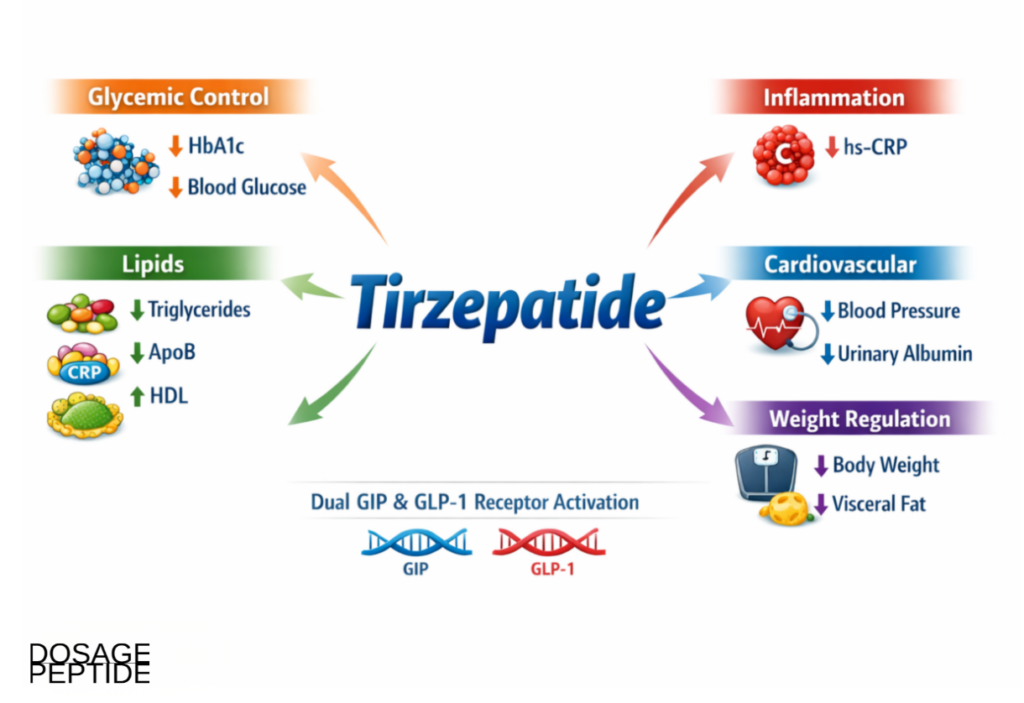
The central research question addressed here is direct: how does tirzepatide, a dual glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptor agonist, influence the panel of tirzepatide cardiometabolic biomarkers that clinicians and researchers use to gauge metabolic and cardiovascular risk? Unlike many compounds discussed in research settings, tirzepatide is not a preclinical curiosity — it is an FDA-approved medicine (marketed as Mounjaro for type 2 diabetes and Zepbound for obesity), and its effects on glycemia, lipids, inflammation, blood pressure, renal markers, adipokines, and hepatic fat have been measured across one of the largest and most rigorously designed trial programs in modern metabolic medicine. This article synthesizes that established clinical evidence, explains the receptor-level mechanisms behind each biomarker shift, and frames the findings honestly by study type, so the strength of every claim is transparent.
Dosage Peptide highlights the importance of peptide purity, batch consistency, analytical characterization, and methodological rigor in laboratory research. These principles support reproducible investigations of metabolic and hepatic pathways, helping researchers generate reliable experimental data and strengthen the interpretation of findings in controlled scientific studies.
An important framing note before the science begins. The clinical trial data summarized below were generated using pharmaceutical-grade, regulatory-approved tirzepatide administered to human participants under physician supervision. Research-grade or “research-use-only” tirzepatide sold to laboratories is a different category of material: it is not the approved product, it is not intended for human use, and it should be understood strictly as a reagent for in-vitro or controlled experimental work. Nothing here constitutes dosing advice; human dosing figures are reported only as they appear in the peer-reviewed literature, to describe what was studied.
What Are Cardiometabolic Biomarkers, and Why Study Them with Tirzepatide?
Cardiometabolic biomarkers are measurable biological signals that together describe the health of the interlocking systems governing glucose handling, lipid transport, vascular tone, inflammation, and organ stress. No single number captures cardiometabolic risk; instead, researchers assemble a panel — glycated hemoglobin, fasting glucose, insulin-resistance indices, triglycerides, apolipoprotein B, high-sensitivity C-reactive protein, systolic and diastolic blood pressure, urinary albumin excretion, adipokines, and liver enzymes — and interpret them as a coordinated picture. A therapy that moves only one marker may be useful; a therapy that shifts many markers in a favorable direction simultaneously suggests engagement of upstream regulatory biology rather than a narrow single-pathway effect.
Tirzepatide is an especially informative subject for biomarker research precisely because it engages two incretin receptors at once. This dual agonism raises a fundamental scientific question that biomarker panels are well suited to answer: are the observed cardiometabolic improvements simply downstream consequences of weight loss, or does the molecule exert direct signaling effects on metabolic and vascular tissue that are partly independent of adiposity change? The trial program was designed with prespecified and post-hoc mediation analyses specifically to interrogate that question, which is why tirzepatide has become a reference case for how to disentangle weight-dependent from weight-independent metabolic effects.
It also helps to understand why biomarkers, rather than clinical events alone, dominate this field. Cardiovascular and renal events accumulate slowly, so trials powered to detect them require thousands of participants followed for years. Biomarkers act as validated intermediaries: a change in HbA1c, ApoB, or albuminuria can be measured in weeks to months and, when the marker is causally linked to outcomes, offers an early read on likely benefit. The risk of relying on surrogates is that not every biomarker change translates faithfully into event reduction — history offers cautionary examples — which is exactly why the tirzepatide story is strengthened by having both a rich biomarker dataset and dedicated hard-outcome trials that broadly corroborate it.
Throughout this article, the emphasis is on what was measured, in whom, and how confidently. The strongest evidence comes from large randomized controlled trials with prespecified endpoints; supporting evidence comes from post-hoc analyses and imaging substudies; mechanistic plausibility comes from clamp studies and receptor pharmacology. Keeping these tiers distinct is essential to an honest reading of the tirzepatide cardiometabolic biomarker literature.
How Does Tirzepatide Work at the Molecular Level?
