Few research peptides carry as much popular baggage as Melanotan II. Nicknamed the “Barbie drug” in tabloid coverage and marketed across the internet as an injectable shortcut to a suntan, it occupies an awkward space between a genuine object of laboratory pharmacology and an unregulated consumer product that regulators on three continents have repeatedly warned against.1 The central question this article examines is narrow and testable: does Melanotan II actually do what its reputation claims in sunless-tanning research, meaning pigment darkening independent of, or with minimal, ultraviolet exposure, and what does the documented record say about the price paid in safety?
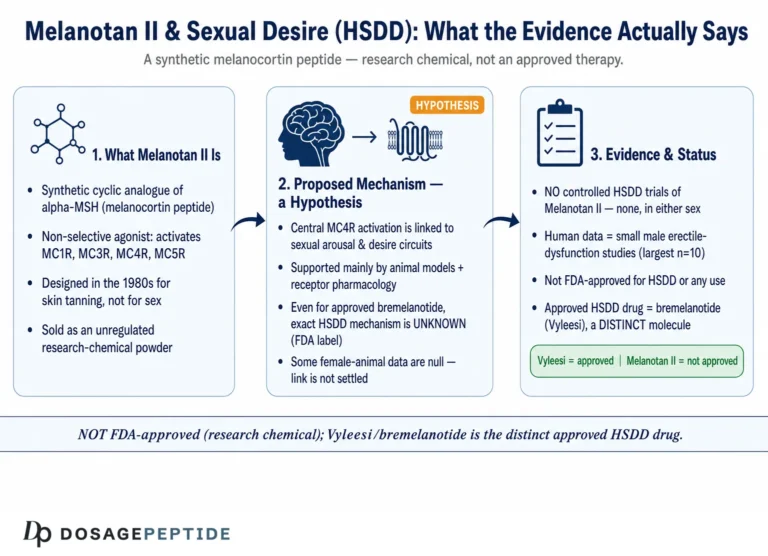
The short, honest answer is that Melanotan II is a genuinely potent stimulator of melanogenesis in laboratory and small early-phase human models, but that the depth of rigorous human evidence is shallow, ends decades ago, and was never carried through the Phase 2 and Phase 3 program that would establish efficacy and a real adverse-event incidence. What has grown instead is a body of case reports documenting harm from unregulated self-administration. Melanotan II is not approved by the U.S. Food and Drug Administration (FDA) for any use, is treated as an unlicensed medicine in the United Kingdom and Australia, and is sold in a grey market as a “research chemical not for human consumption.”1,9 A structurally related but chemically distinct analog, afamelanotide (brand name Scenesse), is FDA-approved, but only for a rare photodermatosis and only as a controlled implant, and it is a different molecule.11
This page is written for readers who want the pharmacology and the evidence hierarchy laid out plainly, with primary sources, so they can distinguish what has been measured in controlled settings from what is asserted in marketing copy. It is educational and does not endorse use. Throughout, the article labels each claim by its true evidence level: in vitro, preclinical/animal, early-phase human, case report, or investigational. Where the honest answer is “we do not know,” it says so.
What Melanotan II Is and Where It Came From
Melanotan II (frequently abbreviated MT-II or MT-2, CAS 121062-08-6, molecular formula C50H69N15O9) is a synthetic cyclic heptapeptide analog of alpha-melanocyte-stimulating hormone (alpha-MSH), one of the melanocortin peptides the body derives from the precursor protein pro-opiomelanocortin (POMC).4,5 Its full chemical name is Ac-Nle4-cyclo[Asp5,D-Phe7,Lys10]-alpha-MSH(4-10)-NH2, a compact way of describing a seven-residue fragment of the natural hormone that has been chemically rebuilt for stability and potency.3,4
The molecule was not conceived as a tanning product. It emerged from academic work at the University of Arizona in the late 1980s and early 1990s, where Victor Hruby, Mac Hadley, and colleagues were systematically engineering alpha-MSH analogs to understand and exploit the melanocortin system. Endogenous alpha-MSH is a poor drug candidate: it is degraded within minutes and has weak, transient activity. The Arizona group introduced three deliberate modifications that transformed it. First, substituting norleucine for methionine at position 4 removed the oxidation-prone sulfur atom. Second, replacing L-phenylalanine with D-phenylalanine at position 7 both increased receptor affinity and blocked cleavage by peptidases that only recognize the natural L-configuration. Third, and most importantly, a lactam bridge between the side chains of aspartate-5 and lysine-10 cyclized the peptide, locking it into the bioactive “reverse-turn” conformation and conferring marked resistance to exopeptidase and dipeptidyl-peptidase degradation.16 The result was a compound described in the pharmacology literature as “superpotent,” with far longer in vivo persistence than the parent hormone, whose half-life is under five minutes.2,16
The original therapeutic rationale was elegant. If a drug could induce the skin to produce its own protective eumelanin without requiring ultraviolet radiation, it might offer photoprotection to people at high risk of sun-induced skin damage, or a means of studying pigmentation biology. That “sunless tanning” concept is why the earliest human work was done, and it is the direct ancestor of the consumer mythology that followed. It is worth stressing the distinction the marketing world blurs: the Arizona program produced two named agents. Melanotan I, later developed as afamelanotide, is a linear analog that went through formal clinical development and is now an approved drug for a niche indication. Melanotan II is the cyclic, more broadly acting analog that was not carried through to approval as a tanning agent and instead escaped into the grey market.11,12
A second, unintended discovery shaped the compound’s later notoriety. During the early human tanning study, male volunteers reported spontaneous erections, an effect traced to the peptide’s action on central melanocortin-4 receptors rather than on skin.2 This observation was significant enough that a separate research line spun off from it: a related melanocortin agonist, bremelanotide (PT-141), was developed specifically for sexual-desire indications and eventually approved for hypoactive sexual desire disorder in premenopausal women.13 Melanotan II, then, sits at the root of a small family tree of melanocortin drugs, some approved and some not, a lineage worth keeping in mind because vendors routinely borrow the credibility of the approved relatives to sell the unapproved one. For the compound-specific handling and dosing conventions used in research settings, the dedicated Melanotan II dosage protocol collects the reconstitution math in one place.
