Epithalon (also spelled Epitalon) is a synthetic four–amino-acid peptide, alanine-glutamic acid-aspartic acid-glycine, abbreviated AEDG, that occupies an unusual place in longevity research: it is one of the very few compounds ever reported to switch telomerase back on in ordinary human cells, yet almost all of the evidence behind that reputation comes from a single research lineage in St. Petersburg, Russia. The central research question this article examines is not “does Epithalon reverse aging” — no serious body of evidence supports that framing — but rather a narrower and more honest one: what has actually been measured, in what kind of experiment, by whom, and how far can those measurements legitimately be extended toward human beings? The short answer is that the intriguing cell-culture and rodent findings have not been broadly replicated by independent laboratories, the human data are small and old, and Epithalon is not an approved drug anywhere in the West. This page is written for researchers and educated readers who want the real texture of the literature rather than the marketing gloss.
Nothing here is medical or dosing advice. Epithalon is discussed strictly as an investigational research peptide. Where studies used specific quantities in animals or cells, those are reported as historical experimental facts, not as recommendations for any human use.
What is Epithalon?
Epithalon is a synthetic tetrapeptide with the sequence Ala-Glu-Asp-Gly (AEDG) and the molecular formula C14H22N4O9.[6] Structurally it is tiny — four amino acids strung together — which is part of why it is easy and cheap to synthesise and why so many vendors offer it. That simplicity, however, should not be mistaken for well-understood pharmacology. As a recent 2025 review in the International Journal of Molecular Sciences candidly noted, even after roughly 25 years of study “the quantity of physico-chemical and structural investigations of this peptide remains quite limited.”[6] In other words, the basic biochemistry of how a four-residue peptide would survive, distribute, and act in a living organism is still not fully characterised.
From pineal extract to defined peptide
To understand Epithalon you have to start with its predecessor, Epithalamin (sometimes written epithalamin). Epithalamin is not a defined single molecule but a polypeptide extract of the pineal gland, historically prepared from bovine (cattle) pineal tissue. The pineal gland is best known for producing melatonin and for its role in circadian and seasonal rhythms, and mid-twentieth-century Soviet gerontology became interested in the idea that pineal factors might influence aging. Vladimir Khavinson and colleagues at the St. Petersburg Institute of Bioregulation and Gerontology worked to identify the “active” short peptide within that crude extract, and Epithalon (AEDG) emerged as the synthetic, chemically defined analog of what they proposed was the key bioregulatory sequence.[6] This lineage matters for two reasons. First, it means the entire Epithalon research program is downstream of one institution’s decades-long “peptide bioregulator” hypothesis. Second, it means many claims made about Epithalon are actually inherited from studies of the cruder Epithalamin extract, and the two are not interchangeable evidence.
Where Epithalon sits in the wider peptide landscape
Epithalon belongs to a family of short “Khavinson peptides” (including tripeptides and other tetrapeptides) that the same group proposed as tissue-specific regulators. If you are new to how short peptides are studied and classified in general, our practical, evidence-based guide to peptides gives useful background on why molecule size, stability, and delivery route dominate whether a peptide can do anything measurable in a body. Epithalon is also frequently grouped, in popular longevity writing, alongside compounds like NAD+ precursors and mitochondrial peptides — a grouping driven more by shared marketing themes than by shared, validated mechanisms, as we discuss later.
A note on the naming, and why it causes confusion
Three overlapping names circulate, and conflating them is one of the most common sources of overstated claims. Epithalamin is the crude bovine pineal polypeptide extract — a mixture, not a single molecule. Epithalon (or Epitalon, an alternative transliteration from Russian) is the synthetic, chemically defined AEDG tetrapeptide proposed as the “active” sequence distilled from that extract. Marketing copy routinely borrows evidence generated with the crude extract and attaches it to the defined peptide, or vice versa, as if the two were interchangeable. They are not: a defined four-residue peptide and a whole-tissue extract can differ enormously in what they contain and do. Throughout this article, where a study used the extract we say Epithalamin, and where it used the tetrapeptide we say Epithalon, precisely because that distinction is where much of the confusion — and much of the hype — lives.