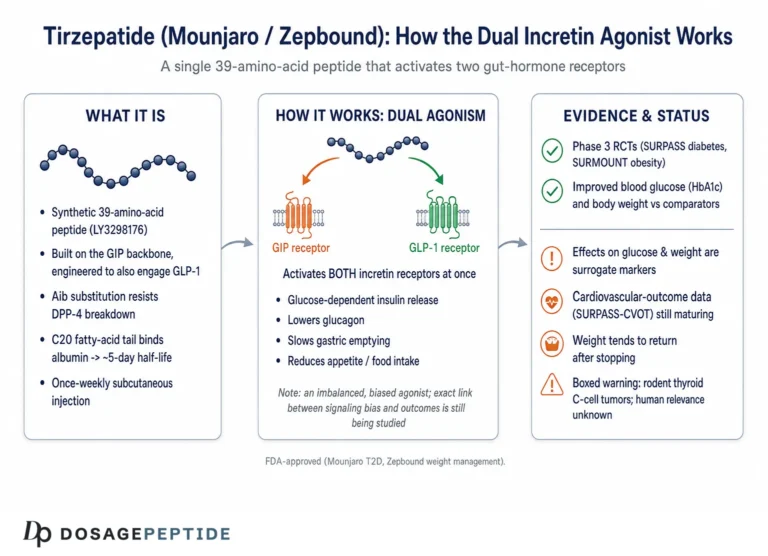
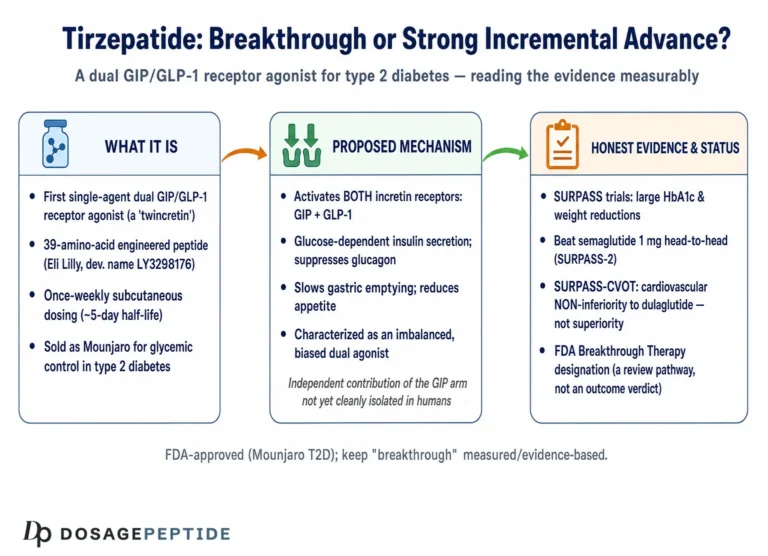
Tirzepatide is a single 39-amino-acid synthetic peptide engineered from the native GIP sequence and modified with a C20 fatty-diacid moiety that binds albumin, extending its half-life to roughly five days and enabling once-weekly administration. Functionally, it behaves as a full agonist at the GIP receptor and a partial (biased) agonist at the GLP-1 receptor. Both receptors are class B G-protein-coupled receptors, and understanding how their signaling converges is the foundation for interpreting every biomarker downstream.
What Does GLP-1 Receptor Signaling Contribute?
GLP-1 receptors are expressed on pancreatic beta cells, alpha cells, the central nervous system, the vasculature, the kidney, and the gastrointestinal tract. On the beta cell, GLP-1 receptor activation couples to the stimulatory G-protein (Gs), raising intracellular cyclic AMP (cAMP) and activating protein kinase A (PKA) and the exchange protein Epac2. The net effect is glucose-dependent amplification of insulin secretion — insulin is released more vigorously only when blood glucose is elevated, which is why incretin-based agents carry a low intrinsic risk of hypoglycemia. GLP-1 signaling also suppresses inappropriate glucagon secretion from alpha cells, slows gastric emptying to blunt postprandial glucose spikes, and acts on hypothalamic and hindbrain circuits to reduce appetite and energy intake.
What Does GIP Receptor Signaling Add?
GIP is the other major incretin hormone, and in health it is responsible for a large share of the “incretin effect” — the observation that oral glucose triggers more insulin than an equivalent intravenous glucose load. GIP receptors are found on beta cells (where GIP, like GLP-1, augments glucose-dependent insulin secretion through the cAMP/PKA axis) and, importantly, on adipocytes and in the central nervous system. The adipocyte GIP receptor is central to one of tirzepatide’s most discussed mechanisms: GIP signaling appears to improve adipose tissue insulin sensitivity, enhance postprandial lipid buffering, promote healthy triglyceride storage in subcutaneous fat, and increase local blood flow and nutrient uptake. By improving the fat cell’s ability to absorb and store incoming lipid appropriately, GIP agonism may reduce the ectopic spillover of fatty acids into liver and muscle that drives insulin resistance.
How Do cAMP, PKA, and the Incretin Effect Integrate?
Because both receptors elevate cAMP and recruit PKA in the beta cell, dual agonism produces additive and possibly synergistic insulinotropic signaling at the level of second messengers. This is the molecular basis for the larger glycemic effect observed with tirzepatide versus selective GLP-1 receptor agonists.[1] Restoring a more physiological incretin response also helps normalize the disordered insulin-to-glucagon ratio that characterizes type 2 diabetes. The biased partial agonism at the GLP-1 receptor is thought to reduce receptor internalization and preserve signaling durability, contributing to sustained effect. For readers wanting definitions of terms such as incretin effect, cAMP, or biased agonism, the site’s peptide research glossary provides plain-language entries.
How Does Central Appetite Regulation Fit In?
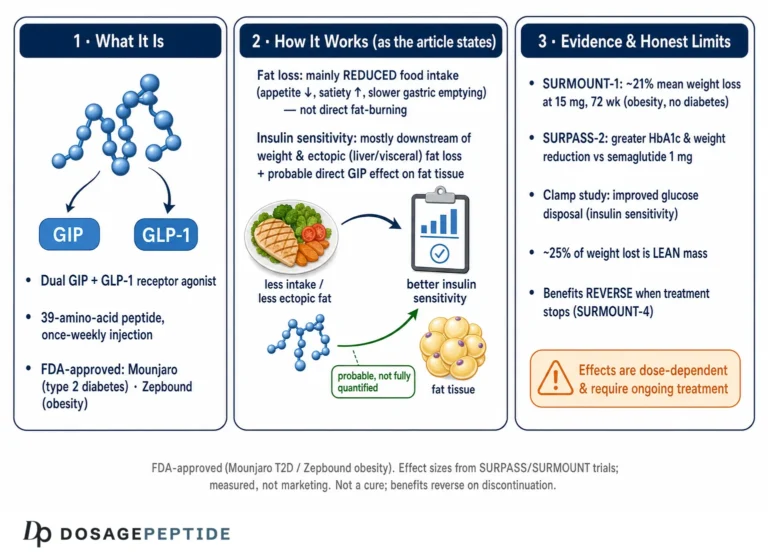
Both incretin receptors are expressed in appetite-regulating centers, including the arcuate nucleus of the hypothalamus and the area postrema and nucleus tractus solitarius in the hindbrain. Activation reduces hunger, increases satiety, and lowers caloric intake. The resulting energy deficit drives substantial weight loss, which itself improves nearly every cardiometabolic biomarker. The scientifically interesting point — explored in the mediation section below — is that many biomarker improvements are only partly explained by this appetite-driven weight loss, implying that the direct tissue-level signaling described above contributes independently.
Why Might Dual Agonism Outperform Single-Receptor Activation?