The transition from academic reagent to internet commodity is itself instructive. Once the sequence and synthesis were published and the “tan without the sun” concept became widely known, the peptide could be manufactured cheaply by contract chemical suppliers and sold directly to consumers under the “research chemical” banner, sidestepping the drug-approval process entirely. This is a recurring pattern for melanocortin and other bioactive peptides: the science that establishes proof of concept simultaneously creates a template that an unregulated supply chain can copy. Because the molecule is stable, potent at microgram-to-milligram doses, and administered subcutaneously with ordinary insulin syringes, the practical barriers to grey-market distribution are low. Understanding this history matters because it explains why a compound with such a thin clinical dossier became so widely used: the demand was cosmetic and the supply was frictionless, while the evidence base that would normally gate a drug was simply bypassed rather than satisfied.1,9
Molecular Mechanism: The Melanocortin System

Melanotan II works by activating melanocortin receptors, a family of five G-protein-coupled receptors (MC1R through MC5R) distributed across skin, brain, adrenal cortex, and other tissues. Unlike the natural hormone, which is comparatively selective, Melanotan II is a non-selective agonist: it binds and activates MC1R, MC3R, MC4R, and MC5R with high affinity, while sparing MC2R, the adrenocorticotropic-hormone (ACTH) receptor.5 Receptor-binding studies report inhibition constants in the low-nanomolar range across the subtypes it hits, with the tightest binding at MC1R.18 The clinically and physiologically important consequence of sparing MC2R is that Melanotan II does not directly drive cortisol output the way ACTH does, so its effects are dissociated from the classic stress-steroid axis.
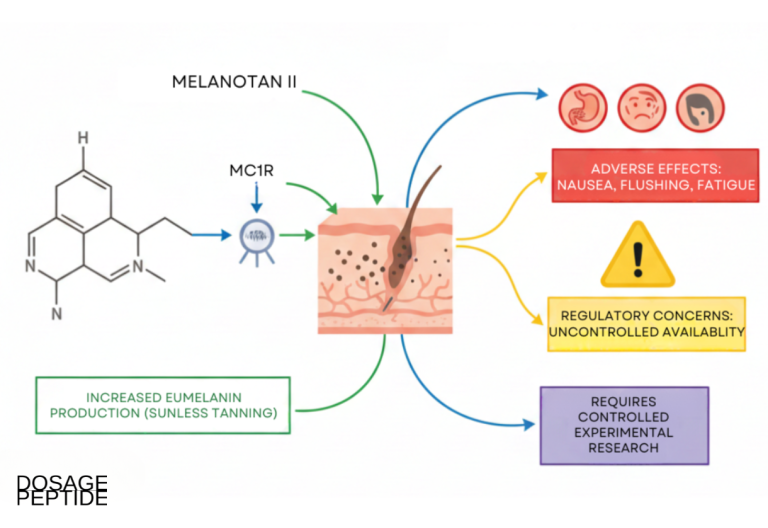
The pigmentary effect runs through MC1R on melanocytes. When Melanotan II activates MC1R, it stimulates adenylate cyclase, raising intracellular cyclic AMP, which activates protein kinase A and the transcription factor MITF. MITF in turn upregulates the enzymatic machinery of melanogenesis, chiefly tyrosinase, and shifts synthesis toward eumelanin, the darker, more photoprotective pigment, rather than the reddish pheomelanin.5,11 Because this cascade is driven pharmacologically at the receptor, it can proceed with little or no ultraviolet input, which is the entire mechanistic basis for the “sunless tan” claim. This is a real and reproducible piece of cell biology; the honest caveats are about magnitude, durability, and the collateral effects of hitting the other receptors.
