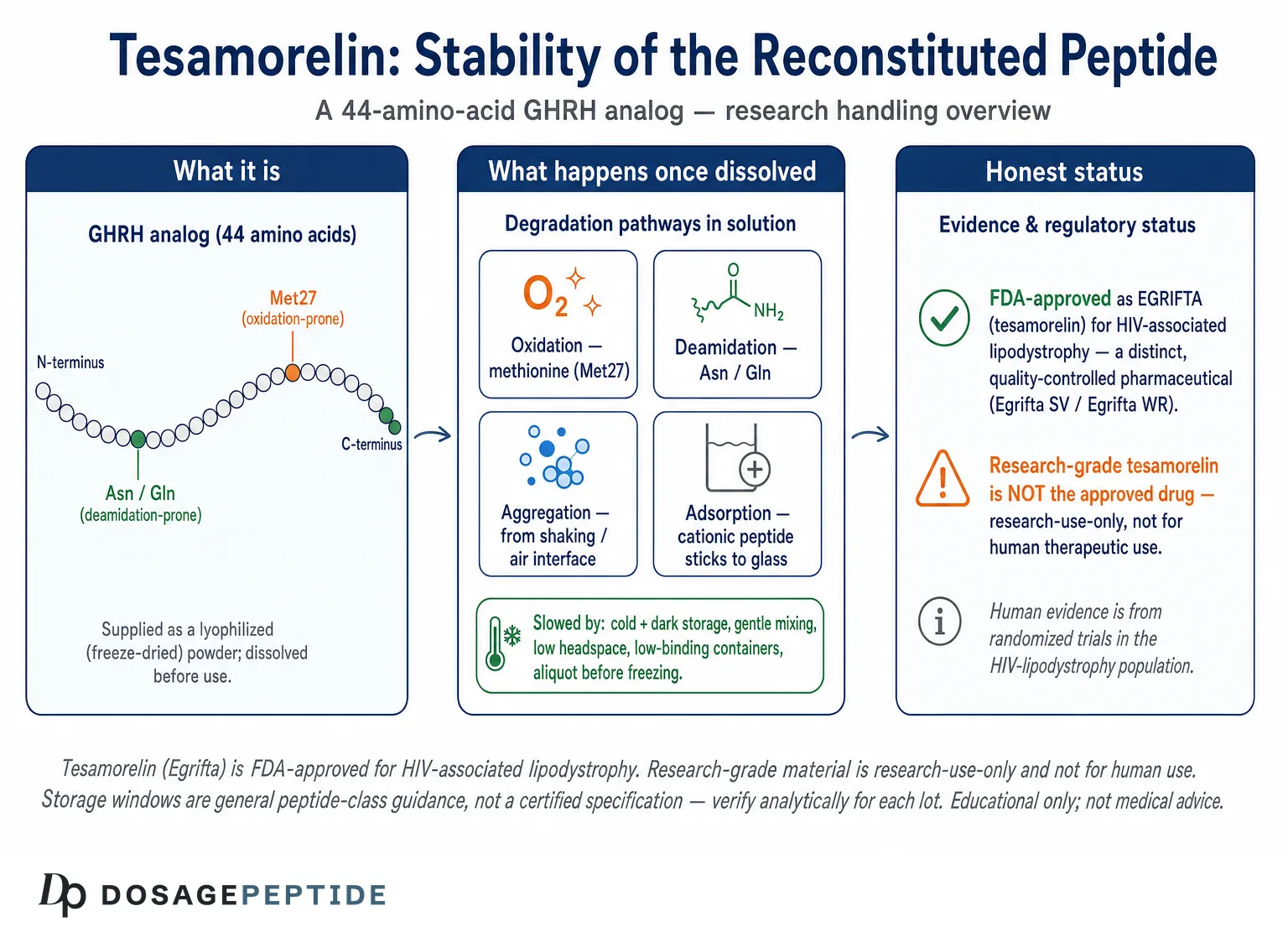
Once tesamorelin is dissolved, four classes of degradation compete, and the sequence of the molecule tells us which will dominate. Understanding these pathways is what turns storage guidance from a list of rules into a set of reasoned choices.
Deamidation of asparagine and glutamine
Deamidation is the hydrolytic conversion of an asparagine (Asn) or glutamine (Gln) side-chain amide to a carboxylic acid, generating aspartate/iso-aspartate or glutamate respectively. It is one of the most common and best-characterized non-enzymatic degradation routes for peptides in solution. The reaction is strongly pH-dependent — accelerated under neutral-to-alkaline conditions — and sequence-dependent, with Asn followed by small residues (Asn-Gly, Asn-Ser) being especially labile because they readily form the cyclic succinimide intermediate.[6] Tesamorelin carries an Asn8-Ser9 motif and a cluster of glutamines; deamidation at these positions alters local charge and can perturb the alpha-helix, degrading receptor recognition. Because deamidation accelerates with pH, a mildly acidic solution environment slows it — one reason researchers favor slightly acidic reconstitution conditions for stability-sensitive work.