The clinical superiority of tirzepatide over a selective GLP-1 agonist on glycemia and weight[1] raises a mechanistic question: why does adding GIP agonism help, given that GIP resistance is a known feature of type 2 diabetes? Several explanations are proposed and remain areas of active research. First, restoring glycemic control with the combined effect may resensitize the GIP receptor, reviving a pathway that was blunted by hyperglycemia. Second, the GIP contribution to adipose tissue — improving insulin sensitivity, lipid buffering, and possibly local blood flow — addresses a compartment that GLP-1 agonists reach less directly. Third, central GIP signaling may complement GLP-1’s appetite effects while potentially mitigating nausea, allowing higher effective exposure. Fourth, tirzepatide’s biased, partial agonism at the GLP-1 receptor may favor sustained signaling with reduced receptor desensitization. No single explanation is settled, and the relative contribution of each receptor to specific biomarkers is precisely the kind of question that controlled receptor-pharmacology research is designed to dissect.
How Does Tirzepatide Improve Glycemic and Insulin-Sensitivity Biomarkers?
Tirzepatide improves glycemic and insulin-sensitivity biomarkers by activating both GIP and GLP-1 receptors, thereby enhancing glucose-dependent insulin secretion, suppressing inappropriate glucagon release, and improving peripheral glucose utilization. In the SURPASS phase 3 program, tirzepatide produced dose-dependent reductions in HbA1c that exceeded those observed with the selective GLP-1 receptor agonist semaglutide in a head-to-head comparison.[1]
The glycemic biomarkers most consistently reported in the clinical literature include:
- HbA1c (glycated hemoglobin): The integrated marker of average glycemia over roughly three months. Mean reductions across the SURPASS program ranged from approximately 1.9% to more than 2.4% depending on dose and background therapy, with a large proportion of participants reaching HbA1c <7% and many reaching <5.7% (the non-diabetic range).
- Fasting plasma glucose (FPG): Significant reductions reflecting suppressed overnight hepatic glucose output and improved fasting insulin action.
- HOMA-IR: A calculated index of insulin resistance derived from fasting glucose and insulin; improvements indicate enhanced peripheral and hepatic insulin sensitivity.
- C-peptide and beta-cell function indices: Markers used to infer preserved or improved insulin secretory capacity relative to prevailing glucose.
- Postprandial glucose excursions: Blunted by delayed gastric emptying and amplified meal-related insulin secretion.
In SURPASS-2, the direct comparison against semaglutide 1 mg, a prespecified exploratory analysis found that 60% of participants on the highest 15 mg tirzepatide dose achieved a composite of HbA1c ≤6.5% with ≥10% weight loss and no severe hypoglycemia, versus 22% on semaglutide.[1] The following table summarizes the general pattern of glycemic response by dose observed across the SURPASS trials; exact values vary by study population and background therapy.
| Glycemic biomarker | Direction of change | Approximate magnitude (program range) | Primary evidence |
|---|---|---|---|
| HbA1c | Decrease | −1.9% to −2.4% (5–15 mg) | SURPASS-1 to -5 RCTs[1] |
| Fasting plasma glucose | Decrease | Substantial, dose-dependent | SURPASS RCTs[1] |
| HOMA-IR | Decrease (improved sensitivity) | Improved, partly weight-independent | Mechanistic + RCT analyses |
| % reaching HbA1c <7% | Increase | Up to ~80–90% at higher doses | SURPASS-2[1] |
Collectively, these biomarker changes demonstrate that tirzepatide modifies glucose regulation at multiple checkpoints — pancreatic secretion, hepatic output, and peripheral uptake — rather than relying on a single endocrine lever. Notably, improvements in insulin-sensitivity indices occur in part independently of the magnitude of weight loss, consistent with direct receptor-mediated signaling in metabolic tissue. Researchers modeling reconstitution and preparation of research-grade material for in-vitro glucose-signaling assays often consult a structured peptide reconstitution guide to standardize concentrations before analysis.
What Do Beta-Cell Function Markers Show?
Beyond simple glucose lowering, researchers are interested in whether tirzepatide improves the quality of insulin secretion relative to demand. The disposition index — the product of insulin sensitivity and insulin secretion — is the conceptual gold standard for beta-cell function, because a healthy beta cell secretes more insulin precisely when sensitivity falls and less when sensitivity is restored. Analyses using homeostatic and clamp-derived indices report that tirzepatide improves both the insulin-sensitivity and the secretory components, consistent with the dual incretin mechanism acting on the beta cell while peripheral sensitivity improves. C-peptide, co-secreted with insulin in equimolar amounts and not cleared by the liver, is the practical marker used to gauge endogenous secretion because it is unaffected by exogenous insulin therapy. The pattern — lower fasting glucose achieved without a rise, and often with a favorable shift, in the secretion-to-sensitivity relationship — is what distinguishes an insulin-sensitizing incretin effect from simple insulin supplementation. This is one reason the glucose-dependent nature of incretin signaling matters: insulin is amplified in proportion to need rather than imposed regardless of it.
How Does Postprandial Free-Fatty-Acid Handling Change?
A less-discussed but mechanistically central biomarker domain is postprandial free fatty acid (FFA) flux. In insulin resistance, adipose tissue fails to suppress lipolysis appropriately after meals, flooding the circulation with FFAs that are taken up ectopically by liver and muscle, worsening insulin resistance in a self-reinforcing cycle. GIP receptor agonism on the adipocyte is thought to improve postprandial insulin-mediated suppression of lipolysis and enhance the buffering of dietary lipid into appropriate subcutaneous storage. The downstream consequences — lower circulating FFAs, reduced hepatic lipid delivery, and improved muscle glucose uptake — help explain why several biomarkers (triglycerides, liver fat, HOMA-IR) move together rather than independently. This coordinated adipose-liver-muscle axis is a plausible unifying mechanism behind the “systems-level” biomarker signature and is a productive target for in-vitro adipocyte and hepatocyte research using well-characterized reagents.
How Does Tirzepatide Influence Lipid and Lipoprotein Biomarkers?
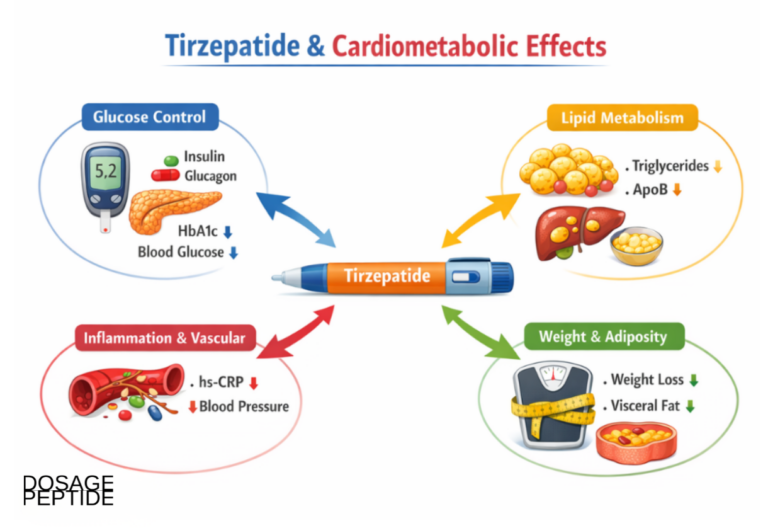
Tirzepatide influences lipid and lipoprotein biomarkers through integrated effects on adipose tissue metabolism, hepatic lipid handling, and insulin-mediated suppression of lipolysis. Trials in the SURPASS program report consistent reductions in triglycerides, very-low-density lipoprotein (VLDL) cholesterol, and apolipoprotein B, the lipid changes most tightly linked to atherogenic risk.[2]
Why Do Triglycerides and VLDL Fall?
