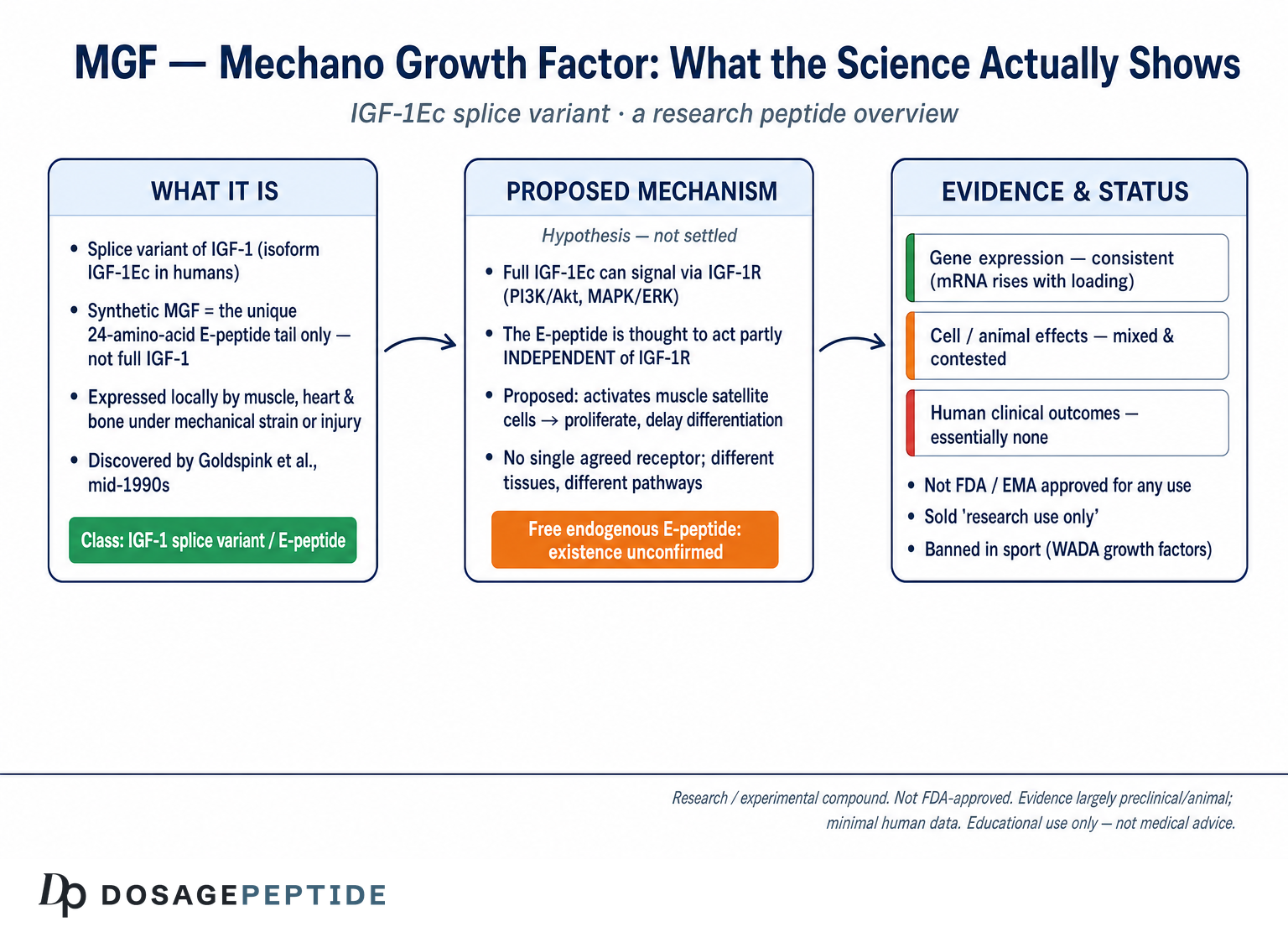
Mechano Growth Factor, almost always abbreviated to MGF, is not a wholly separate hormone in the way that name might suggest. It is a splice variant of insulin-like growth factor 1 (IGF-1) — specifically the isoform researchers label IGF-1Ec in humans — that skeletal muscle, heart, bone and several other tissues transcribe in response to mechanical strain or physical damage. The compound entered the scientific vocabulary through the work of Geoffrey Goldspink and colleagues in the mid-1990s, who noticed that stretched or overloaded muscle rapidly switched on a version of the IGF-1 gene carrying an unusual carboxy-terminal “E-peptide” not found in the liver-derived circulating form.1 Because the trigger was mechanical loading, they coined the name mechano growth factor.2
In the research-peptide marketplace, MGF is sold as a synthetic version of that unique 24–25 amino-acid E-peptide tail, and a longer-lasting chemically modified relative, PEG-MGF, is sold alongside it. Marketing copy frequently frames these as potent muscle-building or injury-repair agents. The honest scientific picture is considerably more restrained. MGF sits at the center of an unusually contested corner of muscle biology: some laboratory studies report that the synthetic E-peptide activates muscle stem cells and protects heart and nerve tissue, while other well-designed studies find essentially no effect, and a fundamental question — whether the E-peptide even exists as a free, biologically active molecule inside the body — remains formally unresolved.4
This article walks through what MGF actually is at the molecular level, what the primary literature does and does not support, how it compares with related compounds such as native IGF-1 and IGF-1 LR3, the animal and cell models used to study it, what can be said about safety, and its regulatory standing. Throughout, the aim is education grounded in primary sources rather than promotion. MGF is not an approved medicine anywhere, the great majority of evidence is preclinical, and human data are minimal. Readers should treat every claim below as a description of research findings, not as guidance for use.