Oxidation of methionine (Met27)
Methionine is oxidized to methionine sulfoxide, and under harsher conditions to the sulfone, by molecular oxygen, peroxides, light, and trace transition-metal contaminants. For tesamorelin, Met27 sits within the receptor-binding helix, so its oxidation is not cosmetic — it disrupts the secondary structure required for GHRH-R engagement.[6] There are two mechanistically distinct oxidation routes worth separating. The first is simple aerobic oxidation, in which dissolved molecular oxygen slowly converts the thioether sulfur to a sulfoxide; this is favored by ample headspace air, warm temperature, and long dwell time in solution. The second is metal-catalyzed oxidation, in which trace transition metals such as iron and copper — leached from water, glass, or stainless steel, or present as reagent contaminants — drive a site-specific, radical-mediated oxidation that can be far faster than the aerobic route. Light adds a third accelerant through photo-oxidation. Because these routes are additive, the highest-risk scenario for tesamorelin is a warm, well-aerated, brightly-lit solution prepared with metal-contaminated water — and each of those factors is individually controllable.
Practical mitigations used in careful research handling therefore target each accelerant: minimizing vial headspace (or overlaying with an inert gas such as nitrogen or argon where the workflow permits) reduces the oxygen reservoir; using high-purity, low-metal water and, where feasible, freshly deoxygenated diluent limits both aerobic and metal-catalyzed routes; a metal chelator such as EDTA is sometimes added to sequester catalytic metals when the downstream assay tolerates it; and rigorous light exclusion (amber glass, foil, dark storage) curbs photo-oxidation. General peptide-formulation practice pairs these with cold, short-window storage, since lower temperature slows every one of these reactions.
Aggregation and adsorption
Aggregation is the association of peptide monomers into dimers, higher oligomers, and eventually insoluble particulates, driven by hydrophobic and electrostatic interactions and dramatically promoted at air–liquid interfaces and by agitation. This is precisely why vigorous shaking, frothing, and foam are to be avoided during reconstitution: the air–water interface is a nucleation surface for unfolding and aggregation. Adsorption is a related but distinct loss route: the peptide simply sticks to container surfaces. Cationic peptides — and tesamorelin, with its multiple arginines and lysines, is cationic at neutral pH — adsorb strongly to negatively charged silanol groups on borosilicate glass and to some plastics. In a controlled study of three cationic peptides across common glass and plastic containers, 90% or more of the peptide could be lost from dilute solution to container walls.[7] At the low concentrations used in many binding or cell assays, adsorption is often the single largest and most underestimated source of “disappeared” peptide, corrupting apparent potency and dose–response data even when the molecule itself is chemically intact.
Hydrolysis and physical degradation
Backbone hydrolysis — cleavage of peptide bonds — is generally slower than deamidation and oxidation for a molecule like tesamorelin under refrigerated conditions, but it becomes relevant at elevated temperature and extreme pH, with aspartate-adjacent bonds (Asp-Pro, Asp-Gly) being classic hot spots. Physical instabilities — precipitation, gel formation, and visible particulates — are the endpoint of aggregation and are a signal that the solution should be discarded rather than used, since aggregated peptide is both inactive and analytically confounding.
| Degradation pathway | Molecular target in tesamorelin | Main accelerators | Primary mitigation in research handling |
|---|---|---|---|
| Deamidation | Asn8, Gln cluster, Asn35 | Neutral–alkaline pH, heat, time in solution | Mildly acidic solution, cold storage, short in-use window |
| Oxidation | Methionine (Met27; also reported Met42 in some analyses) | Dissolved O2, light, trace metals, heat | Exclude light, minimize headspace, deoxygenated diluent, cold |
| Aggregation | Hydrophobic helical faces; air–water interface | Agitation/shaking, foaming, freeze–thaw, high concentration | Gentle mixing (roll/swirl), avoid repeated freeze–thaw |
| Adsorption | Cationic Arg/Lys residues vs. glass silanols | Low concentration, glass surfaces, large surface area | Low-binding polypropylene, carrier protein where assay allows |
| Hydrolysis | Backbone amide bonds (Asp-adjacent hot spots) | Extreme pH, high temperature | Near-neutral-to-mildly-acidic pH, cold storage |
How do temperature, light, and freeze–thaw affect stored tesamorelin?
The three physical stressors researchers control most directly are temperature, light, and freeze–thaw cycling. Each maps onto the chemistry above.