| Receptor | Principal tissue | Effect of agonism relevant to MT-II |
|---|---|---|
| MC1R | Melanocytes (skin, hair) | Eumelanin synthesis; basis of the pigment-darkening effect |
| MC2R | Adrenal cortex | ACTH receptor; not activated by MT-II, so no direct cortisol drive |
| MC3R | Hypothalamus, periphery | Energy homeostasis, inflammation modulation |
| MC4R | CNS (hypothalamus, limbic) | Appetite suppression, sexual arousal, autonomic effects |
| MC5R | Exocrine glands | Sebaceous and exocrine secretion (mainly animal data) |
The non-selectivity is the crux of the whole safety story. Because Melanotan II activates central MC4R, it produces effects that have nothing to do with skin color: appetite suppression, nausea, and sexual arousal are all consequences of that receptor, and in animal models MC4R activation modulates thermogenesis, autonomic outflow, and blood pressure.5,7 Preclinical work has microinjected Melanotan II directly into the nucleus accumbens and shown it decreases both the motivation to obtain food and food consumption, an elegant demonstration of the central appetite pathway but also a reminder that this is a brain-active compound, not a cosmetic that stays in the dermis.7 Separate preclinical studies have reported that Melanotan II can promote peripheral nerve regeneration and exert neuroprotective effects in rat models, underscoring the breadth of melanocortin signaling but remaining firmly in the animal-evidence tier.8
In short, the mechanism that makes Melanotan II an interesting research probe, broad melanocortin agonism, is the same mechanism that makes it unpredictable in a whole organism. A selective MC1R agonist would, in theory, darken skin without touching appetite, arousal, or blood pressure. Melanotan II is not that; it is a blunt instrument that pushes on four of the five receptors at once, and any account of its “performance” in tanning research has to be read against that pharmacological promiscuity.
The Sunless-Tanning Evidence: What Has Actually Been Measured
Here the article addresses the headline question directly, and the discipline is to separate what was measured in controlled conditions from what is claimed online. The foundational human evidence for Melanotan II as a tanning agent is a single pilot Phase I study published in Life Sciences in 1996 by Dorr and colleagues.2 It was small: a single-blind, alternating-day, placebo-controlled trial in three healthy male volunteers, who received subcutaneous injections of Melanotan II or saline daily on weekdays for two weeks, with dose escalation in 0.005 mg/kg steps to a range of roughly 0.025 to 0.03 mg/kg. The key positive finding is real and worth stating clearly: even a handful of low-dose subcutaneous injections produced measurable increases in skin pigmentation, with tanning documented in two of the three subjects, and the darkening was dose-dependent.2 That is genuine, if thin, human proof of concept that the peptide darkens skin largely independent of deliberate UV dosing.
The same study is equally important for what it recorded on the harm side, and any faithful summary must carry both halves. The investigators documented dose-limiting adverse effects at these low research doses: nausea, facial flushing, and spontaneous penile erections, with the highest dose producing Grade II somnolence and fatigue in one subject.2 In other words, the earliest and most cited human data establish in the same breath that the compound both tans and reliably produces systemic, dose-limiting side effects, a coupling that has never been engineered apart for Melanotan II specifically.
What is striking is what did not happen next. There is no completed Phase 2 or Phase 3 tanning program for Melanotan II in the peer-reviewed record. The compound’s clinical development as a tanning agent effectively stalled; the linear cousin, afamelanotide, was the molecule that went through structured trials, and even those were for medical photoprotection, not cosmetic tanning.11 This matters enormously for the evidence hierarchy. A claim supported by one three-subject pilot from 1996 is not a claim supported by the kind of adequately powered, endpoint-driven trials that establish efficacy and quantify risk. Everything published since about Melanotan II tanning in humans is dominated not by trials but by case reports and case series describing people who bought the peptide online and injected themselves.9,10
| Evidence type | What it shows for MT-II tanning | Strength |
|---|---|---|
| In vitro / cell assays | Potent MC1R agonism drives eumelanin machinery | Strong for mechanism, silent on whole-body effect |
| Animal models | Pigment darkening plus central effects (appetite, autonomic) | Consistent, but species-limited |
| Dorr 1996 Phase I pilot | Measurable dose-dependent tanning in 2 of 3 men; dose-limiting side effects | Direct human proof of concept, but n=3 |
| Phase 2 / Phase 3 tanning trials | None completed or published | Absent |
| Post-marketing case reports | Tanning occurs; so do serious harms (see safety section) | Real-world signal, no denominator |
A further methodological wrinkle undercuts real-world efficacy claims: the pigmentary response to melanocortin agonism is genetically modulated. MC1R is highly polymorphic, and individuals carrying loss-of-function variants, common in people with red hair and fair, freckled skin who tan poorly, respond differently to receptor stimulation. This is not a footnote; it means the tanning outcome is not uniform across users, and the very people most drawn to a tanning shortcut, those who burn rather than tan, may be the least likely to darken predictably and among the most vulnerable to the mole-related harms discussed later.5 Controlled trials would normally stratify for this; the grey-market experience cannot, so anecdotal “before and after” imagery circulating online carries no information about who will respond, by how much, or at what cost.