Elevated triglycerides in insulin resistance reflect two problems: excessive hepatic production of triglyceride-rich VLDL, and impaired clearance of these particles from the circulation. Tirzepatide addresses both. By improving hepatic and adipocyte insulin sensitivity, it curbs the flux of free fatty acids to the liver and reduces de novo lipogenesis, lowering VLDL output. Simultaneously, restored insulin action enhances lipoprotein lipase activity, improving the clearance of triglyceride-rich particles after meals. The reported reductions in circulating triglycerides — often exceeding 20% at higher doses — therefore reflect coordinated changes in both production and clearance.
What Happens to ApoB, Non-HDL, and HDL?
Apolipoprotein B (ApoB) is a single-copy structural protein on each atherogenic particle (VLDL, IDL, LDL, and Lp(a)), so ApoB concentration is a direct count of atherogenic particle number and a stronger risk predictor than LDL-cholesterol alone. Tirzepatide lowers ApoB and non-HDL cholesterol, indicating a reduced atherogenic particle burden. HDL cholesterol typically remains stable or rises modestly, and the ratio of triglycerides to HDL — a surrogate of small dense LDL and insulin resistance — tends to improve. These shifts describe a lipid profile moving in a cardioprotective direction.
Because these lipid improvements occur alongside glycemic normalization and weight reduction, tirzepatide addresses several correlated cardiometabolic risk domains at once. It is worth noting, however, that the magnitude of LDL-cholesterol lowering with incretin therapies is modest relative to dedicated lipid-lowering agents; the more meaningful signal is in triglyceride-rich lipoproteins and ApoB, which respond to improved insulin action. Comparative dose-response context for the tirzepatide research literature is discussed in the site’s tirzepatide 10 mg vial dosage protocol reference, which catalogs how research-grade concentrations are typically organized.
What Effect Does Tirzepatide Have on Inflammatory Biomarkers?
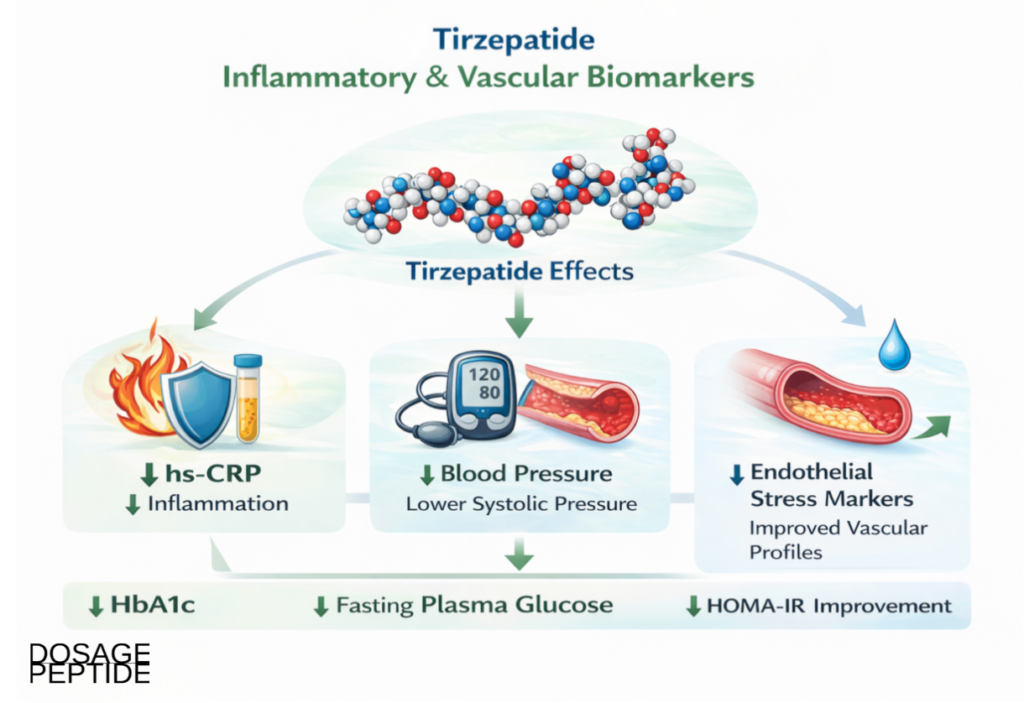
Tirzepatide affects inflammatory biomarkers primarily by reducing the systemic metabolic stress that drives low-grade inflammation. The most studied marker is high-sensitivity C-reactive protein (hs-CRP), an acute-phase reactant produced by the liver in response to interleukin-6 and a validated, independent predictor of cardiovascular events.
In a post-hoc analysis of the SURPASS-4 trial — conducted in participants with type 2 diabetes at high cardiovascular risk — tirzepatide produced substantial reductions in hs-CRP compared with insulin glargine, with a considerable proportion of participants achieving clinically meaningful decreases.[4] Critically, mediation analysis suggested that a meaningful share of the anti-inflammatory effect was not fully explained by weight loss, pointing to direct effects on adipose tissue inflammation, reduced ectopic lipid deposition, and improved insulin signaling.[4]
The inflammatory and related vascular biomarkers examined include:
- hs-CRP: Consistent reductions, partly independent of weight, indicating decreased low-grade systemic inflammation.
- Adipose-tissue inflammatory tone: Inferred improvement as visceral and ectopic fat decrease and adipocyte insulin sensitivity rises.
- Interleukin-6 axis: Because hs-CRP is downstream of IL-6, its decline implies reduced upstream inflammatory drive.
The inflammation story matters because chronic low-grade inflammation links obesity and insulin resistance to atherosclerosis. A therapy that lowers hs-CRP beyond what weight loss alone would predict is engaging inflammatory biology more directly — a finding that the SUMMIT heart-failure trial later reinforced by showing reduced C-reactive protein in a different, cardiac-focused population.[7]
How Does Tirzepatide Affect Hemodynamic and Renal Biomarkers?
Blood pressure and kidney markers are core cardiometabolic endpoints because hypertension and albuminuria are potent, modifiable drivers of cardiovascular and renal events. Tirzepatide produces favorable movement in both domains.
What Are the Blood Pressure Effects?
Across the SURPASS-1 to -5 studies, tirzepatide at 5, 10, and 15 mg was associated with significant reductions in systolic blood pressure, with end-of-study changes reported across the program ranging from roughly −2.8 to −12.6 mmHg depending on study and dose.[5] A dedicated ambulatory blood pressure monitoring substudy within SURMOUNT-1 confirmed that the effect is real and captured over a full 24-hour period rather than being an artifact of clinic measurement, showing meaningful reductions in 24-hour systolic pressure at 36 weeks versus placebo.[11] Mediation analysis of the SURPASS SBP data indicated both weight-dependent and weight-independent components, consistent with natriuretic and vascular effects layered on top of the hemodynamic benefit of weight loss.[5] Diastolic blood pressure changes are generally smaller and less consistent than systolic.
What About Kidney Biomarkers?