What MGF Is and Where It Came From
The IGF-1 gene does not produce a single product. Through alternative splicing — the process by which a cell stitches together different combinations of the gene’s exons — it generates several messenger RNA transcripts that share the mature IGF-1 core but differ in their C-terminal “extension” or E-peptide. In humans the principal circulating isoform is IGF-1Ea, produced largely by the liver under growth-hormone control. A second variant, IGF-1Eb, and a third, IGF-1Ec, arise when the splicing machinery includes or shifts reading through exon 5. IGF-1Ec is the transcript that became known as mechano growth factor.3
The discovery story is worth understanding because it explains the compound’s name and its intended biology. In 1996, Yang, Alnaqeeb, Simpson and Goldspink cloned an IGF-1 isoform that appeared in rabbit skeletal muscle after the muscle was subjected to stretch, and they characterized it as an autocrine or paracrine factor — one that acts locally on the cells that make it rather than circulating through the bloodstream like liver IGF-1.1 A follow-up study in 1999 by McKoy and colleagues confirmed that stretch combined with electrical stimulation drove expression of this distinct splice variant, IGF-1Ec/MGF, in a pattern quite different from the liver-type IGF-1Ea.2 The underlying idea was elegant: muscle experiencing mechanical load would locally manufacture a growth signal to drive its own adaptation and repair.
What makes MGF structurally distinctive is the reading-frame shift introduced by the exon-5 splice. In most species the resulting E-peptide is 25 amino acids long; in humans it is 24 amino acids, and the sequence is highly conserved across mammals, which researchers often read as a sign of functional importance.3 This E-domain is what synthetic “MGF” products contain — not the full IGF-1 molecule, but this short peptide tail. That distinction matters enormously for interpreting the biology, because the mature IGF-1 region and the E-peptide region are thought to do different things.
Expression of MGF is not confined to skeletal muscle. The growth-plate study by the group that mapped IGF-1 isoforms found that MGF represented roughly a third of all IGF-1 isoform expression within the cartilage growth plate, concentrated in the resting and hypertrophic zones.3 Other work has documented MGF induction in cardiac muscle after infarction and in brain tissue after ischemic injury, always with the same signature: a rapid, transient rise in the mechano/damage-responsive splice variant, often preceding the slower rise of the systemic IGF-1Ea form.4 This pattern — early, local, stress-triggered — is the core of the biological hypothesis around MGF: that it is an emergency, first-responder signal produced by tissue under strain.
Two cautions belong here from the outset. First, most of what is known about MGF concerns its behavior as an mRNA transcript and as a synthetic peptide added to cells or injected into animals. Whether the body actually cleaves the full IGF-1Ec protein to liberate a free, circulating E-peptide has never been firmly demonstrated.4 Second, the name “growth factor” invites the assumption that MGF straightforwardly grows muscle in the way anabolic marketing implies. The literature is far more equivocal than that, as later sections detail.
Molecular Mechanism: How an IGF-1 Splice Variant Becomes MGF
To understand MGF’s proposed mechanism, it helps to separate the full IGF-1Ec protein from the E-peptide fragment that research peptides are meant to reproduce. The full-length IGF-1Ec pro-hormone contains the mature IGF-1 sequence plus the MGF E-domain. In principle, that pro-hormone could signal through the classical IGF-1 receptor (IGF-1R) via its mature region and, separately, exert distinct effects through its E-domain. The synthetic MGF sold as a peptide corresponds to the E-domain alone.3
The mature IGF-1 portion, when present, binds IGF-1R, a receptor tyrosine kinase, and triggers the two canonical downstream cascades familiar from IGF-1 biology: the PI3K/Akt pathway, associated with protein synthesis and cell survival, and the MAPK/ERK pathway, associated with proliferation and differentiation. This is the same machinery that engineered IGF-1 analogs such as IGF-1 LR3 exploit, and it is well characterized.3 The MGF E-peptide, however, is proposed to act at least partly independently of IGF-1R. The growth-plate study noted that the E-peptide does not bind IGF binding proteins and lacks the IGF-1R binding epitopes, which is one reason researchers suspect it works through a different, still poorly defined route.3
What might that route be? Cell-culture studies have implicated several signaling elements. Work in cardiomyocyte-like cells suggested the MGF-24aa E-peptide stimulates the MAPK/ERK pathway, while neuroprotection experiments pointed toward protein kinase C (PKC) activity and downstream activation of the antioxidant transcription factor Nrf2.4 In tenocytes (tendon cells), synthetic MGF E-peptide was reported to drive migration through a FAK–ERK1/2 signaling axis that increased nuclear stiffness.11 A separate line of research described a putative MGF receptor that localizes to the nucleus of osteoblasts under mechanical stimulation, hinting at an intracrine or nuclear mode of action rather than classical surface-receptor signaling.12 The candor here is important: there is no single, agreed-upon MGF receptor, and different tissues appear to engage different pathways.