Why a four-residue peptide is a hard thing to believe in
It is worth pausing on the plausibility problem, because it frames everything that follows. Orally or even by injection, most short peptides face a gauntlet: peptidases in blood and tissue that chop them within minutes, poor membrane permeability that keeps them out of cells, and — for any DNA-level mechanism — the further barrier of reaching the nucleus intact. For a tetrapeptide to survive all of that, enter cells, reach chromatin, and selectively modulate transcription is an extraordinary claim that demands extraordinary, independent evidence. This is not a reason to dismiss Epithalon out of hand, but it is the reason a skeptical reader should insist that each proposed step be demonstrated rather than assumed. The burden of proof sits with the compound, and much of that burden remains unmet.
The telomerase hypothesis: what the in-vitro evidence actually shows
A quick primer on telomeres and telomerase
To weigh the evidence you need the underlying biology, kept honest. Telomeres are repetitive DNA caps (the sequence TTAGGG in humans) at the ends of chromosomes; they protect the coding DNA from erosion and from being mistaken for broken ends. Because of how DNA replication works, most somatic cells lose a little telomere length with each division. When telomeres become critically short, cells enter replicative senescence — they stop dividing — which is one strand (among many) of the biology of aging. Telomerase is the enzyme that can rebuild telomeres; its catalytic protein subunit is hTERT. Crucially, most adult human cells keep telomerase switched off, reserving it for germline, stem, and certain immune cells. Cancers are the notable exception: the large majority reactivate telomerase to divide indefinitely. So “reactivating telomerase” is simultaneously the mechanism a longevity enthusiast hopes for and the mechanism an oncologist fears — that tension runs through the entire Epithalon story and should never be edited out of it.
It is also important to state what telomere shortening is not. Short telomeres are one correlate of aging, but aging is driven by many partly independent processes — mitochondrial decline, proteostasis failure, chronic inflammation, epigenetic drift, stem-cell exhaustion. Even if Epithalon reliably lengthened telomeres in people, that would not automatically translate into a longer, healthier life, because telomere length is a contributor to, not the master switch of, human aging. Any argument that runs “Epithalon lengthens telomeres, therefore Epithalon reverses aging” skips several unproven steps.
The single finding that made Epithalon famous is a 2003 cell-culture study by Khavinson, Bondarev, and Butyugov, published in the Bulletin of Experimental Biology and Medicine. In telomerase-negative human fetal fibroblast cultures, addition of Epithalon reportedly induced expression of the catalytic subunit of telomerase (hTERT), restored telomerase enzymatic activity, and produced measurable telomere elongation.[1] The most quoted number is that treated fibroblasts extended their replicative capacity — their Hayflick limit — by roughly 42%, dividing to a higher number of population doublings than untreated controls before senescing.[1]
Why this result is genuinely interesting
It is worth being fair to the finding. Most normal human somatic cells keep telomerase switched off, which is one reason they age and stop dividing; re-activating telomerase in an ordinary (non-cancerous, non-stem) human cell is not a trivial or expected result. If robust and general, it would be mechanistically important. This is precisely why the paper has been cited so heavily and why “telomerase peptide” became Epithalon’s identity in the supplement world.
Why it must be read narrowly
Several hard limits apply, and they are non-negotiable for honest interpretation:
- It is in vitro. These are cultured cells in a dish, not an organism. Extending the number of times a fibroblast divides on plastic tells you nothing directly about whether a person ages more slowly.
- It came from the originating lab. For roughly two decades, the telomerase result was essentially uncorroborated by fully independent groups, which is a serious weakness for any extraordinary claim.
- Telomerase reactivation is double-edged. Telomerase is also a hallmark of most cancers, which switch it on to divide without limit. A compound that reactivates telomerase in somatic cells raises, rather than settles, oncological safety questions.
A recent independent replication — with its own caveats
The picture did improve in 2025. An independent group (Al-dulaimi and colleagues), publishing in Biogerontology, reported the first comprehensive quantitative characterisation of Epithalon’s telomere effects across multiple human cell lines. In normal cells they observed telomere lengthening driven by telomerase upregulation (increased hTERT mRNA and telomerase activity after roughly three weeks of treatment); intriguingly, in cancer cell lines the telomere lengthening appeared to run through the ALT (Alternative Lengthening of Telomeres) pathway rather than telomerase.[2] This is meaningful: it is the kind of external replication the field badly needed. But the authors themselves are explicit that this “was an in vitro study using human cell lines in 2D cell cultures,” that qPCR measures only average telomere length across chromosomes, that only a handful of cell lines were tested, and that “human trials remain necessary before clinical application.”[2] A single 2025 replication strengthens the cell-biology claim; it does not convert a dish result into a human anti-aging therapy.
What would move this from “interesting” to “convincing”?