The urinary albumin-to-creatinine ratio (UACR) is an early, sensitive marker of glomerular stress and an independent predictor of both renal and cardiovascular outcomes. In a prespecified analysis of SURPASS-4 — a population enriched for cardiovascular and renal risk — tirzepatide slowed the decline in estimated glomerular filtration rate (eGFR) and reduced the rate of a composite kidney outcome (eGFR decline of ≥40%, renal death, progression to end-stage kidney disease, or new-onset macroalbuminuria) compared with insulin glargine, alongside marked reductions in UACR.[6] A later pooled post-hoc analysis across SURPASS-1 to -5 reinforced the albuminuria-lowering signal across the broader program.[12]
| Hemodynamic / renal biomarker | Direction | Interpretation | Primary evidence |
|---|---|---|---|
| Systolic blood pressure | Decrease (~−2.8 to −12.6 mmHg) | Weight-dependent + weight-independent | SURPASS SBP analysis[5] |
| 24-hour ambulatory SBP | Decrease | Confirms clinic finding over full day | SURMOUNT-1 ABPM[11] |
| UACR (albuminuria) | Decrease | Reduced glomerular stress | SURPASS-4 + pooled[6] |
| eGFR slope | Slower decline | Possible nephroprotection | SURPASS-4 kidney analysis[6] |
Taken together, the hemodynamic and renal biomarkers describe a coordinated reduction in vascular and glomerular strain that extends beyond glucose control. These are post-hoc and prespecified analyses of trials whose primary endpoints were glycemic or weight-based, so they are best read as strong, hypothesis-consistent signals rather than definitive proof of renal protection — a distinction the dedicated cardiovascular outcome trial helps address.
How Do Adipokines and Body-Composition Biomarkers Change?
Adipose tissue is not an inert storage depot but an active endocrine organ that secretes signaling molecules called adipokines. The two most studied are leptin, which rises with fat mass and signals energy sufficiency, and adiponectin, which improves insulin sensitivity and has anti-inflammatory properties and paradoxically falls in obesity. The ratio between them is a useful index of adipose health.
Tirzepatide-associated fat loss shifts these markers favorably: leptin declines as fat mass falls, and adiponectin tends to rise, improving the adiponectin-to-leptin ratio associated with better insulin sensitivity and lower inflammatory tone. In SURMOUNT-1, mean body-weight reductions reached approximately 15% to 21% across doses over 72 weeks in participants with obesity but without diabetes, accompanied by favorable shifts in these adiposity-linked biomarkers.[3] The GIP-receptor contribution to adipocyte biology is thought to make the quality of fat loss and adipose insulin sensitivity distinctive relative to GLP-1-only agents.
- Adipokine rebalancing: Improved adiponectin-to-leptin ratios track with enhanced insulin sensitivity and reduced inflammatory signaling.
- Ectopic and visceral fat reduction: Decreases in liver and visceral fat improve lipid flux and glucose regulation more than subcutaneous fat loss alone would predict.
- Energy-intake modulation with lean-mass considerations: Central appetite suppression reduces caloric intake; research continues on the proportion of lean versus fat mass lost, an active question across the incretin class.
An important nuance for honest interpretation: biomarker normalization frequently precedes maximal weight reduction, and several markers improve out of proportion to total weight lost. This temporal and quantitative pattern is the empirical backbone of the argument that tirzepatide modifies upstream regulatory networks influencing both adiposity and cardiometabolic risk, rather than acting solely through the downstream consequences of weight loss.
How Does Tirzepatide Affect Hepatic Biomarkers and Liver Fat?
The liver sits at the center of cardiometabolic disease. Excess ectopic fat in hepatocytes — metabolic dysfunction-associated steatotic liver disease (MASLD, formerly NAFLD) — is both a consequence of insulin resistance and a driver of it, and it correlates strongly with cardiovascular risk. Hepatic biomarkers therefore occupy a special place in the tirzepatide cardiometabolic biomarker panel.
The clearest evidence comes from the SURPASS-3 MRI substudy, which used magnetic resonance imaging to directly quantify liver fat content and abdominal fat depots rather than relying on surrogate blood tests. In participants with type 2 diabetes and a baseline liver fat content of roughly 15.7%, all three tirzepatide doses produced significantly greater reductions in liver fat content, visceral adipose tissue volume, and abdominal subcutaneous adipose tissue volume than insulin degludec over 52 weeks.[2] Because MRI-measured liver fat is a rigorous, quantitative endpoint, this substudy is among the strongest mechanistic evidence for tirzepatide’s effect on ectopic fat.
Hepatic biomarkers of interest include:
- MRI-quantified liver fat content: The gold-standard non-invasive measure, robustly reduced in SURPASS-3 MRI.[2]
- ALT and AST (aminotransferases): Liver enzymes that commonly decline as hepatic fat and inflammation fall, though they are imperfect markers of fibrosis.
- Visceral and subcutaneous adipose tissue volumes: Directly measured by MRI, both reduced, with visceral fat loss being the more metabolically consequential.
The distinction between reducing liver fat and reversing liver fibrosis is important and honest to state. Reduction of steatosis and improvement in enzymes are well documented; whether this translates into resolution of steatohepatitis and regression of fibrosis is the subject of dedicated ongoing trials in the incretin class, and should not be assumed from fat-content data alone.
What Does the SURPASS Trial Program Show About Tirzepatide Cardiometabolic Biomarkers?
The SURPASS program comprised five pivotal phase 3 randomized controlled trials in type 2 diabetes, each testing tirzepatide against a different comparator and background, which is what makes its biomarker evidence so robust. Studying the same molecule against placebo, a GLP-1 agonist, and two forms of insulin builds confidence that the biomarker effects are attributable to tirzepatide rather than to any single comparison.
| Trial | Comparator | Population focus | Key biomarker relevance |
|---|---|---|---|
| SURPASS-1 | Placebo | Drug-naive T2D | Monotherapy glycemic effect |
| SURPASS-2 | Semaglutide 1 mg | T2D on metformin | Head-to-head HbA1c & weight[1] |
| SURPASS-3 | Insulin degludec | T2D on metformin ± SGLT2i | MRI liver & visceral fat[2] |
| SURPASS-4 | Insulin glargine | T2D at high CV risk | hs-CRP, UACR, eGFR[4][6] |
| SURPASS-5 | Placebo (on insulin glargine) | T2D on basal insulin | Add-on glycemic & weight |
The SBP mediation analysis drew on all five trials to separate weight-dependent from weight-independent blood-pressure effects,[5] and the pooled albuminuria analysis similarly aggregated SURPASS-1 to -5.[12] This layered design — individual RCTs plus pooled and mediation analyses — is precisely what allows researchers to move from “the biomarker changed” toward “the biomarker changed partly because of direct drug action.” Dose-response reference material for the higher end of the research range is organized in the tirzepatide 15 mg vial dosage protocol reference.
What Does the SURMOUNT Program Add for Obesity Populations?