Temperature
Reaction rates for deamidation, oxidation, and hydrolysis all rise with temperature, roughly following Arrhenius behavior, so temperature is the master variable. For the lyophilized powder, cold storage extends shelf life dramatically: general peptide-stability guidance places years of stability at −20°C (or colder) for dry material with low residual moisture, versus much shorter windows at ambient temperature.[8] For reconstituted solution, the hierarchy is stark: refrigerated (2–8°C) solution is stable for days to a few weeks depending on the peptide and buffer, whereas room-temperature solution may hold for only hours to a couple of days, with a large fraction of the total degradation occurring within the first 72 hours before settling into a slower steady-state rate.[9]
It is worth noting the counter-intuitive instruction on the approved Egrifta SV label: after reconstitution with the supplied Sterile Water for Injection, the finished product is not to be refrigerated or frozen — it is administered promptly and stored at controlled room temperature only briefly.[2] That instruction reflects a preservative-free, single-use finished-product design intended for immediate use, not a claim that cold is bad for the molecule. In a research context where a solution must be held and re-sampled over days, refrigeration slows the chemistry — the two situations answer different questions.
Light
Ultraviolet and even visible light drive photo-oxidation of methionine, tryptophan, and tyrosine and can accelerate aggregation. Tesamorelin contains oxidation-sensitive methionine and multiple tyrosines, so light exclusion is a low-cost, high-value control. Amber vials, foil-wrapping, and dark storage (a closed freezer or refrigerator) are standard.[8]
Freeze–thaw cycling
Freezing a peptide solution is not free stabilization. Each freeze–thaw cycle concentrates the peptide and buffer into the shrinking liquid phase, generates ice–water interfaces, and produces transient pH shifts as buffer components crystallize at different rates — all of which promote aggregation and unfolding. The consensus practice is therefore to aliquot a reconstituted stock into single-use portions before freezing, so each experiment thaws a fresh aliquot exactly once rather than subjecting the whole stock to repeated cycling.[9] This single practice often does more to preserve usable potency across a multi-week study than any other handling decision.
| State | Typical storage | General stability window* | Dominant risk if mishandled |
|---|---|---|---|
| Lyophilized powder, sealed | −20°C or colder, desiccated, dark | Months to years | Moisture uptake (Tg drop), oxidation over long term |
| Lyophilized powder, opened repeatedly | −20°C, desiccated | Reduced vs. sealed | Hygroscopic water gain, condensation on cold vial |
| Reconstituted, refrigerated | 2–8°C, dark | Days to a few weeks | Deamidation, oxidation, adsorption |
| Reconstituted, room temperature | 20–25°C | Hours to ~1–2 days | Rapid oxidation/deamidation, microbial risk |
| Reconstituted, frozen aliquots | −20 to −80°C, single-use | Weeks to months (peptide-dependent) | Freeze–thaw aggregation if re-cycled |
*General peptide-class guidance, not a tesamorelin-specific certified specification. Actual stability depends on purity, buffer, concentration, container, and must be verified analytically for any given lot and protocol.
Which diluent should be used to reconstitute tesamorelin in research?
Diluent choice affects sterility, pH, and therefore chemical stability, and it is one of the most frequently debated handling decisions. The two most common options are bacteriostatic water and sterile water; acidic diluents are sometimes used for solubility- or stability-sensitive work. For a fuller walkthrough of the mechanics of dissolving a lyophilized vial, see our peptide reconstitution guide.
Bacteriostatic water versus sterile water
Bacteriostatic water for injection is sterile water containing 0.9% benzyl alcohol as a bacteriostatic preservative. The benzyl alcohol does not kill bacteria outright but inhibits their growth, which allows repeated withdrawals from a single multi-use vial over an extended window (commonly cited as up to 28 days) without the contamination risk that an unpreserved solution carries once opened.[10] Sterile water for injection contains no preservative; it is appropriate when the entire reconstituted vial will be consumed in a single session, but once opened it offers no ongoing protection against microbial growth. The general research logic is straightforward: if a stock will be sampled repeatedly over days, a bacteriostatic diluent addresses the microbial dimension of stability that refrigeration alone does not; if a vial is single-use, sterile water suffices.
Importantly, the approved Egrifta products specify Sterile Water for Injection as the supplied diluent and are designed for prompt use rather than multi-day multi-withdrawal storage.[2] That is a finished-product design decision and does not translate to a universal rule for research handling, where the storage question is different.
Does pH matter, and what about acidic diluents?
Yes — pH is a lever on deamidation in particular, which accelerates as pH rises toward and above neutrality. A mildly acidic solution environment (roughly pH 4–5) slows deamidation and can improve the solubility of some peptides, which is why dilute acetic acid is sometimes used as a reconstitution or pre-wetting solvent for stability- or solubility-challenged peptides.[6] There is a trade-off: excessively acidic conditions and elevated temperature can promote acid-catalyzed backbone hydrolysis, and the acetate counter-ion already present in tesamorelin acetate means the salt form is compatible with mildly acidic handling. Any diluent decision in research should be validated analytically for the specific molecule and downstream assay rather than assumed.