Because Epithalon marketing so often treats the cell-culture result as a finish line, it helps to spell out what the actual finish line would look like. For the telomerase claim to earn real confidence, the field would need: multiple independent laboratories reproducing the effect in several human cell types with pre-registered protocols; demonstration that the effect occurs at concentrations and exposures achievable in a living organism, not only in a dish; evidence in whole animals that telomerase activation is measurable in relevant tissues after realistic dosing; and — before any human anti-aging claim — long, controlled human trials tracking both efficacy endpoints and cancer signals. The 2025 Biogerontology paper is a first, genuine step down that path.[2] Almost every other rung on that ladder is still missing. Naming the missing rungs is not cynicism; it is simply describing the distance between where the evidence is and where the claims are.
How is Epithalon proposed to work? (These are hypotheses)
It is important to label this entire section clearly: the mechanisms below are proposed models, several of them favoured by the originating group, not settled facts. Even the 2025 review flags that “it remains uncertain whether these are the sole mechanisms of action of this compound.”[6]
The “peptide bioregulator” concept
The core theory from Khavinson’s program is that very short peptides act as signalling regulators that can enter cells, reach the nucleus, interact with DNA or chromatin, and modulate the transcription of specific genes — in effect nudging tissue-specific patterns of gene expression back toward a more “youthful” state. This is a bold idea, because most short peptides taken up by cells are simply degraded, and demonstrating that a specific tetrapeptide reaches DNA and selectively changes transcription in vivo is a very high bar. The originating group has proposed that specific short sequences correspond to specific tissues — a kind of peptide “code” — but this framework has not been independently validated as a general mechanism, and mainstream molecular biology does not recognise a settled model in which arbitrary tetrapeptides act as sequence-specific transcriptional regulators. It should be read as this program’s organising hypothesis rather than as textbook cell biology.
Gene-expression and epigenetic hypotheses
The most concrete mechanistic work supporting the “peptide touches chromatin” idea is a 2020 study in Molecules. Using human gingival mesenchymal stem cells, the authors reported that AEDG increased mRNA for the neurogenic markers Nestin, GAP43, β-Tubulin III and Doublecortin by roughly 1.6–1.8-fold, and used molecular modelling to argue that the peptide preferentially binds linker histones (H1/3 and H1/6) at sites where they contact DNA — proposing that by competing with histones it could locally ease transcription of differentiation genes.[3] This is a plausible, testable epigenetic model. It is also, again, an in-vitro stem-cell study with modelling, from the same research lineage, and it describes neurogenesis markers rather than aging outcomes.
The melatonin / pineal axis
Because Epithalon descends from a pineal extract, a long-standing hypothesis is that it acts partly through the pineal–melatonin–circadian axis, perhaps helping to normalise melatonin rhythms that flatten with age. This is frequently asserted in popular writing and is biologically not unreasonable given the origin story, but it is important to separate the well-documented origin of the molecule from a well-documented mechanism. Clean, independent human data showing that Epithalon (as opposed to the crude Epithalamin extract) meaningfully and durably restores melatonin secretion are not robust. Treat the pineal-axis mechanism as an inherited hypothesis, not a demonstrated pathway.
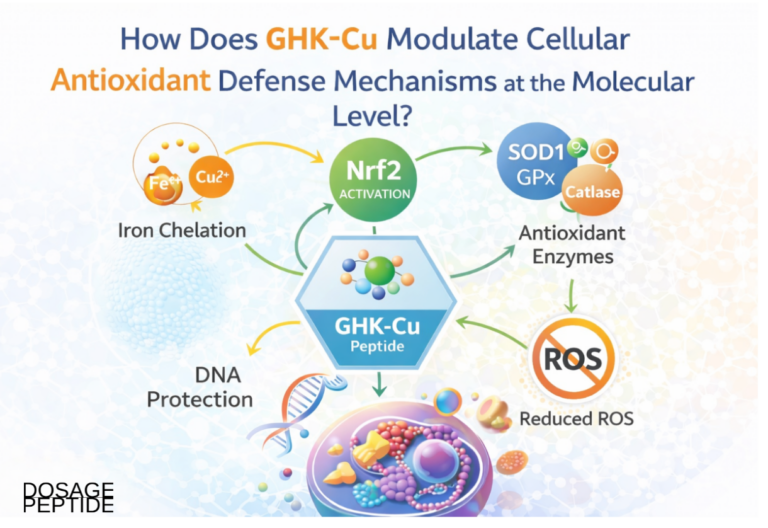
Antioxidant and other proposed activities
Beyond telomeres and chromatin, various papers ascribe additional activities to Epithalon — antioxidant effects, modulation of certain enzymes, and, in one 2025 in-vitro report, enhanced wound healing in a cell model of diabetic retinopathy. These are worth acknowledging for completeness, but they compound rather than resolve the interpretive problem: they are additional individual findings, often in specialised in-vitro systems, each of which would itself need independent replication and translation to living organisms. A long list of disparate proposed activities can create an impression of a “master molecule,” when in fact it more often signals that no single, well-validated mechanism has been pinned down. The 2025 review is explicit that it “remains uncertain whether these are the sole mechanisms of action,” which is a polite way of saying the mechanism is genuinely not settled.[6]
What do the animal studies show?