The proposed muscle mechanism is the one most cited in the peptide world. The hypothesis holds that the MGF E-peptide preferentially activates quiescent satellite cells — the resident stem cells of skeletal muscle — pushing them to enter the cell cycle and proliferate as myoblasts while delaying their differentiation and fusion. This bias toward proliferation over differentiation, if real, would be biologically sensible: after damage, muscle first needs to expand its stem-cell pool before those cells mature and fuse into new muscle fibers, a job the mature IGF-1 domain is thought to handle later.5 In this model, MGF and mature IGF-1 are sequential, complementary signals: MGF for early expansion, IGF-1 for later maturation.
It is essential to flag that this is a hypothesis supported by some experiments and contradicted by others. The most direct counter-evidence comes from work showing that synthetic MGF peptide, at concentrations up to 500 ng/mL, failed to increase proliferation of mouse C2C12 cells or primary human myoblasts and failed to inhibit their differentiation, even though the same cells responded robustly to IGF-1.6 The proposed mechanism, in other words, is plausible and partly supported at the level of individual studies, but it is not a settled fact, and the reproducibility problem sits at the heart of the field.
One more mechanistic subtlety recurs throughout the literature: the endogenous E-peptide, if it is produced at all, appears to have a very short half-life, and IGF-1 aggregation at physiological pH may mask its detection in tissue. Synthetic versions require chemical stabilization to persist. This is why the entire question of whether MGF functions as a discrete secreted molecule in vivo remains open, and why so much of the evidence rests on adding stabilized synthetic peptide to isolated cells.4
It is also worth distinguishing two competing mechanistic pictures that appear in the literature, because they carry very different implications. In the first, the E-peptide is a genuine secreted signaling molecule that acts on neighboring cells through a surface receptor — a paracrine model that would make injected synthetic MGF at least conceptually coherent as an exogenous drug. In the second, the E-domain functions primarily within the cell that expresses the full IGF-1Ec pro-hormone, influencing processing, trafficking, or nuclear events without ever existing as a free extracellular peptide — an intracrine model under which injecting a synthetic fragment might not reproduce the natural biology at all. The osteoblast work describing nuclear localization of an MGF-associated receptor leans toward the second picture, while the cardiac and neural studies that add synthetic peptide externally implicitly assume the first.4,12 The field has not reconciled these views, and a reader should notice that a compound’s entire rationale as an injectable depends on which one is correct.
What the Research Actually Shows — Honestly Graded
The evidence base for MGF is best described as a patchwork of preclinical signals, some encouraging, some null, with almost no rigorous human efficacy data. Grading it honestly means distinguishing three things: mRNA-expression studies (strong and consistent), synthetic-peptide effect studies in cells and animals (mixed and contested), and human clinical outcomes (essentially absent).
On the expression side, the evidence is solid. Multiple independent groups have shown that mechanical loading, resistance exercise, stretch, or tissue injury transiently upregulate the IGF-1Ec/MGF transcript. Hameed and colleagues demonstrated that a single bout of high-resistance exercise increased IGF-I splice variant expression in human skeletal muscle, with a notably blunted MGF response in older versus younger men — an age effect that recurs across the MGF literature.10 That MGF is a genuine, mechanically responsive splice variant is not in serious dispute.
On the synthetic-peptide side, the picture fractures. Positive reports include the satellite-cell work of Kandalla and colleagues, who found that the MGF E-peptide increased the proliferative lifespan and delayed senescence of muscle progenitor cells isolated from neonatal and young-adult muscle — but notably not from old-adult muscle, again pointing to age-dependent responsiveness.5 In the heart, Carpenter and colleagues reported that MGF E-peptide reduced loss of cardiac function after acute myocardial infarction in rats, plausibly by protecting cardiomyocytes in the peri-infarct zone from apoptosis.16 Stavropoulou and colleagues mapped IGF-1 transcript expression in infarcted rat myocardium and characterized MGF E-peptide actions in cardiac cells in vitro.9 In the nervous system, Riddoch-Contreras and colleagues found that MGF treatment improved hindlimb muscle strength and increased motoneuron survival in the SOD1(G93A) mouse model of amyotrophic lateral sclerosis,7 and a later study reported that MGF overexpression significantly increased proliferative-cell density in neurogenic regions of the aging mouse brain, partially offsetting the age-related decline in progenitor proliferation.8
Against this stands a directly contradictory and methodologically careful study. Fornaro and colleagues tested both native and chemically stabilized MGF peptide on C2C12 myoblasts, primary human skeletal muscle myoblasts, and primary mouse muscle stem cells. Across concentrations up to 500 ng/mL, the peptide produced no measurable increase in proliferation and no inhibition of differentiation, while IGF-1 in the same experiments worked as expected. The authors concluded that their data called into question whether the E-peptide has a physiological role as a distinct signaling molecule at all.6 This is not a fringe result; it appears in a mainstream physiology journal and directly targets the central muscle claim.
| Research domain | Representative finding | Model | Evidence level |
|---|---|---|---|
| Gene expression | Loading/exercise transiently raises IGF-1Ec/MGF mRNA2,10 | Human & rabbit muscle | Consistent (mRNA only) |
| Muscle stem cells | E-peptide extends proliferative lifespan in young donors5 | Human progenitor cells | Positive, single-lab |
| Muscle stem cells | No effect on proliferation or differentiation6 | C2C12, primary cells | Negative, well-controlled |
| Cardiac | Reduced functional loss after infarction16 | Rat MI model | Preclinical, animal |
| Neural | Motoneuron rescue; enhanced neurogenesis7,8 | Mouse models | Preclinical, animal |
| Human clinical outcomes | — | — | Essentially none |
The bottom line is that MGF has intriguing but internally conflicting preclinical evidence and no controlled human efficacy trials establishing that injected MGF or PEG-MGF builds muscle, heals injuries, or improves any clinical outcome in people. Marketing that presents MGF as a proven anabolic or regenerative agent runs well ahead of the science. Readers wanting a broader view of how peptide evidence is weighed can consult general references such as the site’s peptide dosage library for how comparable compounds are documented.