Where SURPASS studied type 2 diabetes, the SURMOUNT program studied obesity, extending the biomarker evidence to people without diabetes and to those with diabetes and obesity together. This matters because it separates tirzepatide’s effects from the confounding of baseline hyperglycemia and demonstrates cardiometabolic biomarker improvement across the weight spectrum.
| Trial | Population | Reported mean weight change (higher doses) | Biomarker relevance |
|---|---|---|---|
| SURMOUNT-1 | Obesity without diabetes | ~15% to 21% over 72 weeks | Adipokines, lipids, BP, glycemia[3] |
| SURMOUNT-2 | Obesity with type 2 diabetes | ~13.4% (10 mg) to 15.7% (15 mg) | Combined glycemic + weight biomarkers[9] |
| SURMOUNT-3 | Obesity, after intensive lifestyle lead-in | Substantial additional loss | Effect beyond lifestyle alone |
| SURMOUNT-4 | Obesity, randomized withdrawal | Maintenance vs regain | Durability of biomarker benefit |
The SURMOUNT-1 ambulatory blood pressure substudy discussed earlier came from this program,[11] as did evidence that cardiometabolic biomarkers improve even when baseline glucose is normal — a strong argument that these effects are not merely a byproduct of glucose lowering. SURMOUNT-2 is particularly informative because it isolates the added weight and biomarker benefit in people who already have diabetes.[9]
What Do Mediation Analyses Reveal About Adiposity-Independent Effects?
A recurring theme in this article is the question of whether tirzepatide’s biomarker effects are “just weight loss.” Mediation analysis is the statistical tool used to answer this. In simplified terms, it partitions the total effect on a biomarker into an indirect portion (mediated by weight change) and a direct portion (remaining after weight change is accounted for). A large direct component implies mechanisms beyond caloric restriction and fat loss.
Two mediation analyses are especially relevant. The hs-CRP analysis in SURPASS-4 indicated that a meaningful fraction of the anti-inflammatory effect persisted after adjusting for weight,[4] and the systolic blood pressure analysis across the SURPASS program similarly found both weight-dependent and weight-independent contributions.[5] These results are consistent with the receptor biology: GIP-mediated improvement in adipocyte function, GLP-1 effects on the vasculature and kidney, and the reduction of ectopic fat all plausibly act independently of total body weight.
An honest caveat is warranted. Mediation analysis rests on assumptions (correct temporal ordering, no unmeasured confounding of the mediator-outcome link) that are difficult to fully satisfy in post-hoc analyses of trials not designed for this purpose. The direction and consistency of the findings across multiple biomarkers and trials strengthen the inference, but the precise fraction attributable to direct effects should be treated as an estimate, not a fixed quantity.
What Do the Cardiovascular and Heart-Failure Outcome Trials Show?
Biomarkers are surrogates; the ultimate test is whether they translate into fewer clinical events. Two trials move tirzepatide from the biomarker realm toward hard outcomes.
What Did the SUMMIT Heart-Failure Trial Find?
SUMMIT was a phase 3, randomized, double-blind, placebo-controlled trial in patients with heart failure with preserved ejection fraction (HFpEF) and obesity. Tirzepatide reduced the risk of a composite of cardiovascular death or worsening heart failure and improved health status and exercise tolerance, while lowering body weight, systolic blood pressure, and C-reactive protein.[7] A cardiac imaging substudy additionally showed reductions in left ventricular mass and paracardiac adipose tissue, connecting the biomarker changes to structural cardiac remodeling.[7] This is important because HFpEF associated with obesity has historically lacked effective disease-modifying therapy.
What Did SURPASS-CVOT Show for Major Cardiovascular Events?
SURPASS-CVOT was the dedicated cardiovascular outcome trial, an event-driven, double-blind head-to-head comparison of tirzepatide against dulaglutide (a GLP-1 agonist with proven cardiovascular benefit) in over 13,000 people with type 2 diabetes and established atherosclerotic cardiovascular disease. Over a median follow-up of about four years, tirzepatide met the primary objective of non-inferiority for three-point major adverse cardiovascular events (MACE), with event rates numerically favoring tirzepatide and larger reductions in HbA1c, weight, blood pressure, and lipids.[10] Because the comparator was an active agent already known to reduce cardiovascular risk, non-inferiority is a meaningful result, and it anchors the biomarker improvements described throughout this article in a hard-outcome context.
The honest framing is that the primary result was non-inferiority (superiority for MACE was not formally established on the primary endpoint), while several secondary and metabolic endpoints favored tirzepatide. This is the appropriate level of confidence: tirzepatide’s broad biomarker profile is now corroborated by dedicated outcome data, without overstating a superiority claim the trial did not definitively demonstrate.
What Research Models and Study Designs Are Used to Measure These Biomarkers?
Understanding how biomarkers are measured is essential to weighing the evidence. The tirzepatide literature draws on a hierarchy of study designs, each with distinct strengths.
- Randomized controlled trials (RCTs): The backbone of the evidence. Randomization balances confounders, and prespecified endpoints (HbA1c, weight, blood pressure) carry the highest weight. SURPASS and SURMOUNT are the primary examples.
- Imaging substudies: MRI-based quantification of liver fat and adipose depots (SURPASS-3 MRI) and cardiac MRI (SUMMIT) provide direct, objective tissue-level measurement rather than blood surrogates.[2]
- Ambulatory monitoring substudies: 24-hour blood pressure monitoring (SURMOUNT-1 ABPM) removes clinic-measurement bias.[11]
- Hyperinsulinemic-euglycemic clamp and mechanistic studies: The reference method for quantifying insulin sensitivity, used to link receptor pharmacology to whole-body metabolism.
- Post-hoc and pooled analyses: Aggregate data to examine secondary biomarkers (hs-CRP, UACR) and to run mediation analyses; hypothesis-generating rather than confirmatory.[12]
- In-vitro and preclinical receptor pharmacology: Cell-based assays of cAMP accumulation, receptor binding, and adipocyte function that explain the mechanisms — the domain most relevant to research-grade material.
For laboratory work using research-grade peptides, standardization of preparation is a prerequisite for interpretable biomarker or receptor-assay data. Tools such as a reconstitution and concentration calculator help researchers convert between mass, volume, and molar concentration consistently across experiments, reducing a common source of between-batch variability.
How Strong Is the Evidence, by Study Type?
An honest evidence review requires grading claims by the design that supports them. The table below maps major tirzepatide cardiometabolic biomarkers to their proposed mechanism and the strongest available evidence tier.
| Biomarker family | Proposed mechanism | Strongest evidence tier |
|---|---|---|
| HbA1c / FPG | Dual incretin insulinotropy, glucagon suppression | Prespecified RCT primary endpoint (highest)[1] |
| Body weight / adiposity | Central appetite suppression + energy balance | Prespecified RCT primary/co-primary[3] |
| Liver / visceral fat | Reduced lipogenesis, improved adipose buffering | Prespecified MRI substudy (high, objective)[2] |
| Triglycerides / ApoB | Insulin-mediated lipid handling | RCT secondary endpoints (moderate-high) |
| hs-CRP | Reduced adipose inflammation, partly weight-independent | Post-hoc + mediation (moderate)[4] |
| Systolic blood pressure | Weight loss + natriuretic/vascular effects | Pooled + ambulatory substudy (moderate-high)[11] |
| UACR / eGFR | Reduced glomerular stress, hemodynamic effects | Prespecified/post-hoc renal analysis (moderate)[6] |
| MACE (hard outcome) | Aggregate cardiometabolic improvement | Dedicated CVOT, non-inferiority met (high)[10] |
The pattern is coherent: the endpoints tirzepatide was designed to hit (glycemia, weight) rest on the strongest evidence; the broader cardiometabolic biomarkers rest on a mix of secondary, post-hoc, and imaging evidence that is strong and consistent but sometimes exploratory; and the hard-outcome data now provide a confirmatory anchor. Reading the literature this way avoids both under-crediting a genuinely broad-acting molecule and over-claiming effects that remain hypothesis-generating.