Rodent work is where the “extends lifespan” reputation originates, and it deserves careful, unromantic reading. A representative and frequently cited study is Anisimov and colleagues (2003, Biogerontology), which tested Epitalon in female Swiss-derived SHR mice: 54 animals per group received subcutaneous saline or 1.0 µg of Epitalon on five consecutive days each month.[4]
What that study actually found
The results are more nuanced than the headline “extends lifespan” suggests. In these mice, Epitalon did not change mean lifespan, body weight, or food consumption. What it did do, per the authors, was slow the age-related shutdown of estrous (reproductive) function, decrease the frequency of chromosome aberrations in bone-marrow cells by about 17% (p<0.05), increase the lifespan of the longest-lived 10% of survivors by about 13%, and raise maximum lifespan by about 12%.[4] That is a specific and limited claim: effects on maximum and tail-end survival and on some biomarkers, not a robust extension of typical (mean) lifespan.
The caveats that dominate the animal literature
| Limitation | Why it matters for interpretation |
|---|---|
| Single-lineage authorship | The large majority of positive rodent studies originate with Khavinson’s institute or close collaborators; independent replication in Western labs is sparse. |
| Modest, heterogeneous effect sizes | Reported benefits often land on maximum lifespan, tumour counts, or biomarkers rather than large, consistent mean-lifespan gains. |
| Reporting-era standards | Many studies predate modern preregistration, blinding, and effect-size reporting norms, making risk-of-bias hard to assess. |
| Species translation | Rodent geroprotection frequently fails to translate to humans even for far better-studied interventions. |
Separate reports from the same broad program have described reduced spontaneous tumour incidence and, in some tumour-prone strains, reduced malignant burden in Epitalon-treated mice. These are interesting and are part of why the peptide is discussed at all — but they carry the identical caveat: promising, preclinical, and not independently confirmed at scale. None of this establishes a human anti-cancer or anti-aging benefit.
The mean-versus-maximum-lifespan distinction
One technical point deserves emphasis because marketing consistently blurs it. Gerontologists distinguish between shifting mean lifespan (the whole survival curve moves, implying a broad slowing of aging) and shifting only maximum lifespan or the survival of the longest-lived tail (which can arise from narrower effects and is statistically noisier because it rests on a small number of animals). In the Anisimov SHR-mouse data, Epitalon did not move mean lifespan; the reported gains were in maximum lifespan and in the last 10% of survivors.[4] That is a legitimate and interesting result, but it is a narrower one than “Epithalon extends lifespan,” and it is exactly the kind of nuance that gets sanded off in a product description. A careful reader treats “extended maximum lifespan in one mouse strain from one lab” and “extends lifespan” as very different sentences.
The independence problem, stated plainly
The deepest issue with the animal literature is not any single study’s design; it is the structural fact that the corpus is dominated by one research lineage. In mainstream biomedicine, an intervention earns credibility when unrelated groups, with no stake in the original hypothesis, reproduce the effect using their own animals, reagents, and analysts. That adversarial replication is how the field guards against undetected bias, subtle methodological quirks, or publication of only favourable results. For Epithalon, that independent, adversarial rodent replication is largely absent. Until it exists, the honest stance is to regard the rodent lifespan and anti-tumour findings as a promising internal signal from one program rather than as established preclinical fact.
What about human data?