MGF, PEG-MGF, IGF-1 and Related Compounds Compared
MGF is frequently discussed alongside a cluster of IGF-1–related molecules, and confusion between them is common. Clarifying the relationships is one of the most useful things a reader can take away, because the compounds differ sharply in what they are, how long they last, and how much evidence supports them.
Native IGF-1 (IGF-1Ea) is the mature growth factor produced mainly by the liver under growth-hormone control. It binds IGF-1R with high affinity, circulates bound to IGF binding proteins, and has a well-established endocrine role in growth and metabolism. Its circulating half-life is short on its own but is extended in the body by binding proteins.
MGF (IGF-1Ec E-peptide) is the 24-amino-acid C-terminal tail of the mechano-responsive splice variant. As a synthetic peptide it does not carry the mature IGF-1 domain, so it is not simply “IGF-1 with a longer name.” Its proposed actions are receptor-uncertain and its unmodified form is thought to survive only minutes in circulation.4
PEG-MGF is MGF chemically conjugated to polyethylene glycol (PEGylation). The PEG shell shields the peptide from enzymatic degradation, extending its functional presence from minutes to a reported window of days. Vendor and secondary sources describe a half-life on the order of days, versus minutes for unmodified MGF, which is the entire rationale for the modification. It is important to note that this pharmacokinetic claim rests largely on the general pharmacology of PEGylation and vendor literature rather than published human data specific to PEG-MGF.13
IGF-1 LR3 is a different animal entirely: a modified full-length IGF-1 analog with an N-terminal 13-amino-acid extension and an Arg-for-Glu substitution at position 3, which dramatically reduces its binding to IGF binding proteins and extends its half-life to roughly 20–30 hours. Unlike the MGF E-peptide, LR3 signals through IGF-1R directly and potently. Readers comparing these should not conflate MGF with LR3; the site’s IGF-1 LR3 protocol page lays out how that analog differs in structure and handling.
| Compound | What it is | Primary target | Reported persistence | Approval status |
|---|---|---|---|---|
| IGF-1 (Ea) | Native mature growth factor | IGF-1R | Short; extended by binding proteins | Approved form (mecasermin) for specific indications |
| MGF (E-peptide) | IGF-1Ec C-terminal fragment | Uncertain / non-IGF-1R | Minutes (unmodified) | None |
| PEG-MGF | PEGylated MGF E-peptide | Uncertain / non-IGF-1R | Days (reported) | None |
| IGF-1 LR3 | Modified long-acting IGF-1 analog | IGF-1R | ~20–30 hours | None (research reagent) |
Beyond the IGF family, MGF is often marketed within the broader “recovery” and “repair” peptide category alongside compounds such as BPC-157 and TB-500, which act through entirely different, non-IGF mechanisms. Those comparisons are largely commercial rather than mechanistic; a compound-by-compound reading, such as the discussion of the BPC-157 and TB-500 recovery pairing or the individual TB-500 profile, makes clear that grouping them together says more about marketing categories than shared biology. The key point for MGF specifically is that its closest true relatives are the other IGF-1 splice variants and analogs, not the general pool of “healing peptides.”
Research Models and Methodology
Because MGF has never progressed to controlled human efficacy trials, essentially all of its evidence comes from a defined toolkit of laboratory models. Understanding those models — and their limits — is central to reading the literature critically rather than taking headline conclusions at face value.
The most common models fall into a few categories. Immortalized cell lines such as mouse C2C12 myoblasts and rat H9C2 cardiac cells are cheap, reproducible, and easy to manipulate, and they underpin much of the mechanistic work on ERK, PKC and proliferation. Their weakness is that immortalized lines behave differently from primary tissue and can over- or under-report responses. Primary cells — human muscle progenitor cells, primary myoblasts, and freshly isolated satellite cells — are more physiologically faithful, and it is telling that the sharpest disagreement in the field (Kandalla’s positive satellite-cell findings versus Fornaro’s null results) plays out precisely in these primary systems.5,6
Animal models supply the in-vivo evidence. The rabbit stretch-and-stimulation model established the original expression biology.1,2 Rodent injury models — myocardial infarction in rats, the SOD1(G93A) transgenic mouse for motoneuron disease, ischemia models in brain, and muscle crush or freeze injury — supply most of the functional claims.7,8,9,16 A muscle-injury study using MGF overexpression, for example, reported modulation of inflammatory cytokine expression and altered macrophage resolution during repair, illustrating that MGF’s effects in vivo may be as much immunomodulatory as directly anabolic.14 These models are informative but come with the usual translational caveats: rodent physiology differs from human, overexpression via viral vectors is not the same as injecting a peptide, and effect sizes in inbred disease models often shrink or vanish in humans.