Concentration, carrier protein, and adsorption control
Because tesamorelin is cationic and adsorbs to container walls, the stock concentration and container are part of the “diluent” decision. Preparing a more concentrated stock and diluting into assay buffer immediately before use reduces the residence time of dilute peptide against surfaces. Where the downstream assay tolerates it, a small amount of carrier protein (for example, low-percentage bovine serum albumin) competitively occupies adsorption sites and markedly improves recovery of dilute cationic peptides — a technique validated by the finding that low-binding surfaces and blocking agents rescue the 80–90% losses seen with bare glass.[7]
Microbial and endotoxin considerations in stored solution
Chemical stability is only half of the storage question; biological contamination is the other. An unpreserved reconstituted solution is a nutrient-poor but not sterile-forever medium, and once a vial is entered, each withdrawal risks introducing microorganisms. Two consequences follow. First, microbial growth can directly degrade the peptide, because many bacteria secrete proteases that cleave peptide bonds — a contaminated stock can lose potency far faster than chemistry alone would predict. Second, even after cells are removed or killed, bacterial cell-wall fragments (endotoxin/lipopolysaccharide) persist and can confound cell-based and in-vivo research by triggering inflammatory responses that have nothing to do with the peptide under study. This is the core rationale for bacteriostatic diluents in multi-withdrawal research stocks and for aseptic technique regardless of diluent: the benzyl alcohol in bacteriostatic water suppresses growth during the in-use window, but it does not remove pre-existing endotoxin, so starting from low-endotoxin water and clean containers matters. For work sensitive to these effects, endotoxin can be quantified by the limulus amebocyte lysate (LAL) assay, and the practical rule is to keep the in-use window short, store cold, and discard promptly on any sign of turbidity.
How does container material change tesamorelin recovery?
Container choice is a stability variable in its own right for a cationic peptide. Standard borosilicate glass presents silanol (Si-OH) groups and siloxane surfaces that carry negative charge and bind cationic peptides electrostatically; the documented result is that only 10–20% of expected peptide may be recovered from dilute solution in bare borosilicate vials.[7] High-purity polypropylene is inherently free of surface silanols and generally adsorbs less, and dedicated low-binding (“protein LoBind”-type) tubes are engineered specifically to minimize this loss.[7] The counter-consideration is extractables and leachables: only high-purity, mold-release-free polypropylene provides the low extractables required for sensitive analytical work, so “plastic” is not automatically superior — the grade matters. For quantitative pharmacology where every nanogram counts, container material should be selected deliberately and, ideally, recovery should be measured for the specific peptide, concentration, and container combination rather than assumed from general rules.
| Container | Surface chemistry | Adsorption of cationic peptide | Best-fit research use |
|---|---|---|---|
| Standard borosilicate glass | Silanol/siloxane, net negative | High (recovery often 10–20% at low conc.) | Concentrated stocks; avoid for dilute cationic peptide |
| High-purity polypropylene | No surface silanols | Lower | General handling if grade is low-extractable |
| Low-binding (LoBind-type) tubes | Engineered anti-adsorption | Lowest | Dilute working solutions, quantitative assays |
What is best-practice reconstitution and handling for tesamorelin in research?
Synthesizing the chemistry above into a workflow, the following steps reflect standard careful peptide handling adapted to tesamorelin’s specific vulnerabilities (oxidation-prone methionine, deamidation-prone amides, cationic adsorption). None of this is human dosing guidance; it is laboratory handling for research-use-only material.
- Equilibrate before opening. Let the cold, sealed vial reach room temperature before breaking the seal, so that atmospheric moisture does not condense onto the cold powder and raise residual moisture.
- Choose the diluent to match the storage plan. Bacteriostatic water for multi-day, multi-withdrawal stocks; sterile water (or a validated mildly acidic diluent) for single-use or stability-sensitive work.
- Add diluent gently down the vial wall. Direct the stream against the glass rather than onto the cake, to avoid frothing and interfacial stress that nucleate aggregation.
- Dissolve by rolling or swirling — never shake. Gentle mixing preserves the peptide; vigorous agitation and foam generation promote aggregation at the air–water interface.
- Minimize headspace and exclude light. Less headspace air means less dissolved oxygen driving methionine oxidation; dark storage curbs photo-oxidation.
- Store cold, and aliquot before freezing. Refrigerate solutions in use; for longer holds, divide into single-use aliquots and freeze once, so no aliquot endures repeated freeze–thaw.
- Use low-adsorption containers for dilute work, and consider a carrier protein where the assay permits, to protect against silent adsorptive losses.