This is where honesty matters most, because the human evidence is far thinner than the confident tone of most Epithalon marketing implies. The most cited human result is a 2003 paper by Khavinson and Morozov in Neuroendocrinology Letters, titled — with characteristic boldness — “Peptides of pineal gland and thymus prolong human life.”[5]
What the cohort study reported
The study followed 266 elderly people for six to eight years. Subjects received peptide bioregulators — Epithalamin (the pineal extract) and Thymalin (a thymus extract) — during the first two to three years, and outcomes were compared with controls receiving standard care. The authors reported reduced incidence of acute respiratory disease, ischemic heart disease, hypertension and other age-related conditions, and lower mortality: roughly a 2.0–2.1-fold decrease in the Thymalin group and a 1.6–1.8-fold decrease in the Epithalamin group, with even larger reductions cited when peptides were re-administered over several years.[5]
Why this cannot bear the weight placed on it
Read carefully, this study proves much less about Epithalon than it is made to imply:
- It tested Epithalamin, not Epithalon. The human mortality claim rests on the crude pineal extract, not the defined AEDG tetrapeptide sold today. Extrapolating from one to the other is an assumption, not a finding.
- It is small, old, and single-source. A 266-person cohort from one institution, published two decades ago in a niche journal, has not been reproduced by independent groups in a modern randomised, blinded, placebo-controlled trial.
- Design limits. Long open-label follow-up cohorts are highly vulnerable to selection, attrition, and confounding; dramatic multi-fold mortality reductions from a short peptide course should invite skepticism, not credulity.
- No large modern RCT exists. There is, to date, no large, independent, contemporary randomised controlled trial demonstrating that Epithalon (AEDG) extends human life or reverses aging biomarkers.
The blunt summary: the famous “Epithalon extends human life” claim traces to a single small, old, non-independent cohort that actually studied a related extract. That is not a foundation on which any human should build health decisions.
What a credible human evidence base would require
It is fair to ask what would actually settle the question. A credible human evidence base for an anti-aging claim would need, at minimum: randomised allocation to Epithalon or placebo; blinding of participants, care providers, and outcome assessors; pre-registered primary endpoints; sample sizes large enough to detect realistic effects and to surface uncommon harms; independent sponsorship and analysis; and long follow-up — because both aging benefits and cancer risks unfold over years. Ideally several such trials would be run by different groups. None of this exists for Epithalon today. When you see a confident human claim, the single most useful question is: “compared with what, in whom, measured how, and by whom?” For Epithalon, the honest answers are, respectively, no proper control, a small old cohort, soft or extract-based endpoints, and one research lineage.
Why small old cohorts mislead
Long open-label follow-up studies are among the easiest designs to be fooled by. People who enrol in and stay with a longevity intervention often differ systematically from those who do not — they may be more health-conscious, better resourced, or simply healthier at baseline (the “healthy-user” and “healthy-adherer” effects). Without randomisation and blinding, those differences alone can manufacture large apparent mortality reductions that have nothing to do with the compound. A reported multi-fold drop in mortality from a brief peptide course is, if anything, a red flag: effect sizes that large are rarely real in geroscience, where even genuine interventions produce modest, hard-won gains. The appropriate response to such a number is heightened scrutiny of the design, not excitement.
Epithalon versus other “longevity” compounds discussed in research
Epithalon is often bundled with other compounds under a “longevity stack” banner. It is worth drawing the mechanistic contrasts — while stressing that none of these comparisons implies proven efficacy for any of them in slowing human aging.
| Compound class | Proposed primary mechanism | Evidence character |
|---|---|---|
| Epithalon (AEDG) | Proposed telomerase reactivation / chromatin-level gene regulation | In-vitro + rodent from one lineage; one 2025 independent cell replication; weak human data |
| NAD+ precursors (e.g., NMN, NR) | Restore cellular NAD+ to support metabolism, DNA-repair enzymes, sirtuins | Larger, more independent literature incl. some human trials, but durable anti-aging benefit still unproven |
| Mitochondrial peptides (e.g., MOTS-c) | Mitochondrial-derived signalling on metabolism/stress | Mostly preclinical; early-stage |
The key contrast is not that one clearly “works” better — it is that the mechanisms are entirely different (telomere biology vs. cellular metabolism) and the evidence bases differ in breadth and independence. The NAD+ field, for instance, has attracted substantially more independent investigation, though it too is far from settled; our overview of what the evidence shows about NAD+ supplements and aging lays out how even a more-studied longevity candidate resists simple “anti-aging” conclusions. Reading Epithalon next to NAD+ is a useful humility exercise: if a better-funded, more-replicated area still cannot claim victory, a single-lineage peptide certainly cannot.