So, does Melanotan II “perform” in sunless-tanning research? On the narrow mechanistic and proof-of-concept question, the answer is a qualified yes: it demonstrably increases eumelanin and produces visible darkening at low doses, largely without requiring UV, in the small human data that exist. But “performs in a pilot” is a categorically weaker statement than “is proven safe and effective,” and the gap between them is exactly where the compound’s real problem lives. There is no rigorous quantification of how much tan, how durably, in whom, at what dose, and at what risk. Reports and reviews consistently note that real-world users often combine Melanotan II with UV exposure anyway, and that the pigmentation is patchy and accompanied by new or darkening moles, which is not a benign cosmetic outcome but a dermatological red flag.9,10 The evidence supports the mechanism; it does not support the marketing.
Melanotan II Versus Related Melanocortin Compounds
Melanotan II is best understood in the context of its relatives, because vendors exploit the confusion among them and because the comparison clarifies what “approved” actually means. Four compounds share the melanocortin lineage but differ profoundly in selectivity, evidence, and legal standing.
Endogenous alpha-MSH is the natural benchmark: a 13-amino-acid hormone that activates melanocortin receptors but is degraded within minutes, making it useless as a drug and the reason the Arizona chemists built stabilized analogs in the first place.16 Afamelanotide (Melanotan I, Scenesse) is the linear, more MC1R-focused analog that completed formal clinical development. On October 8, 2019, the FDA approved it, delivered as a 16 mg subcutaneous implant every two months, to increase pain-free light exposure in adults with a history of phototoxic reactions from erythropoietic protoporphyria (EPP), a rare inherited photodermatosis.11 In pivotal trials, patients receiving afamelanotide spent more total hours in direct sunlight on pain-free days than those on placebo, and the drug was granted first-in-class status; it had earlier been approved in Europe.11,12 The crucial points for a reader are that afamelanotide is a different molecule from Melanotan II, is approved only for a rare disease and not for cosmetic tanning, and is administered as a controlled-release implant under medical supervision, not injected from a grey-market vial.
Bremelanotide (PT-141, Vyleesi) is the other approved relative, and its history is directly tied to Melanotan II. Because Melanotan II produced sexual arousal via central MC4R in the early tanning work, a metabolite-derived analog was developed specifically for that effect; the FDA approved bremelanotide in June 2019 as an on-demand subcutaneous injection for acquired, generalized hypoactive sexual desire disorder in premenopausal women.13 It acts on MC4R in the hypothalamus, particularly the paraventricular nucleus, engaging downstream oxytocin circuitry, a fundamentally central mechanism unlike the vascular action of PDE5 inhibitors.19 Researchers who study these pathways often cross-reference the PT-141 dosage protocol because bremelanotide is the melanocortin agonist with the most structured human sexual-function data.
| Compound | Receptor profile | Regulatory status | Approved use |
|---|---|---|---|
| alpha-MSH (natural) | Broad, low stability | Not a drug | None (endogenous hormone) |
| Afamelanotide (Melanotan I / Scenesse) | MC1R-focused | FDA-approved (2019) | Photoprotection in EPP, implant only |
| Bremelanotide (PT-141 / Vyleesi) | MC4R-preferring | FDA-approved (2019) | HSDD in premenopausal women |
| Melanotan II | Non-selective MC1/3/4/5R | Not FDA-approved | None; research chemical only |
The comparison drives home the point that “melanocortin peptide” is not a guarantee of anything. Two members of the family cleared the FDA bar by demonstrating efficacy and characterizing safety in structured trials for specific medical indications, and both are delivered under controlled conditions. Melanotan II, the very compound most heavily marketed to consumers, is the one that never completed that path. Its non-selectivity, activating pigment, appetite, arousal, and autonomic pathways simultaneously, is precisely why it is a harder molecule to develop safely than its more focused cousins, and why it has instead ended up as an unregulated product rather than a licensed medicine. Readers comparing melanocortin agents can browse the broader peptide dosage index to see how these related molecules are catalogued side by side.