Methodologically, several recurring issues make the MGF literature hard to synthesize. First, peptide identity and stability vary between studies: some use the native short E-peptide, others a chemically stabilized version, and the results can diverge accordingly — a point Fornaro’s group specifically probed by testing both.6 Second, concentrations differ widely, and supraphysiologic doses in a dish may reveal effects irrelevant to any plausible in-vivo exposure. Third, the detection problem looms over the entire field: because the endogenous E-peptide is short-lived and may aggregate or be masked, distinguishing genuine biology from artifact is genuinely difficult.4 Fourth, age of the tissue is a major modifier: multiple studies find responses in young or neonatal tissue that are absent in old tissue, so a study’s choice of donor age can determine whether it reports a positive or null result.5,10
For anyone evaluating MGF, the practical methodological lesson is to ask, for each cited study, exactly what was administered, to what model, at what dose, and whether the outcome was a molecular marker or a functional result. A change in ERK phosphorylation in an immortalized cell line is a very different order of evidence from an improvement in survival in a live animal, and neither is the same as a clinical benefit in a person. The MGF literature contains all three types of claim, often cited interchangeably in promotional material, and separating them is the single most useful analytical habit a reader can adopt.
Safety and Tolerability: What Is and Isn’t Known
Any honest safety discussion of MGF must begin with the same admission that frames the efficacy discussion: there are no controlled human safety trials of synthetic MGF or PEG-MGF. What can be said about safety is therefore largely inferential, drawn from the biology of the IGF-1 axis, from animal studies not designed primarily as toxicology, and from the general risks of unregulated injectable research peptides. There is no established safe dose, no characterized human adverse-event profile, and no regulatory safety review because the compound has never been submitted for one.4
The most substantive theoretical concern derives from MGF’s membership in the IGF-1 family. IGF-1 signaling promotes cell proliferation and survival, and chronically elevated IGF-1 activity is associated in epidemiological literature with proliferative and neoplastic risk. Because MGF is designed to stimulate proliferation of progenitor and stem cells, and because its precise receptor targets are incompletely mapped, its long-term effects on cell growth in humans are simply unknown. This is not a claim that MGF causes cancer; it is a statement that a proliferation-promoting agent with an uncharacterized mechanism and no long-term human data warrants serious caution, and that the burden of proof for safety has not been met.
A second category of concern is generic to injectable research peptides regardless of the specific molecule. These products are not manufactured to pharmaceutical standards, are frequently mislabeled, and may contain impurities, incorrect peptide content, endotoxin, or bacterial contamination introduced during production or reconstitution. Injection carries risks of local reactions, infection, and immune responses to a foreign peptide. PEGylation, used to make PEG-MGF long-acting, introduces its own considerations: while PEG is widely used in approved drugs, questions about anti-PEG antibodies and tissue accumulation with repeated exposure exist in the pharmacology literature and have not been addressed for PEG-MGF specifically.13
A third point concerns interactions and physiologic context. MGF sits within a hormonal axis that influences blood glucose, growth signaling, and, potentially, cardiac and vascular tissue. The cardiac studies that report protective effects also underscore that MGF is biologically active in the heart, which cuts both ways: an agent potent enough to alter cardiomyocyte survival is an agent whose off-target cardiac effects deserve scrutiny, not reassurance.9,16 None of these interactions has been mapped in humans receiving synthetic MGF.
Dosing and exposure control add another layer of concern that is specific to how these peptides reach the market. Approved biologic drugs come with a defined therapeutic window, a characterized dose-response relationship, and pharmacokinetic data describing absorption, distribution, and clearance. MGF has none of these established for human use. PEG-MGF’s long duration of action, marketed as an advantage, is also a liability from a safety standpoint: a long-acting agent cannot be rapidly withdrawn if an adverse reaction develops, so any problem persists for the length of the peptide’s activity. Combined with batch-to-batch variability in research-grade material, this means two people using nominally identical products could receive meaningfully different actual exposures, with no way to know which.
It is also worth being explicit about what the animal literature does and does not tell us about safety. Studies such as the SOD1 motoneuron work and the neurogenesis work were efficacy studies in disease models; they were not toxicology studies, did not systematically dose-range for harm, and cannot substitute for a formal safety evaluation.7,8 Reading a favorable efficacy outcome in a mouse as evidence of human safety is a category error that peptide marketing frequently commits.
The responsible summary is that MGF’s human safety is uncharacterized, that its mechanism gives specific theoretical reason for caution around proliferation, and that the practical risks of unregulated injectable peptides compound the uncertainty. This article does not provide dosing guidance for MGF because none can be given responsibly in the absence of clinical data. Individuals considering any peptide compound should consult a qualified medical professional rather than relying on vendor protocols or anecdote.
Handling and Reconstitution in a Research Context
In legitimate laboratory settings, MGF and PEG-MGF are handled as lyophilized (freeze-dried) peptides that must be reconstituted before use. This section describes standard research-grade peptide handling practices in general terms, strictly for educational and laboratory-safety context. It is not a use protocol and does not imply that MGF is appropriate for administration to humans or animals outside of approved research.