There is also a lesson in how these compounds are marketed together as a “stack.” The stacking narrative implies additive or synergistic longevity benefit, but for that to be meaningful each component would first have to demonstrate an individual benefit, and then the combination would have to be tested. Neither condition is met for Epithalon-containing stacks. Combining several unproven interventions does not sum to a proven one; it multiplies the unknowns, including unknown interactions. The honest framing is that these are separate investigational compounds with separate, incomplete evidence, not a validated regimen.
Handling, stability and reconstitution in research settings
These notes describe how short lyophilised peptides are generally handled in a laboratory context. They are provided for completeness and are not a protocol for human use.
General physical handling
Epithalon is typically supplied as a lyophilised (freeze-dried) powder in a sealed vial. Like most small peptides, it is more stable dry than in solution. As a defined tetrapeptide it is comparatively simple, but the 2025 review’s observation that its physico-chemical characterisation is still limited is a reminder that batch-to-batch behaviour cannot be assumed.[6] General laboratory practice for lyophilised peptides emphasises cold storage of the sealed powder, protection from moisture and light, and preparing solutions only when needed. The specific vial sizes and quantities that appear in the Epithalon research literature — including the commonly encountered 10 mg presentation — are catalogued, with their reconstitution math, on our Epithalon 10 mg research reference page, again as documentation of what studies used rather than as guidance for human dosing.
Reconstitution basics
Reconstitution — dissolving a lyophilised peptide into a liquid — is where handling errors most often occur, because concentration and stability depend on the diluent, volume, temperature, and time in solution. The general principles (gentle addition of diluent down the vial wall, avoiding vigorous agitation, minimising freeze-thaw cycles, tracking concentration) apply to essentially all research peptides. Our peptide reconstitution guide walks through those mechanics, and the companion piece on storing peptides before and after reconstitution covers why reconstituted solutions are generally far less stable than the dry powder and are typically kept refrigerated and used within a limited window. For working out concentrations from a given vial size and diluent volume, a reconstitution calculator removes arithmetic error from the process.
Purity is a first-order problem
Because Epithalon is sold as a research chemical rather than a regulated pharmaceutical, purity, identity, and endotoxin content are not guaranteed by any Western authority. Independent certificates of analysis (mass spectrometry, HPLC purity) are the only meaningful signal a given vial contains what the label claims — and even a clean COA does not make an unapproved compound safe for a person.
Why the research-chemical supply chain is its own hazard
It is easy to focus on the biology and forget that, for an unapproved compound, the supply chain itself is a variable. Research-use-only material is not manufactured to pharmaceutical standards, is not subject to the identity, sterility, and consistency controls of an approved drug, and can vary from vendor to vendor and batch to batch. Reported problems in the grey peptide market include under- or over-potent vials, incorrect or degraded peptide, and contamination — none of which a buyer can detect by eye. A certificate of analysis helps only if it is independent, batch-specific, and verifiable, and even then it speaks to what was in a sample, not to what is in the vial in hand. This uncertainty stacks on top of the biological uncertainty: you may not know exactly what the molecule does, and you may not know exactly what you have. That combination is precisely why “research-use-only” is a meaningful label and not a formality.
Safety, unknowns and the big evidence gaps
The candid safety statement for Epithalon is short: we do not have the data to characterise its human safety. The gaps are not minor footnotes; they are the story.
- No long-term human safety data. There is no large, modern, controlled dataset on chronic Epithalon (AEDG) exposure in people. Absence of reported harm in tiny old studies is not evidence of safety.
- The telomerase question cuts both ways. The very mechanism marketed as beneficial — reactivating telomerase — is also a route cancer cells exploit. The 2025 replication’s finding that Epithalon lengthened telomeres in cancer cell lines (via ALT) is a reminder that “telomere extension” is not automatically a good thing.[2]
- No large modern RCTs of any endpoint. Aging biomarkers, mortality, cognition, sleep — none has been tested in Epithalon in a large, independent, randomised, placebo-controlled human trial.
- Not an approved drug. As of 2026, Epitalon is not FDA-approved for any indication and is not a dietary supplement; it is sold as a research-use-only chemical that is not manufactured or labelled for human use, and its compounding status in the U.S. has been described as an unsettled regulatory gray zone.
- Research-grade purity risk. Contaminants, mislabelling, and inconsistent potency are real hazards of the unregulated research-chemical market.