- Inspect and discard on any physical change. Cloudiness, particulates, gel, or precipitate indicate aggregation; such solutions are both inactive and analytically misleading.
Because reconstitution changes the effective concentration and any downstream research calculation depends on it, a reconstitution-aware calculation tool such as our dosage calculator can help translate vial mass and diluent volume into concentration for record-keeping. For terminology used throughout this article — lyophilization, deamidation, Tg, IGF-1 — our peptide research glossary provides concise definitions.
How is tesamorelin stability actually measured?
Storage guidance is only credible if it can be checked, and peptide stability is assessed with a defined toolkit of analytical methods. The purpose is to distinguish intact, active molecule from its degradation products — not merely to measure total peptide mass, which can be unchanged even as activity collapses.
Reversed-phase HPLC (RP-HPLC)
RP-HPLC is the workhorse for peptide purity and stability. Because deamidation, oxidation, and truncation each change the molecule’s hydrophobicity, degradation products typically resolve as separate peaks from the parent, allowing quantification of percent intact peptide over time. A properly developed stability-indicating method is validated to separate and unambiguously identify the parent peptide from its degradants, and its specificity is demonstrated by challenging it with forced-degradation (stress) samples.[11]
Mass spectrometry
Mass spectrometry (often LC-MS) confirms molecular identity and pinpoints degradation chemistry by mass shift: a +16 Da increment flags methionine oxidation to the sulfoxide (+32 for the sulfone), while a +1 Da shift is the signature of deamidation (loss of ammonia, gain of a hydroxyl). This makes MS the definitive method for assigning which residue degraded and by which pathway, complementing HPLC’s quantification.[11]
Forced-degradation (stress) testing and orthogonal methods
Following the logic of ICH stability guidance, forced-degradation studies deliberately stress the peptide under acid, base, oxidative (e.g., hydrogen peroxide), thermal, and photolytic conditions to map its degradation pathways and prove that the analytical method can detect them.[11] Orthogonal biophysical methods round out the picture: size-exclusion chromatography and dynamic light scattering detect aggregation and particulates, while circular dichroism reports on secondary structure (loss of alpha-helical content signals unfolding). For a molecule like tesamorelin whose activity depends on an intact receptor-binding helix, structural methods are as informative as chromatographic purity.
| Method | What it detects | Degradation route it best reveals |
|---|---|---|
| RP-HPLC (stability-indicating) | Percent intact vs. degradant peaks | Deamidation, oxidation, truncation |
| LC-MS / high-res MS | Exact mass, mass shifts (+16, +1 Da) | Oxidation vs. deamidation assignment |
| SEC / DLS | Aggregates, oligomers, particulates | Aggregation |
| Circular dichroism | Secondary-structure content | Unfolding / conformational loss |
| Forced degradation (ICH-style) | Pathway mapping, method specificity | All, under deliberate stress |
What does the clinical and research evidence base tell us about tesamorelin?
Stability matters because it protects a molecule with a genuinely substantial evidence base — and that evidence base is worth stating honestly and by study type. Tesamorelin is unusual among research peptides in that it has completed large randomized human trials, because it is an approved drug.
Human randomized controlled trials
The pivotal evidence comes from two multicenter, double-blind, placebo-controlled phase 3 trials in adults with HIV-associated abdominal fat accumulation. The first, reported by Falutz and colleagues in the New England Journal of Medicine in 2007, randomized 412 patients 2:1 to tesamorelin 2 mg daily subcutaneously or placebo for 26 weeks and demonstrated a statistically significant reduction in visceral adipose tissue versus placebo.[12] A pooled analysis of both phase 3 trials with extension data (Falutz et al., Journal of Clinical Endocrinology & Metabolism, 2010) covered 816 patients treated for up to 52 weeks, reporting VAT reductions on the order of 15–18%, an IGF-1 rise reflecting on-target GH-axis activation, comparable adverse-event rates between arms, and — importantly — re-accumulation of visceral fat after discontinuation, indicating the effect requires continued dosing.[13]
Subsequent investigator-initiated randomized trials extended the picture to liver fat: Stanley and colleagues (JAMA, 2014) showed that tesamorelin over 6 months reduced both visceral and, more modestly, liver fat in HIV-infected patients with abdominal adiposity,[14] and a later randomized, double-blind trial (Stanley et al., Lancet HIV, 2019) in patients with HIV and hepatic steatosis reported a relative reduction in hepatic fat fraction of roughly one-third versus placebo over 12 months.[15] These are real, human, randomized data — a rarity in the research-peptide space — but they are specific to the HIV-lipodystrophy population and to the approved product; they should not be over-extrapolated to unstudied populations or uses.
What research models are used to study tesamorelin and its stability?