Lyophilized peptides are typically shipped and stored dry, and dry powder is far more stable than solution. General practice is to store the unopened vial cold — refrigerated at 2–8 °C for short periods and frozen (often at −20 °C or lower) for longer-term storage — and to allow the vial to reach room temperature before opening to avoid condensation. Reconstitution is normally performed with bacteriostatic water (water containing a small amount of benzyl alcohol as a preservative) or sterile water, added slowly down the inside wall of the vial rather than injected directly onto the peptide pellet, which can shear or denature fragile peptides. The vial is then swirled gently, not shaken, until the powder dissolves.
Once in solution, peptides are markedly less stable and are generally kept refrigerated and used within a limited window, with repeated freeze-thaw cycles avoided because they degrade peptide integrity. The short intrinsic half-life of unmodified MGF is one reason PEGylated versions exist; even so, the reconstituted solution’s shelf life is finite and depends on temperature, preservative, and handling. Researchers calculating concentrations must account for the peptide mass stated on the certificate of analysis rather than assuming the labeled amount, since actual peptide content in research-grade material can vary.
Concentration and volume mathematics is where handling errors most often occur. The general relationship is straightforward — the concentration of the reconstituted solution equals the peptide mass divided by the diluent volume — but small arithmetic mistakes translate into large dosing errors, which is precisely why reconstitution is treated as a careful, deliberate step in any research protocol. General-purpose tools such as a peptide reconstitution calculator exist to reduce this class of error, and the broader dosage reference library illustrates how reconstitution volumes are documented for comparable compounds. These references are provided for methodological literacy, not as endorsement of MGF administration.
Two honesty points close this section. First, the existence of detailed handling conventions should not be mistaken for evidence of safety or efficacy; one can describe how to dissolve a compound cleanly while the compound’s clinical value remains entirely unproven. Second, sterile technique and accurate math cannot compensate for the fundamental problems already discussed — unverified purity, unknown human safety, and absent efficacy data. Clean handling of an unproven, unapproved peptide is still handling of an unproven, unapproved peptide.
Limitations and the Human-Evidence Gap
The single most important thing to understand about MGF is the size of the gap between its laboratory reputation and its human evidence base. That gap is not a minor caveat; it is the central fact. Decades after MGF was first described, there are no adequately powered, controlled clinical trials demonstrating that administering synthetic MGF or PEG-MGF produces any beneficial outcome in humans — not muscle growth, not injury repair, not cardiac protection, not neurological benefit. Every strong efficacy claim in circulation traces back to cell-culture or animal work, and even that work is internally contradictory.4,6
Several specific limitations compound the problem. The first is the unresolved existence of the free endogenous E-peptide. The review by Zabłocka and colleagues — authored in part by members of the group that discovered MGF — states plainly that while the full-length IGF-1Ec isoform has been identified, the existence of endogenously functioning E-peptides has not been confirmed, even though synthetic E-domain peptides can be active in assays.4 If the body does not actually liberate a free MGF E-peptide, then injecting a synthetic one is administering a molecule that may have no natural physiological counterpart, which reframes the entire compound as an experimental synthetic agent rather than a “bioidentical” hormone.
The second limitation is reproducibility. When a careful, well-controlled study using primary human and mouse cells finds no proliferative or anti-differentiation effect of MGF at concentrations up to 500 ng/mL — while the positive studies come disproportionately from a smaller number of laboratories — the appropriate scientific response is caution, not confidence.6 Contested preclinical findings that have not been independently replicated across multiple labs are a weak foundation for any efficacy claim.
The third limitation is the translational chasm between the models used and human application. Overexpressing MGF via a viral vector in a mouse brain, or adding stabilized peptide to a dish of young satellite cells, tells us something about MGF biology under those specific conditions. It tells us very little about what happens when an adult human injects a synthetic peptide of uncertain purity, at an unvalidated dose, expecting a systemic anabolic effect. The age-dependence of MGF responsiveness sharpens this point: several studies show effects in young or neonatal tissue that are absent in old tissue, which means even a genuine effect in a young mouse may not generalize to an older human.5,10
The fourth limitation is publication and commercial bias. MGF exists in an ecosystem where vendors have a financial interest in favorable framing, secondary sources recycle optimistic claims, and the underlying primary literature is small and mixed. It is easy to find a dozen confident articles asserting MGF’s muscle-building power; it is harder, and more important, to notice that they rarely cite the null results or the receptor uncertainty. The candor applied to other under-evidenced “bioregulator” peptides on this site — where the honest verdict is often that rigorous independent evidence is scarce — applies with equal force to MGF.
Taken together, these limitations do not prove MGF is inert or useless. They establish something more modest and more important: that MGF is an interesting research molecule with unresolved fundamental questions and no demonstrated human benefit, and that treating it as a validated therapeutic or performance agent is not supported by the evidence.
A useful way to hold all of this in mind is to picture the evidence as a pyramid. At the broad, well-supported base sits the expression biology: MGF is unquestionably a real, mechanically responsive IGF-1 splice variant. In the narrower middle sit the contested cell and animal studies, where some laboratories report effects and others do not. At the apex, where clinical proof of human benefit would live, there is nothing at all — no controlled trials, no established outcomes, no approved indication. Nearly all promotional claims about MGF quietly borrow the certainty of the base and project it onto the empty apex. Recognizing that sleight of hand is the most important interpretive skill for anyone reading about this compound.