The unknowns are structural, not incidental
It is tempting to read a list of gaps as a to-do list that will soon be filled. For Epithalon, the gaps are better understood as structural features of where the compound sits. There is no commercial or regulatory engine driving large trials, because a cheap, unpatentable four-residue peptide offers little incentive for the expensive, independent research that would be required to establish safety and efficacy. That means the evidence vacuum is unlikely to be filled quickly, and the burden of uncertainty will keep falling on individuals rather than on a controlled trial system. We also lack the ordinary pharmacological basics a clinician would want before recommending anything: well-characterised human pharmacokinetics, dose-response and safety ceilings, interaction data with common medications, and any signal about effects in people with pre-existing cancer risk — the population for whom a telomerase-activating compound is most theoretically concerning. None of these are minor. Their absence is the reason the responsible description of Epithalon is “investigational research peptide with an interesting but unproven and largely single-source evidence base,” full stop.
Anyone genuinely weighing this compound should treat these gaps as decisive rather than as details to be optimistic past. If you want the specific quantities and reconstitution figures used in the research literature — again, as documentation, not advice — those are collected on our Epithalon 10 mg vial research dosage reference, which is written to present what studies reported rather than to endorse human use.
Why the hype outruns the evidence
Epithalon is a case study in how a scientifically interesting but preliminary finding becomes a confident consumer claim. Several forces drive the gap.
A great story compresses badly
“A pineal peptide that turns telomerase back on and extends lifespan” is an irresistible narrative. But each clause hides a qualifier: the telomerase result is in vitro; the lifespan result is in rodents and mostly affects maximum, not mean, survival; the human study used a different (crude) preparation. Marketing copy strips the qualifiers and keeps the headline.
Single-source literature masquerades as consensus
When dozens of citations trace back to one institution, a reader skimming reference counts can mistake volume for independent corroboration. The bulk of the Epithalon corpus was generated by the St. Petersburg Institute of Bioregulation and Gerontology under Khavinson and close collaborators, and even the 2025 International Journal of Molecular Sciences review — sympathetic to the compound’s “promising properties” — concedes that the evidence base remains narrow and that basic characterisation of the peptide is still limited.[6] That is not an accusation of fraud — it is a structural warning that the evidence has not been stress-tested by the wider scientific community.
The 2025 replication is progress, not vindication
It would be equally dishonest to dismiss Epithalon entirely. The independent 2025 cell-line replication genuinely strengthens the specific claim that AEDG can influence telomere biology in human cells.[2] The honest position sits between the hype and the reflexive dismissal: Epithalon is a real molecule with some reproducible cell-level effects and a long but narrow preclinical trail, whose human relevance is genuinely unknown and whose safety is uncharacterised. That is a legitimate object of continued research. It is not a validated anti-aging therapy, and no amount of confident marketing changes the state of the evidence.
Anecdote is not evidence — and here it is especially weak
Much of Epithalon’s online reputation rests on user testimonials: better sleep, more energy, subjective “anti-aging” impressions. It is worth being clear about why such reports carry almost no evidential weight for the claims at issue. Aging is slow and unmeasurable over the weeks in which people judge these effects; the outcomes users report (sleep, energy, mood) are highly susceptible to placebo, expectation, and lifestyle changes that often accompany starting a new regimen; there is no control group; and reporting is self-selected toward people motivated to perceive benefit. None of this means individuals are lying — it means the human perceptual apparatus is simply not a reliable instrument for detecting whether telomeres lengthened or lifespan changed. A compound could produce vivid subjective effects and do nothing for aging, or produce no sensation and quietly matter; anecdote cannot distinguish these. For a telomere or longevity claim, only controlled measurement counts, and that is exactly what is missing.
How to read Epithalon claims critically
- Ask whether a cited result is in vitro, animal, or human — the word “study” flattens a huge quality gap.
- Check whether the “human” evidence actually used Epithalon (AEDG) or the older Epithalamin extract.
- Look for independent replication, not just many papers from one lineage.
- Be especially wary when the marketed mechanism (telomerase) is one with known cancer-associated risks.
For readers building general fluency in evaluating peptide claims, our peptide research glossary defines the technical terms — hTERT, senescence, ALT, lyophilisation — that let you audit these claims yourself instead of trusting a vendor’s summary.
Frequently Asked Questions
Does Epithalon actually activate telomerase in humans?
Epithalon has been reported to activate telomerase and lengthen telomeres in cultured human cells, first by Khavinson’s group in 2003 and again in an independent 2025 cell-line study. Both are in-vitro results in dishes. There is no robust demonstration that Epithalon activates telomerase to any meaningful, safe, health-relevant degree in living humans. The cell-culture finding is real; its human significance is unproven.