Beyond the human trials, the preclinical and analytical models used to characterize a GHRH analog like tesamorelin fall into a few categories, and understanding them clarifies what a “potency” number actually measures. At the receptor level, GHRH-R binding and activation are assessed in cell systems expressing the receptor, using cAMP-accumulation readouts as the proximal signal of agonism — this is the assay most directly degraded by oxidation or deamidation of the binding helix. Ex-vivo and cell-based systems using cultured pituitary somatotrophs measure GH release as a functional endpoint. Downstream, IGF-1 induction in hepatocyte models or in-vivo serves as a systemic pharmacodynamic marker. For visceral-fat and metabolic questions, the human HIV-lipodystrophy trials themselves are the primary evidence, supported by imaging endpoints (CT/MRI-derived visceral adipose tissue and hepatic fat fraction) rather than animal surrogates. On the stability side, the “models” are analytical rather than biological: forced-degradation studies under controlled stress, real-time and accelerated stability chambers at defined temperature and humidity, and the chromatographic/spectrometric methods described earlier. A rigorous stability program pairs a chemical readout (percent intact by HPLC) with a biological readout (retained receptor activity or IGF-1 induction), because the two can diverge — and it is the biological readout that ultimately defines whether stored material is still fit for research use.
Pharmacokinetics and honest limits
Population pharmacokinetic analysis in HIV-infected patients and healthy subjects characterizes tesamorelin as a rapidly absorbed, rapidly cleared peptide with a short plasma half-life — on the order of tens of minutes — consistent with its design as a pulsatile GHRH-receptor agonist rather than a sustained GH replacement.[16] The honest boundaries of the evidence are equally important. The efficacy database is concentrated in HIV-associated lipodystrophy; robust long-term outcome data in other populations are limited or absent. GH-axis stimulation raises IGF-1 and warrants attention to glucose metabolism and to the theoretical concerns that accompany any GH/IGF-1 elevation. And the anti-aging framing sometimes attached to GHRH analogs is largely extrapolation from mechanism rather than demonstrated long-term benefit in healthy individuals — a gap that should be stated plainly rather than papered over.
How does tesamorelin compare with related GHRH and GH-axis peptides?
Tesamorelin sits within a family of growth hormone secretagogues, and its stability considerations broadly resemble those of other GHRH analogs and growth hormone–releasing peptides (GHRPs), all of which are supplied lyophilized and share the same four degradation pathways. The differences are in sequence-specific vulnerabilities and pharmacology.
| Peptide | Class / target | Approximate MW | Approved drug? | Key stability note |
|---|---|---|---|---|
| Tesamorelin | GHRH-R agonist (44-aa GRF analog) | ~5,136 Da (free base) | Yes (HIV lipodystrophy) | Met + Asn/Gln residues; cationic adsorption |
| Sermorelin | GHRH-R agonist (GRF 1–29) | ~3,358 Da | Historically yes (now varies) | Shorter, notably labile in solution; Asp-Pro/Asn hot spots |
| CJC-1295 (with/without DAC) | GHRH-R agonist, long-acting | ~3,367 Da (no DAC) | No (research-use) | DAC variant designed for extended half-life |
| Ipamorelin | Ghrelin/GHS-R agonist (GHRP) | ~712 Da | No (research-use) | Small pentapeptide; different receptor and pathway |
The comparison underscores a general principle: molecular weight, sequence, and charge dictate both the pharmacology and the failure modes. Tesamorelin’s larger 44-residue structure gives it more potential deamidation and oxidation sites than a short GHRP, while its cationic character makes adsorption a bigger practical concern than for a neutral small peptide. Researchers comparing protocols for different vial strengths can consult the dedicated tesamorelin 10 mg vial protocol and the tesamorelin 5 mg vial protocol for concentration-specific handling references.
What are the open questions and limitations in tesamorelin stability science?
Several honest gaps remain. First, most publicly available quantitative stability figures for reconstituted tesamorelin come either from the approved-product label (which concerns a specific finished formulation and a prompt-use design) or from general peptide-class guidance; rigorous, lot-specific stability curves for research-grade material under varied storage conditions are rarely published, so any stated in-use window should be treated as a starting hypothesis to be verified analytically, not a certified specification. Second, the relative contribution of each degradation pathway under real research storage — how much of a given potency loss is oxidation versus deamidation versus adsorption — is molecule-, buffer-, and container-specific and is best resolved by RP-HPLC plus MS on the actual samples in use. Third, the interplay of preservative (benzyl alcohol) with peptide conformation over extended multi-withdrawal storage is not deeply characterized for every peptide, so multi-day bacteriostatic-water stocks trade microbial control against a less-characterized chemical background. The responsible posture is to store conservatively (cold, dark, aliquoted, low-adsorption containers), to keep the in-use window short, and to verify rather than assume.