Research Models and Methodology
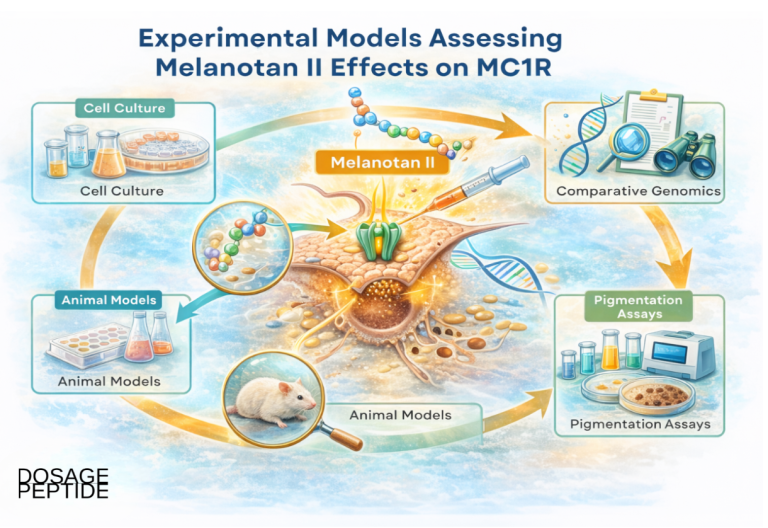
Understanding how Melanotan II is actually studied clarifies both its legitimate scientific interest and the limits of what those studies can tell us about cosmetic tanning in humans. The compound is used across several distinct experimental layers, and each answers a different question.
At the in vitro level, Melanotan II is a workhorse pharmacological tool for characterizing melanocortin receptors. Radioligand-binding assays use it to map receptor distribution and affinity across tissues; functional assays measure the cyclic-AMP response it triggers to quantify agonist potency; and cell-based melanogenesis assays in cultured melanocytes track tyrosinase activity and melanin output. Because the peptide is potent and stable, it is convenient for probing receptor signaling, desensitization, and trafficking.5,18 These studies are the source of the low-nanomolar affinity figures and the mechanistic cascade described earlier, and they are internally rigorous, but by design they say nothing about what happens in an intact, freely behaving organism.
At the preclinical animal level, Melanotan II has been administered to rodents and other species to study pigmentation, feeding behavior, energy balance, sexual behavior, and even nerve repair. The nucleus-accumbens microinjection study exemplifies the sophistication available in animal work: by delivering the peptide to a discrete brain region, investigators dissected the appetite-suppressing pathway from its other effects.7 Rat studies of peripheral-nerve regeneration and neuroprotection illustrate that the melanocortin system reaches well beyond skin.8 Animal models are indispensable for mechanism, but they carry the usual translational caveats: pigmentation biology, metabolism, and dosing scale differ between species, and a rodent’s response to a central melanocortin agonist is not a human tanning outcome.
At the early-phase human level, the record is dominated by the 1996 Dorr pilot, with its dose-escalation, alternating-day placebo design, and objective pigmentation measurement.2 Methodologically this was a reasonable Phase I design for its era, but with three participants it was powered only to detect a signal, not to estimate effect size, characterize the dose-response curve, identify responders, or catch anything but the most common adverse events. No subsequent controlled human tanning trial extended it. As a result, the “human methodology” for Melanotan II tanning essentially begins and ends with a proof-of-concept study, and everything downstream is observational.
That observational layer, the case reports and case series, is a genuine but methodologically weak source. These reports capture real harms in real users, which is valuable, but they have no control group, no denominator, and no way to verify what the person actually injected, since grey-market products are not analytically standardized. Reviews of melanotan use synthesize these reports and repeatedly flag the same problem: without regulated supply or supervised dosing, it is impossible to separate the peptide’s intrinsic risk from contamination, mis-dosing, and unsterile injection.9,10 A rigorous methodological reading, therefore, is that Melanotan II has strong mechanistic data, moderate animal data, minimal controlled human data, and a growing but uncontrolled real-world harm signal, an evidence pyramid that is broad at the bottom and almost empty where it matters most for a cosmetic claim.
For anyone approaching Melanotan II purely as a laboratory subject, the practical implication is that experimental conclusions should be pinned to the model that generated them. A cell-assay potency figure does not justify a whole-body tanning claim; an animal appetite result does not predict human tolerability; and a single small pilot does not substitute for a safety database. This is the same disciplined framing applied to other research peptides across the site, such as the analysis in the BPC-157 and TB-500 blend explainer, where the distance between preclinical enthusiasm and human proof is the entire story.
Safety and Tolerability: The Documented Risk Profile
This is the section that matters most, because the safety record is where Melanotan II’s reputation and its evidence diverge most sharply. The adverse effects fall on a spectrum from common and predictable to rare and severe, and the literature documents both ends.6,9,10
The common, dose-related effects were visible even in the tiny 1996 pilot and recur throughout case series: nausea and vomiting, facial flushing, appetite suppression, spontaneous erections in men, drowsiness and fatigue, and injection-site reactions.2,6 These are direct pharmacological consequences of broad melanocortin agonism, particularly central MC4R activation, and they are not incidental impurities; they are the drug doing what the drug does. A compound that reliably causes nausea and unwanted arousal at doses that also tan is, by definition, a compound with a narrow window between “effect” and “side effect.”