How Does Tirzepatide Compare with Semaglutide and Retatrutide?
Placing tirzepatide alongside its most relevant comparators clarifies what dual and triple receptor agonism contribute to the cardiometabolic biomarker picture.
Versus semaglutide (GLP-1 only): In the head-to-head SURPASS-2 trial, tirzepatide produced greater HbA1c and weight reductions than semaglutide 1 mg.[1] The leading hypothesis is that adding GIP agonism — with its adipocyte and central effects — augments the metabolic response beyond GLP-1 activation alone. Semaglutide nonetheless remains a well-validated agent with its own robust cardiovascular outcome evidence; the two are complementary reference points rather than a simple hierarchy. Comparative research context for the GLP-1 agonist is catalogued in the semaglutide 10 mg vial dosage protocol reference.
Versus retatrutide (triple GIP/GLP-1/glucagon agonist): Retatrutide adds glucagon-receptor agonism, which increases energy expenditure and hepatic fat mobilization. In its phase 2 obesity trial, retatrutide produced mean weight reductions of up to approximately 24% at 48 weeks — numerically larger than tirzepatide — though it is at an earlier stage of clinical development and its full cardiometabolic outcome and safety profile are still being established.[8] Glucagon agonism can transiently raise glucose and heart rate, so its net cardiometabolic biomarker effect requires larger, longer trials to characterize. Research-grade reference material for the triple agonist is organized in the retatrutide 6 mg vial dosage protocol reference.
| Feature | Semaglutide | Tirzepatide | Retatrutide |
|---|---|---|---|
| Receptor targets | GLP-1 | GIP + GLP-1 | GIP + GLP-1 + glucagon |
| Regulatory status | Approved (T2D, obesity) | Approved (T2D, obesity) | Investigational (phase 3 ongoing) |
| Reported peak weight loss | ~15% (obesity trials) | ~15–22.5% (SURMOUNT-1)[3] | ~24% at 48 wk (phase 2)[8] |
| Dedicated CV outcome data | Established | Non-inferior vs dulaglutide[10] | Awaiting phase 3 outcomes |
| Distinctive biomarker feature | Broad GLP-1 effects | GIP-driven adipose sensitivity, liver fat[2] | Glucagon-driven energy expenditure |
What Are the Limitations and Open Questions?
A rigorous account of tirzepatide cardiometabolic biomarkers must state clearly what remains uncertain.
- Secondary and post-hoc status of many biomarkers: hs-CRP, UACR, and lipid endpoints were largely secondary or post-hoc. They are consistent and biologically plausible but were not the primary questions the trials were powered to answer.
- Mediation-analysis assumptions: The weight-independent effect estimates depend on assumptions that cannot be fully verified in post-hoc data; the qualitative conclusion is more secure than the precise percentages.
- Fibrosis versus steatosis: Reduced liver fat is well documented, but whether tirzepatide reverses steatohepatitis and fibrosis awaits dedicated liver-endpoint trials.
- Body-composition detail: The proportion of lean versus fat mass lost, and its long-term functional significance, is an active research question across the incretin class.
- Durability and discontinuation: Withdrawal studies suggest weight regain after stopping, raising questions about how durably biomarkers stay improved off-treatment.
- Generalizability: Trial populations may not represent all real-world groups; effects can differ by baseline HbA1c, renal function, and comorbidity.
- Research-grade material is not the studied product: All human data derive from pharmaceutical-grade tirzepatide; laboratory reagents are uncharacterized for human use and their assay behavior can vary by purity and formulation.
These limitations do not undercut the central finding — that tirzepatide moves a broad panel of cardiometabolic biomarkers favorably and now has supportive hard-outcome data — but they define the boundary between established fact and reasonable hypothesis, which is exactly where honest scientific writing should sit. For laboratory researchers, that boundary is also where the most valuable questions live: the weight-independent mechanisms, the receptor-specific contributions, and the tissue-level biology that human trials can suggest but only controlled experimental models can resolve.
How Do Tirzepatide Cardiometabolic Biomarkers Change Over Time?
The temporal sequence in which biomarkers respond is itself informative, and it is a recurring reason to doubt that weight loss alone explains the effects. Glycemic markers move first and fastest: fasting glucose falls within days to weeks of reaching an effective dose, and HbA1c — constrained by red-cell turnover — declines over the following two to three months. Blood pressure reductions also appear early, often before the bulk of weight is lost, which is one of the observations underpinning the weight-independent interpretation of the hemodynamic data.
Weight itself declines progressively across the dose-escalation period and continues for many months, with the largest reported reductions accruing over 72 weeks in the obesity trials.[3] Liver fat and visceral adipose tissue reduce over the 52-week windows used in imaging substudies, tracking with but not perfectly mirroring total weight.[2] Inflammatory markers such as hs-CRP fall relatively early, again out of proportion to the weight lost at that timepoint.[4] The general principle is that markers closest to the drug’s direct pharmacology (glucose, blood pressure, inflammation) respond earlier, while markers dependent on tissue remodeling (liver fat, adipokine set-points) evolve more slowly. Understanding this staging helps researchers design sampling schedules that capture each biomarker at an appropriate window rather than at a single arbitrary endpoint.
What Safety-Related Biomarkers Are Monitored in Tirzepatide Research?
A complete and honest biomarker account includes the parameters tracked for safety, not only those that improve. Several are routinely reported in the trial program and are relevant context for any research framing.
- Heart rate: Incretin therapies, including tirzepatide, are associated with a modest increase in resting heart rate of a few beats per minute. The clinical significance of this small chronotropic effect, set against the favorable blood-pressure and outcome data, remains an area of ongoing study.
- Pancreatic enzymes (amylase, lipase): Mild, often asymptomatic elevations in lipase and amylase have been observed with incretin agents. Their predictive value for clinically important pancreatic events is limited, and they are monitored more as a precaution than as a validated risk marker.
- Gallbladder-related markers: Rapid weight loss of any cause raises gallstone risk, so hepatobiliary parameters receive attention in longer trials.
- Gastrointestinal tolerability: Nausea, vomiting, and diarrhea are the most common adverse effects, generally dose-dependent, transient, and concentrated during dose escalation; they are the main driver of discontinuation rather than laboratory abnormalities.
Reporting these alongside the favorable cardiometabolic biomarkers is part of a balanced scientific picture. None of this constitutes clinical guidance; it simply reflects the full biomarker panel that the peer-reviewed literature tracks when characterizing the compound. The dose-escalation structure that shapes both efficacy and tolerability is described in structured research-reference material such as the tirzepatide dosage protocol reference.