Is Epithalon FDA-approved or legal to use?
As of 2026, Epithalon (Epitalon) is not FDA-approved for any indication and is not classified as a dietary supplement. It is sold as a research-use-only chemical that is not manufactured or labelled for human consumption, and its compounding status in the United States has been described as an unsettled regulatory gray area. It is an investigational research compound, not an approved medicine.
Did a study really show Epithalon extends human lifespan?
Not exactly. The widely cited 2003 human cohort (266 elderly subjects) tested Epithalamin, the crude pineal extract, not the defined AEDG tetrapeptide, and reported reduced mortality over six to eight years. It was small, old, single-institution, and has not been independently replicated in a modern randomised controlled trial. It cannot support a claim that Epithalon extends human life.
What did the animal studies find?
Rodent studies from Khavinson’s program reported effects such as reduced chromosome aberrations, delayed reproductive aging, and increases in maximum (not necessarily mean) lifespan, plus reduced tumour incidence in some strains. Effect sizes were modest and largely from one research lineage. Rodent geroprotection frequently fails to translate to humans, so these findings are suggestive preclinical signals, not proof of human benefit.
Is Epithalon safe?
There is no adequate long-term human safety data. Its marketed mechanism, telomerase reactivation, is also exploited by cancer cells, which raises rather than resolves safety questions, and research-grade material carries purity and mislabelling risks. Combined with the absence of large modern trials, the honest answer is that Epithalon’s human safety profile is uncharacterised, and that uncertainty should be treated as a serious limitation.
How is Epithalon different from NAD+ boosters?
They target different biology. Epithalon is proposed to act on telomere maintenance and gene expression; NAD+ precursors aim to restore cellular NAD+ for metabolism and DNA-repair pathways. The NAD+ field has more independent research, including some human trials, though durable anti-aging benefit remains unproven there too. Neither should be described as a validated way to slow human aging.
Why is so much Epithalon research from one group?
Epithalon originated at the St. Petersburg Institute of Bioregulation and Gerontology under Vladimir Khavinson, whose team developed both the parent extract Epithalamin and the synthetic AEDG peptide. Most subsequent studies came from that institute or close collaborators. Independent replication has only recently begun, which is why cautious readers weight the single-lineage evidence carefully rather than treating citation volume as scientific consensus.
What does “in vitro” mean and why does it matter here?
“In vitro” means “in glass” — experiments in cells or components outside a living organism, typically in culture dishes. Epithalon’s flagship telomerase and gene-expression findings are in vitro. Such results can reveal mechanisms but routinely fail to reproduce in whole animals or humans, where absorption, degradation, distribution, and complex physiology intervene. Treating a dish result as a proven human benefit is one of the most common errors in longevity marketing.
References
- Khavinson VKh, Bondarev IE, Butyugov AA. Epithalon peptide induces telomerase activity and telomere elongation in human somatic cells. Bull Exp Biol Med. 2003;135(6):590–592. PMID 12937682. https://pubmed.ncbi.nlm.nih.gov/12937682/
- Al-dulaimi S, Thomas R, Matta S, Roberts T. Epitalon increases telomere length in human cell lines through telomerase upregulation or ALT activity. Biogerontology. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12411320/
- Khavinson VKh, et al. AEDG peptide (Epitalon) stimulates gene expression and protein synthesis during neurogenesis: possible epigenetic mechanism. Molecules. 2020. https://pmc.ncbi.nlm.nih.gov/articles/PMC7037223/
- Anisimov VN, et al. Effect of Epitalon on biomarkers of aging, life span and spontaneous tumor incidence in female Swiss-derived SHR mice. Biogerontology. 2003;4(4):193–202. https://pubmed.ncbi.nlm.nih.gov/14501183/
- Khavinson VKh, Morozov VG. Peptides of pineal gland and thymus prolong human life. Neuro Endocrinol Lett. 2003. PMID 14523363. https://pubmed.ncbi.nlm.nih.gov/14523363/
- Araj SK, Brzezik J, Mądra-Gackowska K, Szeleszczuk Ł. Overview of Epitalon — highly bioactive pineal tetrapeptide with promising properties. Int J Mol Sci. 2025;26(6):2691. PMID 40141333. https://pubmed.ncbi.nlm.nih.gov/40141333/