The dermatological effects are the most directly relevant to a tanning context and the most concerning. Beyond generalized darkening, users develop new melanocytic nevi, darkening and enlargement of existing moles, and eruptive or atypical (dysplastic) nevi. A published case describes eruptive dysplastic nevi following melanotan use, and a separate case report documents pigmentary changes of the oral mucosa after Melanotan II injections.10,14 Most alarming, there are case reports of melanoma appearing after initiation of melanotropic-peptide use, the great majority involving unregulated melanotan.9 The mechanistic worry is coherent: a drug that stimulates melanocyte activity and changes existing moles could plausibly complicate the early detection of melanoma or, in the worst interpretation, contribute to malignant change. Causation from case reports cannot be proven, but for a cosmetic product the mere fact that it darkens and multiplies moles, the very lesions dermatologists monitor for cancer, is a serious problem.
The rare but severe systemic effects are documented in emergency-medicine literature. A widely cited case describes a 39-year-old man who injected 6 mg of internet-purchased Melanotan II, roughly six times a typical starting research dose, and presented two hours later with diffuse body aches, sweating, and anxiety; he was admitted to intensive care with rhabdomyolysis (a creatine kinase of 17,773 IU/L) and acute kidney injury.6 Other reported severe outcomes across the melanotan literature include renal infarction, and reviews list kidney dysfunction and, rarely, cerebral edema among documented harms.9 Cardiovascular signals, including blood-pressure changes consistent with central autonomic effects, are biologically plausible and reported.9
| Severity tier | Documented effects | Evidence source |
|---|---|---|
| Common, dose-related | Nausea, flushing, appetite loss, spontaneous erections, fatigue | Phase I pilot + case series2,6 |
| Dermatological | New/darkening moles, eruptive dysplastic nevi, oral pigmentation | Case reports10,14 |
| Serious / oncologic | Melanoma after melanotan use | Case reports (causation unproven)9 |
| Severe systemic | Rhabdomyolysis, acute kidney injury, renal infarction, cerebral edema | Case reports / emergency medicine6,9 |
It is also worth naming the injection-associated hazards that sit alongside the peptide’s intrinsic pharmacology, because in practice they are inseparable from how the compound is used. Grey-market Melanotan II is reconstituted and injected by users themselves, often repeatedly over weeks of “loading,” which introduces the ordinary but non-trivial risks of any unsupervised subcutaneous injection: local infection and abscess, injection-site nodules and bruising, and, where equipment is reused or shared, the transmission of bloodborne viruses. None of these are effects of the molecule, but all of them are effects of the delivery model that the molecule’s grey-market status forces. Public-health commentary has highlighted exactly this compounding of hazards, an unlicensed brain-active drug delivered by an unregulated route from an unverified source, as the reason clinicians treat the practice as meaningfully dangerous rather than a cosmetic indulgence.15
Two structural features of this risk profile deserve emphasis. First, the severe outcomes are documented exclusively in the context of unregulated use, where dose accuracy, sterility, and product purity are all uncontrolled; the rhabdomyolysis case followed a sixfold overdose of an internet product.6 Because no formal safety trial was ever completed, the true incidence of any of these events, common or catastrophic, is simply unknown; there is no denominator.9 Second, the grey-market supply chain introduces its own hazards independent of the peptide: non-sterile reconstitution and shared needles carry infection and bloodborne-virus risk, and unverified powders may be under- or over-dosed or contaminated. Expert commentary aimed at the public has been blunt that the combination of an unlicensed, brain-active drug and an unregulated supply chain is why clinicians consider Melanotan II genuinely risky rather than a harmless cosmetic hack.15 The safety verdict is therefore not “mild and manageable” but “poorly characterized, with a real signal for serious harm and no reliable incidence data.”
Handling and Reconstitution in a Research Context
Because Melanotan II is distributed as a lyophilized (freeze-dried) powder for laboratory use, questions about reconstitution and storage come up constantly, and it is worth describing the conventions accurately while being clear that describing a laboratory procedure is not the same as endorsing administration to a person. The compound is not approved for human use, and nothing in this section should be read as instruction for self-injection.
In a research setting, a typical vial contains 10 mg of peptide as a dry cake. Reconstitution means dissolving that powder in a sterile diluent, most commonly bacteriostatic water (water containing 0.9 percent benzyl alcohol, which suppresses microbial growth and allows multi-day storage). The concentration is a matter of simple arithmetic: adding 2 mL of diluent to a 10 mg vial yields 5 mg/mL, while adding 3 mL yields approximately 3.33 mg/mL.3 The diluent should be introduced slowly down the inside wall of the vial rather than squirted directly onto the peptide cake, and the vial swirled, not shaken, because peptides are shear-sensitive and vigorous agitation can denature them or generate foam.