Regulatory Status
MGF’s regulatory status is unambiguous in the ways that matter, even though the compound occupies a gray zone in the marketplace. It is not an approved drug. The United States Food and Drug Administration has not approved MGF or PEG-MGF for any human use, and no equivalent approval exists in the European Union or other major jurisdictions. Neither compound has completed the clinical trials that would be prerequisite to approval, and neither is available as a licensed medicine.13
Where MGF is sold, it is marketed as a “research chemical” or “for research use only” peptide — a designation that signals it is intended for laboratory investigation and is explicitly not for human consumption. This labeling does not confer any safety or quality assurance; it is, in practice, the legal framing under which unapproved compounds are distributed. Products sold this way are outside the manufacturing, purity, and labeling controls that govern approved pharmaceuticals, which is a core reason the safety concerns discussed earlier are so hard to quantify.
In the context of sport, the position is stricter and clearer. The World Anti-Doping Agency (WADA) prohibits growth factors that affect muscle, tendon or ligament protein synthesis, and mechano growth factors are named within the growth-factors category of the Prohibited List. MGF and its derivatives, including PEG-MGF, fall under this prohibition, which applies at all times (both in and out of competition) for athletes subject to anti-doping rules.15 An athlete using MGF is therefore committing an anti-doping rule violation regardless of any perceived benefit, and the same reasoning that placed it on the list — its purported anabolic and repair-promoting activity — is exactly the activity that remains clinically unproven.
It is worth drawing out an irony that the discoverers themselves noted. The review by Zabłocka and colleagues observed that mainstream pharmaceutical developers have largely declined to pursue MGF-type peptides — citing manufacturing cost, short half-life, and patent difficulty — leaving the space to be filled by unregulated and doping markets, where the compounds are used without adequate evidence and with attendant safety risks from uncontrolled analogs.4 That dynamic explains much about MGF’s current status: a compound with genuine scientific interest that never crossed the threshold into legitimate clinical development, yet circulates widely in a research-chemical and performance-enhancement gray market.
For readers, the regulatory takeaway is simple. MGF is not a medicine, has no approved indication, is sold only under research-use framing without pharmaceutical quality controls, and is banned in sport. Any decision involving it should be made with a qualified clinician and with full awareness that its human safety and efficacy have not been established. Broader context on how comparable unapproved peptides are catalogued can be found across the site’s reference library, which consistently flags the research-only, non-approved status of these compounds.
Frequently Asked Questions
Is MGF the same thing as IGF-1?
No, though they are closely related. MGF is a splice variant of the IGF-1 gene — specifically the IGF-1Ec isoform in humans — and synthetic “MGF” peptides reproduce only the unique 24-amino-acid C-terminal E-peptide tail of that variant, not the mature IGF-1 molecule.1,3 Native IGF-1 signals strongly through the IGF-1 receptor; the MGF E-peptide is thought to act at least partly through different, still poorly defined pathways. Calling MGF “a form of IGF-1” is loosely true at the gene level but misleading if it implies the two molecules do the same thing.
Does MGF actually build muscle?
The honest answer is that this is not established in humans. The muscle hypothesis — that MGF activates satellite cells to proliferate before differentiating — has support from some cell studies but is directly contradicted by a well-controlled study in which synthetic MGF had no effect on myoblast proliferation or differentiation while IGF-1 worked normally.5,6 There are no controlled human trials showing that injected MGF or PEG-MGF increases muscle mass or strength. Claims that MGF is a proven muscle-builder go beyond the evidence.
What is the difference between MGF and PEG-MGF?
PEG-MGF is the same MGF E-peptide with a polyethylene glycol chain attached (PEGylation). Unmodified MGF is thought to survive only minutes in circulation, whereas PEGylation shields the peptide from degradation and reportedly extends its functional presence to a matter of days.13 The proposed biological actions are the same; the difference is durability. Note that the long-half-life figure comes largely from the general pharmacology of PEGylation and vendor sources rather than published human data on PEG-MGF specifically.
Does the body naturally produce free MGF peptide?
This is genuinely unresolved and is one of the most important caveats in the field. The full-length IGF-1Ec protein is real and detectable, and its mRNA rises with mechanical loading. But whether the body actually cleaves that protein to release a free, circulating, biologically active E-peptide has never been confirmed, even though synthetic E-peptides are active in some assays.4 If no free endogenous E-peptide exists, then injected synthetic MGF may have no natural physiological counterpart.
Is MGF approved or legal to use?
MGF is not approved by the FDA, EMA, or any comparable regulator for any human use. It is sold only as a “research use only” chemical, a designation that carries no safety or quality assurance and explicitly excludes human consumption.13 In sport, mechano growth factors including MGF and PEG-MGF are on the WADA Prohibited List under growth factors and are banned at all times for athletes subject to anti-doping rules.15
Is MGF safe?
Its human safety is uncharacterized because no controlled human safety trials exist. There are specific theoretical concerns because MGF promotes cell proliferation and belongs to the IGF-1 family, whose sustained activity is associated in epidemiological literature with proliferative risk, and its receptor targets are incompletely mapped.4 On top of that, unregulated injectable peptides carry generic risks of impurity, contamination, mislabeling, and injection-related harm. No responsible safe dose can be stated, and anyone considering it should consult a qualified physician.
How does MGF compare to IGF-1 LR3?
They are quite different. IGF-1 LR3 is a modified full-length IGF-1 analog engineered to resist binding proteins and act potently through the IGF-1 receptor for roughly 20–30 hours, whereas MGF is a short E-peptide fragment with an uncertain receptor and a very short native half-life. The two should not be conflated. The site’s IGF-1 LR3 reference details how that analog differs structurally; both, however, remain unapproved research compounds.