How should shelf-life and expiry figures for tesamorelin be interpreted?
Numbers attached to peptide stability are frequently misread, so it helps to separate three distinct concepts. A manufacturer expiry on lyophilized powder is a conservative date backed (for a pharmaceutical) by real-time stability data on that specific formulation and packaging; for research-grade material it may be a generic estimate rather than a lot-specific certified figure, and it applies only while the vial remains properly sealed and stored. A reconstituted in-use window is a completely different quantity — it starts the moment diluent is added and is governed by the solution chemistry (temperature, pH, diluent, container, concentration) discussed throughout this article, not by the powder’s expiry date. And an accelerated-stability figure — derived from holding samples at elevated temperature and extrapolating via Arrhenius kinetics — is a prediction, useful for ranking formulations but not a substitute for real-time data on the exact material.
The practical upshot is that a single “X days after reconstitution” number copied from a general source should be treated as a hypothesis, not a specification. The only way to know the true in-use window for a given lot, diluent, and storage condition is to measure it: pull samples across a time course and quantify percent intact peptide by a stability-indicating HPLC method, ideally paired with a receptor-activity or IGF-1-induction check. Where such measurement is not feasible, the conservative default — cold, dark, aliquoted, low-adsorption storage with the shortest practical in-use window — errs in the right direction. This is also why two labs can honestly report different stability for “the same” peptide: their diluent, concentration, container, and temperature differ, and each of those is a stability variable.
Frequently Asked Questions
How long is reconstituted tesamorelin stable in research settings?
There is no single certified number for research-grade material, but general peptide-class guidance and the molecule’s chemistry point to days-to-a-few-weeks when refrigerated (2–8°C) and dark, versus only hours to about a day at room temperature. Much of the total degradation occurs in the first 72 hours. Any specific in-use window should be confirmed analytically (RP-HPLC) for the exact lot, diluent, concentration, and container, since these variables materially change the answer.
Should tesamorelin be reconstituted with bacteriostatic or sterile water?
It depends on the storage plan. Bacteriostatic water (0.9% benzyl alcohol) suppresses microbial growth and suits multi-day, multi-withdrawal stocks, remaining usable for a commonly cited window of up to 28 days after first entry. Sterile water contains no preservative and fits single-use vials consumed in one session. The approved Egrifta product uses supplied Sterile Water for Injection and is designed for prompt use, which is a finished-product decision rather than a universal research rule.
Why does tesamorelin degrade — which parts of the molecule are vulnerable?
Four pathways compete once it is in solution: deamidation of asparagine/glutamine side chains (accelerated at higher pH), oxidation of methionine (Met27 sits in the receptor-binding helix), aggregation promoted by agitation and air–liquid interfaces, and adsorption of the cationic peptide onto glass surfaces. Because Met27 lies in the binding region, oxidation there can abolish receptor recognition even when total peptide mass looks unchanged, which is why activity-relevant analysis matters more than mass alone.
Does freezing reconstituted tesamorelin protect it?
Freezing slows chemistry but is not free of risk. Each freeze–thaw cycle concentrates peptide and buffer into the shrinking liquid phase, creates ice interfaces, and causes transient pH shifts that promote aggregation and unfolding. The standard mitigation is to divide the reconstituted stock into single-use aliquots and freeze each once, so no portion endures repeated cycling. Aliquoting before freezing is often the single most protective handling decision across a multi-week study.
Why does container choice affect how much tesamorelin I recover?
Tesamorelin is cationic at neutral pH, and standard borosilicate glass carries negatively charged silanol groups that bind cationic peptides electrostatically. In controlled studies of cationic peptides, only 10–20% of dilute peptide was recovered from bare glass. High-purity polypropylene and dedicated low-binding tubes reduce this loss substantially. For dilute working solutions, low-adsorption containers — and sometimes a carrier protein where the assay allows — prevent silent losses that would otherwise corrupt dose–response data.
Is tesamorelin FDA-approved, and can research-grade material be used therapeutically?
Tesamorelin is FDA-approved as the pharmaceutical Egrifta for HIV-associated lipodystrophy, and a newer weekly-reconstitution formulation (Egrifta WR) was approved in March 2025. However, research-grade tesamorelin sold for laboratory use is not the approved drug: it is intended for in-vitro and non-clinical research only, is not manufactured to finished-pharmaceutical controls, and is not for human therapeutic use. The approval applies to the specific quality-controlled products, not to bulk research powder.
How is tesamorelin stability measured analytically?
Reversed-phase HPLC quantifies percent intact peptide by resolving degradation products as separate peaks, and a stability-indicating method is validated against forced-degradation samples. Mass spectrometry assigns the chemistry — a +16 Da shift indicates methionine oxidation, a +1 Da shift indicates deamidation. Size-exclusion chromatography and dynamic light scattering detect aggregation, and circular dichroism reports secondary-structure loss. Together these methods distinguish intact, active molecule from degradants, which mass measurement alone cannot do.