Storage conventions reflect peptide chemistry. Lyophilized Melanotan II is generally kept frozen, around minus 20 degrees Celsius, and is relatively stable in that state. Once reconstituted, the solution is refrigerated at 2 to 8 degrees Celsius and, per common laboratory practice, used within roughly one to two weeks, since even bacteriostatic diluent only delays, rather than prevents, degradation and contamination.3 Reconstituted peptide should be protected from light and repeated temperature cycling, and never refrozen. These handling details are why the site maintains a dedicated peptide reconstitution guide and compound-specific pages, so that the arithmetic and storage logic are documented in one consistent place rather than reinvented from vendor blurbs.
| Diluent added to 10 mg vial | Resulting concentration | Volume containing 0.5 mg |
|---|---|---|
| 2.0 mL bacteriostatic water | 5.0 mg/mL | 0.10 mL (10 units on a U-100 syringe) |
| 2.5 mL bacteriostatic water | 4.0 mg/mL | 0.125 mL (12.5 units) |
| 3.0 mL bacteriostatic water | ~3.33 mg/mL | 0.15 mL (15 units) |
The concentration table is included because it illustrates a genuine safety hazard rather than a convenience: the reason grey-market Melanotan II is dangerous is partly that these calculations are error-prone, and a decimal-place mistake or a misread syringe converts a small dose into a large one. The rhabdomyolysis case discussed earlier was, at root, a dosing error, a person injecting roughly six times a typical starting amount.6 In a regulated drug, dosing is fixed by the manufacturer and the delivery device; afamelanotide, for instance, is an implant with a predetermined payload precisely to remove this class of error.11 With a self-reconstituted grey-market vial, the user is simultaneously the chemist, the pharmacist, and the patient, with no oversight at any step. That is a structural risk that no amount of careful arithmetic fully neutralizes, and it is one more reason the handling conventions described here belong to a laboratory context and not to a bathroom counter.
Limitations and the Human-Evidence Gap
Pulling the threads together, the defining feature of Melanotan II is a mismatch between the strength of its mechanistic story and the weakness of its clinical evidence. It is worth being explicit about each limitation because the marketing narrative depends on readers not noticing them.
The first and largest gap is the absence of adequately powered human trials. The entire human efficacy claim for tanning rests on a three-person pilot from 1996.2 No Phase 2 or Phase 3 study defined the dose-response relationship, the durability of pigmentation, the proportion of responders, or the rate of adverse events in a controlled population. In evidence-based terms, that is not a foundation for asserting efficacy or safety; it is a hypothesis-generating result that was never confirmed. Any statement that Melanotan II “works” as a tanning product should be read as extrapolation from mechanism plus a pilot, not as a trial-backed conclusion.
The second gap is the lack of a safety denominator. Case reports establish that serious harms, rhabdomyolysis, kidney injury, dysplastic nevi, melanoma, have occurred in users, but they cannot tell us how often, because there is no systematic surveillance of an unregulated product and no count of how many people used it uneventfully.6,9,10 This cuts both ways rhetorically: defenders point out that millions of doses may have been used, while critics point out that we have no idea, and that the reported events include cancer and organ failure. The honest position is that the incidence is unknown and unknowable from the current data, which is itself a reason for caution rather than reassurance.
The third gap is the confound of unregulated supply. Because grey-market Melanotan II is not analytically standardized, every real-world observation is contaminated by uncertainty about what was actually administered, at what purity, and at what dose. This makes it impossible to cleanly attribute harms to the peptide itself versus to contaminants, mis-dosing, or unsterile technique, and it means the observational literature cannot substitute for controlled trials.9 The fourth gap is the translational distance between the strong preclinical data and human cosmetic outcomes: cell and animal studies are rigorous but were never designed to validate a consumer tanning claim, and non-selective central activity means whole-body effects cannot be predicted from a receptor-binding constant.5,7
Finally, there is a conceptual limitation that no additional data would fix: even a perfectly characterized tanning drug that also suppresses appetite, induces nausea, alters blood pressure, and multiplies moles would be a poor cosmetic, because the collateral effects are intrinsic to the mechanism rather than removable side effects. The approved relatives succeeded by being either more receptor-selective (afamelanotide toward MC1R) or repurposed toward the very effect that is a “side effect” for tanning (bremelanotide toward MC4R-mediated arousal). Melanotan II’s broad agonism is exactly what makes it a compelling research tool and a bad drug candidate for a purely cosmetic endpoint. Recognizing that is the difference between reading the evidence and reading the advertising.
Regulatory Status
The regulatory picture is unambiguous and is the single most important fact for a reader to retain: Melanotan II is not approved by the FDA, nor by the EMA or other major regulators, for any indication. It is not a licensed medicine anywhere for cosmetic tanning. In the grey market it is sold as a “research chemical not for human consumption,” a label that functions primarily as a legal shield for vendors rather than a description of how it is actually used.1,9
In the United States, the FDA has treated the sale of Melanotan II for human use as a violation of the Federal Food, Drug, and Cosmetic Act and has taken enforcement action against marketers of injectable tanning products, including warning letters and administrative proceedings; the agency has advised consumers not to use such products.1 In the United Kingdom, the Medicines and Healthcare products Regulatory Agency (MHRA) has stated that melanotan products are unlicensed medicines that are illegal to sell and could cause serious harm.17 In Australia, the Therapeutic Goods Administration (TGA) has been especially vocal, issuing repeated consumer warnings and intercepting melanotan products at the border, and it is illegal to supply tanning products containing melanotan without a prescription regardless of formulation, spray, tablet, injection, or cream.1,9
The contrast with the approved melanocortin analogs sharpens the point. Afamelanotide (Scenesse) is FDA-approved, but only as a subcutaneous implant for photoprotection in erythropoietic protoporphyria, a rare disease, and is administered under medical supervision; it is not available or approved for tanning.11 Bremelanotide (Vyleesi) is FDA-approved for hypoactive sexual desire disorder in premenopausal women, a completely different indication.13 Both cleared regulatory review by completing structured trials for defined medical uses. Melanotan II did neither, which is precisely why it sits outside the approved-drug system while its relatives sit inside it.