Why is the evidence for MGF so contradictory?
Several reasons converge: studies use different peptide versions (native versus chemically stabilized) and different concentrations; responses appear to depend heavily on the age of the tissue tested, with young tissue responding and old tissue often not; the endogenous peptide is short-lived and hard to detect, making artifact difficult to exclude; and positive findings come disproportionately from a small number of laboratories while the most careful negative study used well-controlled primary cells.4,5,6,10 The result is a small, mixed literature that does not support confident conclusions.
References
- Yang S, Alnaqeeb M, Simpson H, Goldspink G. Cloning and characterization of an IGF-1 isoform expressed in skeletal muscle subjected to stretch. Journal of Muscle Research and Cell Motility. 1996;17(4):487–495.
- McKoy G, Ashley W, Mander J, Yang SY, Williams N, Russell B, Goldspink G. Expression of insulin growth factor-1 splice variants and structural genes in rabbit skeletal muscle induced by stretch and stimulation. The Journal of Physiology. 1999;516(Pt 2):583–592. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC2269271/
- Insulin-Like Growth Factor I (IGF-1) Ec/Mechano Growth Factor – A Splice Variant of IGF-1 within the Growth Plate. PLOS ONE. 2013;8(10):e76133. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC3795771/
- Zabłocka B, Goldspink PH, Goldspink G, Górecki DC. Mechano-Growth Factor: an important cog or a loose screw in the repair machinery? Frontiers in Endocrinology. 2012;3:131. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC3485521/
- Kandalla PK, Goldspink G, Butler-Browne G, Mouly V. Mechano Growth Factor E peptide (MGF-E), derived from an isoform of IGF-1, activates human muscle progenitor cells and induces an increase in their fusion potential at different ages. Mechanisms of Ageing and Development. 2011;132(4):154–162.
- Fornaro M, Hinken AC, Needle S, et al. Mechano-growth factor peptide, the COOH terminus of unprocessed insulin-like growth factor 1, has no apparent effect on myoblasts or primary muscle stem cells. American Journal of Physiology-Endocrinology and Metabolism. 2014;306(2):E150–E156. Available at: https://journals.physiology.org/doi/full/10.1152/ajpendo.00408.2013
- Riddoch-Contreras J, Yang SY, Dick JRT, Goldspink G, Orrell RW, Greensmith L. Mechano-growth factor, an IGF-I splice variant, rescues motoneurons and improves muscle function in SOD1(G93A) mice. Experimental Neurology. 2009;215(2):281–289. Available at: https://pubmed.ncbi.nlm.nih.gov/19038252/
- Mechano growth factor, a splice variant of IGF-1, promotes neurogenesis in the aging mouse brain. Molecular Brain. 2017;10(1):23. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC5501366/
- Stavropoulou A, Halapas A, Sourla A, et al. IGF-1 expression in infarcted myocardium and MGF E peptide actions in rat cardiomyocytes in vitro. Molecular Medicine. 2009;15(5–6):127–135. Available at: https://molmed.biomedcentral.com/articles/10.2119/molmed.2009.00012
- Hameed M, Orrell RW, Cobbold M, Goldspink G, Harridge SDR. Expression of IGF-I splice variants in young and old human skeletal muscle after high resistance exercise. The Journal of Physiology. 2003;547(Pt 1):247–254. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC2342624/
- Increased nuclear stiffness via FAK-ERK1/2 signaling is necessary for synthetic mechano-growth factor E peptide-induced tenocyte migration. Scientific Reports. 2016. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC4705462/
- The nuclear localization of MGF receptor in osteoblasts under mechanical stimulation. PubMed. 2012. Available at: https://pubmed.ncbi.nlm.nih.gov/22752413/
- PEG-MGF (PEGylated Mechano Growth Factor): Research Evidence & Safety Profile. PeptideInsight. Available at: https://peptideinsight.com/en/peptides/peg-mgf
- Overexpression of Mechano-Growth Factor Modulates Inflammatory Cytokine Expression and Macrophage Resolution in Skeletal Muscle Injury. Frontiers in Physiology. 2018;9:999. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC6094977/
- World Anti-Doping Agency. The 2026 Prohibited List — Section S2 (Peptide Hormones, Growth Factors, Related Substances and Mimetics). World Anti-Doping Agency; 2026.
- Carpenter V, Matthews K, Devlin G, et al. The E-domain region of mechano-growth factor inhibits cellular apoptosis and preserves cardiac function during myocardial infarction. Journal of Cellular Physiology. 2008;217(2):267–280. Available at: https://pubmed.ncbi.nlm.nih.gov/23712705/
Educational and research-only disclaimer: This article is provided strictly for educational and informational purposes and describes the current state of scientific research on mechano growth factor (MGF). It is not medical advice, and nothing here should be interpreted as a recommendation to obtain, handle, or administer MGF or any related peptide. MGF and PEG-MGF are not approved by the FDA or any comparable regulator for human use, their human safety and efficacy have not been established, the majority of available evidence is preclinical and internally contradictory, and mechano growth factors are prohibited in competitive sport. MGF does not treat, cure, or prevent any disease. Any decision regarding peptide compounds should be made only in consultation with a qualified, licensed healthcare professional.