Strengthening Cardiometabolic Research with Reliable Peptide Solutions at Dosage Peptide
Cardiometabolic research requires reproducible, well-characterized compounds to ensure accurate interpretation of biomarkers across studies. Variability in peptide quality, incomplete analytical documentation, and inconsistent sourcing can compromise translational relevance and data reliability. For laboratory investigators, the value of the clinical evidence summarized above lies in the questions it opens for controlled experimental work — receptor-signaling assays, adipocyte and hepatocyte models, and mechanistic studies of the weight-independent effects that mediation analyses have flagged. In all such work, research-grade tirzepatide should be handled strictly as a research reagent, not the approved therapeutic product, with attention to purity, batch consistency, and rigorous reconstitution practice so that measured biomarker or receptor responses reflect biology rather than preparation artifacts.
Frequently Asked Questions
How does tirzepatide affect cardiometabolic risk markers?
Across large randomized trials, tirzepatide lowers HbA1c, fasting glucose, triglycerides, apolipoprotein B, high-sensitivity C-reactive protein, systolic blood pressure, urinary albumin, and liver fat, while reducing body weight. These coordinated shifts arise from dual GIP and GLP-1 receptor activation acting on the pancreas, adipose tissue, brain, vasculature, and kidney, rather than from a single glucose-lowering mechanism.
Are tirzepatide’s biomarker effects only due to weight loss?
No, not entirely. Mediation analyses of blood pressure and hs-CRP indicate that a meaningful portion of the improvement persists after statistically accounting for weight change, implying direct effects on adipose function, inflammation, and vascular biology. That said, weight loss is still a major contributor, and the exact weight-independent fraction is an estimate derived from post-hoc analyses rather than a fixed value.
Which biomarkers are most commonly studied with tirzepatide?
The most frequently reported are HbA1c, fasting plasma glucose, HOMA-IR, triglycerides, VLDL, apolipoprotein B, non-HDL and HDL cholesterol, high-sensitivity C-reactive protein, systolic and diastolic blood pressure, urinary albumin-to-creatinine ratio, eGFR, adiponectin and leptin, and MRI-quantified liver and visceral fat. Together they provide an integrated assessment of cardiometabolic health.
Is tirzepatide FDA-approved, and is research-grade material the same thing?
Tirzepatide is FDA-approved as Mounjaro for type 2 diabetes and Zepbound for obesity, and all human clinical biomarker data come from that pharmaceutical-grade product. Research-grade or research-use-only tirzepatide is a separate category: it is not the approved medicine, is not intended for human use, and should be treated strictly as a laboratory reagent for in-vitro or controlled experimental study.
How does tirzepatide compare with semaglutide on biomarkers?
In the head-to-head SURPASS-2 trial, tirzepatide produced greater reductions in HbA1c and body weight than semaglutide 1 mg. The prevailing explanation is that adding GIP receptor agonism to GLP-1 activation enhances adipose insulin sensitivity and central effects. Semaglutide remains a well-established agent with strong independent cardiovascular evidence, so the comparison is best read as complementary rather than a simple ranking.
Does tirzepatide reduce liver fat?
Yes. The SURPASS-3 MRI substudy used magnetic resonance imaging to directly measure liver fat content and found significantly greater reductions with all tirzepatide doses than with insulin degludec, alongside reduced visceral and subcutaneous fat. Whether this steatosis reduction translates into reversal of steatohepatitis or fibrosis is a separate question still being tested in dedicated liver-endpoint trials.
What research models are used to measure tirzepatide biomarkers?
Evidence comes from randomized controlled trials (SURPASS, SURMOUNT), objective imaging substudies (MRI liver fat, cardiac MRI), 24-hour ambulatory blood pressure monitoring, hyperinsulinemic-euglycemic clamp studies for insulin sensitivity, pooled and post-hoc analyses for secondary markers, and in-vitro receptor pharmacology assays. Each design carries a different strength, so claims should be graded by the model that supports them.
Does tirzepatide have proven cardiovascular outcome benefits?
The dedicated SURPASS-CVOT trial found tirzepatide non-inferior to dulaglutide for three-point major adverse cardiovascular events in people with type 2 diabetes and established cardiovascular disease, with metabolic endpoints favoring tirzepatide. The SUMMIT trial separately showed benefit in heart failure with preserved ejection fraction and obesity. These outcomes support, but do not by themselves prove superiority for, every biomarker-based expectation.
References
- Frías JP, Davies MJ, Rosenstock J, et al. (2021). Tirzepatide versus semaglutide once weekly in patients with type 2 diabetes (SURPASS-2). New England Journal of Medicine, 385(6), 503–515.
- Gastaldelli A, Cusi K, Fernández Landó L, et al. (2022). Effect of tirzepatide versus insulin degludec on liver fat content and abdominal adipose tissue in people with type 2 diabetes (SURPASS-3 MRI). The Lancet Diabetes & Endocrinology, 10(6), 393–406.
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. (2022). Tirzepatide once weekly for the treatment of obesity (SURMOUNT-1). New England Journal of Medicine, 387(3), 205–216.
- Sattar N, McGuire DK, Pavo I, et al. (2023). Abstract 16779: Tirzepatide reduces high-sensitivity C-reactive protein in patients with type 2 diabetes and high cardiovascular risk — a post-hoc analysis of the SURPASS-4 trial. Circulation, 148(Suppl_1):16779.
- Lingvay I, Mosenzon O, Brown K, et al. (2023). Systolic blood pressure reduction with tirzepatide in patients with type 2 diabetes: insights from the SURPASS clinical program. Cardiovascular Diabetology, 22:66.
- Heerspink HJL, Sattar N, Pavo I, et al. (2022). Effects of tirzepatide versus insulin glargine on kidney outcomes in type 2 diabetes in the SURPASS-4 trial. The Lancet Diabetes & Endocrinology, 10(11), 774–785.
- Packer M, Zile MR, Kramer CM, et al. (2024). Tirzepatide for heart failure with preserved ejection fraction and obesity (SUMMIT). New England Journal of Medicine, 391(21), 2005–2017.
- Jastreboff AM, Kaplan LM, Frías JP, et al. (2023). Triple–hormone-receptor agonist retatrutide for obesity — a phase 2 trial. New England Journal of Medicine, 389(6), 514–526.
- Garvey WT, Frias JP, Jastreboff AM, et al. (2023). Tirzepatide once weekly for the treatment of obesity in people with type 2 diabetes (SURMOUNT-2). The Lancet, 402(10402), 613–626.
- Cardiovascular outcomes with tirzepatide versus dulaglutide in type 2 diabetes (SURPASS-CVOT). (2025). New England Journal of Medicine, 393, 2409–2420.
- de Havenon A, et al. (2024). Tirzepatide reduces 24-hour ambulatory blood pressure in adults with body mass index ≥27 kg/m²: SURMOUNT-1 ambulatory blood pressure monitoring substudy. Hypertension, 81(4), 797–806.
- Tirzepatide associated with reduced albuminuria in participants with type 2 diabetes: pooled post-hoc analysis from the SURPASS-1–5 clinical trials. (2025). Diabetes Care, 48(3), 430–439.