Does storage temperature for lyophilized tesamorelin differ from the reconstituted solution?
Yes, substantially. The lyophilized powder, sealed and desiccated, is best kept cold (commonly −20°C or colder) and dark, where low residual moisture keeps its glass transition temperature high and stability can extend for months to years. Once reconstituted, the same molecule becomes far more labile: refrigeration slows degradation but the in-use window collapses to days-to-weeks at most, and room-temperature solution degrades within hours to a day. The dry state and the solution state are effectively two different stability regimes.
References
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. Tesamorelin. National Institute of Diabetes and Digestive and Kidney Diseases; NCBI Bookshelf (NBK548730). https://www.ncbi.nlm.nih.gov/books/NBK548730/
- EGRIFTA SV (tesamorelin) for injection — Full Prescribing Information. U.S. Food and Drug Administration, accessdata (label 022505s018, 2024). https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/022505s018lbl.pdf
- FDA Approves F8 Formulation of Theratechnologies’ Tesamorelin (Egrifta WR) for HIV-Associated Lipodystrophy. Contagion Live, 2025. https://www.contagionlive.com/view/fda-approves-f8-formulation-of-theratechnologies-tesamorelin-for-hiv-associated-lipodystrophy
- Understanding Lyophilization: How Freeze-Drying Preserves Peptides. Alpha Peptides technical resource. https://alpha-peptides.com/lyophilization-freeze-drying-peptides/
- Lyophilization in Peptide Research: Freeze-Drying Science, Excipient Selection, and Stability Data. Maple Research Labs. https://mapleresearchlabs.com/peptide-research/lyophilization-peptide-research-freeze-drying-excipients-stability-data/
- The Peptide Science Handbook, Chapter 4: Stability, Solubility, and Degradation Pathways. PolyBiotech. https://www.polybiotech.co/blogs/the-peptide-handbook/the-peptide-science-handbook-chapter-4-stability-solubility-and-degradation-pathways
- Kristensen K, et al. Adsorption of Cationic Peptides to Solid Surfaces of Glass and Plastic. PLOS ONE. 2015;10(5):e0122419. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0122419
- Lyophilized Peptide Storage: Temperature, Humidity & Light. Verified Peptides Knowledge Hub. https://verifiedpeptides.com/knowledge-hub/lyophilized-peptide-storage-temperature-humidity-light/
- Peptide Stability Guide: Storage & Degradation. American Peptides. https://www.americanpeptides.us/blogs/news/peptide-stability-storage-degradation
- Bacteriostatic Water (0.9% Benzyl Alcohol) — Product Information. Canvax Biotech. https://www.canvaxbiotech.com/product/buffers-solutions/water-solutions/bacteriostatic-water-0-9-benzyl-alcohol/
- Development of a novel stability-indicating RP-HPLC method for quantification of a mimetic peptide and its degradation kinetics. PMC5790747. https://pmc.ncbi.nlm.nih.gov/articles/PMC5790747/
- Falutz J, Allas S, Blot K, et al. Metabolic Effects of a Growth Hormone–Releasing Factor in Patients with HIV. N Engl J Med. 2007;357(23):2359–2370 (PMID 18057338). https://pubmed.ncbi.nlm.nih.gov/18057338/
- Falutz J, Mamputu JC, Potvin D, et al. Effects of Tesamorelin (TH9507) in HIV-Infected Patients with Excess Abdominal Fat: A Pooled Analysis of Two Phase 3 Trials with Safety Extension Data. J Clin Endocrinol Metab. 2010;95(9):4291–4304 (PMID 20554713). https://pubmed.ncbi.nlm.nih.gov/20554713/
- Stanley TL, Feldpausch MN, Oh J, et al. Effect of Tesamorelin on Visceral Fat and Liver Fat in HIV-Infected Patients with Abdominal Fat Accumulation: A Randomized Clinical Trial. JAMA. 2014;312(4):380–389 (PMID 25038357). https://pubmed.ncbi.nlm.nih.gov/25038357/
- Stanley TL, Fourman LT, Feldpausch MN, et al. Effects of Tesamorelin on Non-Alcoholic Fatty Liver Disease in HIV: A Randomized, Double-Blind, Multicenter Trial. Lancet HIV. 2019. PMC6981288. https://pmc.ncbi.nlm.nih.gov/articles/PMC6981288/
- Population Pharmacokinetic Analysis of Tesamorelin in HIV-Infected Patients and Healthy Subjects. PubMed (PMID 25358450). https://pubmed.ncbi.nlm.nih.gov/25358450/