| Jurisdiction / body | Position on Melanotan II |
|---|---|
| US FDA | Not approved; sale for human use treated as FD&C Act violation; enforcement actions issued1 |
| UK MHRA | Unlicensed medicine; illegal to sell; warned it could cause serious harm17 |
| Australia TGA | Prescription-only; illegal to supply without prescription; border seizures and consumer alerts9 |
| Approved analogs | Afamelanotide (EPP, implant) and bremelanotide (HSDD) are separate, approved molecules11,13 |
A practical consequence of this status is that consumers who obtain Melanotan II have no recourse to the protections that surround an approved drug. There is no manufacturer accountable for purity or potency, no pharmacovigilance system collecting adverse-event reports, no standardized label or package insert, and no lot-to-lot consistency guarantee. If a vial is under-dosed, over-dosed, contaminated, or mislabeled, nothing in the supply chain is designed to catch it, and the “research chemical, not for human consumption” disclaimer explicitly disclaims responsibility for exactly the use that predominates. This absence of oversight is not a technicality; it is the operational difference between a medicine and a grey-market chemical, and it converts the compound’s already-thin evidence base into a genuinely uncontrolled exposure. Regulators’ warnings should be read in that light, as statements about an entire unmonitored system rather than about the molecule in isolation.1,9,15
For anyone situating Melanotan II among other unapproved research peptides, the site’s broader collections, including the peptide stacks index, catalog these compounds with the same insistence on stating regulatory status plainly. The bottom line for Melanotan II is that its legal standing matches its evidence: an interesting laboratory molecule that never became a medicine, sold in a market that regulators have explicitly warned against.
Frequently Asked Questions
Is Melanotan II FDA-approved for tanning or any other use?
No. Melanotan II is not approved by the FDA, EMA, or other major regulators for tanning or any indication. It is sold in a grey market as a research chemical “not for human consumption,” and US, UK, and Australian authorities have warned against its sale and use.1,9 The approved melanocortin drugs, afamelanotide (Scenesse) and bremelanotide (Vyleesi), are different molecules approved for different, specific medical conditions.11,13
Does the research actually show Melanotan II darkens skin without UV exposure?
The mechanism supports it and a single small human pilot demonstrated it. In the 1996 Dorr Phase I study, low-dose subcutaneous injections produced measurable, dose-dependent pigmentation in two of three volunteers, largely independent of deliberate UV dosing.2 However, this is proof of concept from three subjects, not a large controlled trial, and no Phase 2 or Phase 3 tanning study was ever completed, so the magnitude, durability, and reliability of the effect remain poorly characterized.
What is the difference between Melanotan I and Melanotan II?
Melanotan I (afamelanotide) is a linear analog with more MC1R-focused activity that completed formal trials and is FDA-approved as a subcutaneous implant for photoprotection in erythropoietic protoporphyria.11 Melanotan II is a cyclic, non-selective analog that activates MC1, MC3, MC4, and MC5 receptors, was never approved, and is the compound most heavily sold on the grey market.5 They are distinct molecules with very different regulatory standing.
Why does Melanotan II cause nausea and erections if it is a “tanning” peptide?
Because it is non-selective. Beyond MC1R on skin melanocytes, it activates central MC4 receptors in the brain, which drive appetite suppression, nausea, and sexual arousal.2,5 These are not impurities or contaminants; they are the direct pharmacology of the compound. The same MC4R effect is why a related molecule, bremelanotide, was developed specifically for sexual-desire disorders.13
What are the most serious documented risks?
Case reports document new and darkening moles, eruptive dysplastic nevi, oral mucosal pigmentation, and melanoma after melanotan use, plus severe systemic events including rhabdomyolysis with acute kidney injury and renal infarction.6,9,10,14 The dermatological effects are especially concerning because the drug changes the very moles clinicians monitor for skin cancer. Because no formal safety trial was completed, the true frequency of these events is unknown.9
Is the melanoma risk proven?
No, causation is not proven. There are multiple case reports of melanoma appearing after starting melanotropic-peptide use, most involving unregulated melanotan, but case reports cannot establish cause and effect, and there is no controlled data or denominator.9 What is established is that Melanotan II stimulates melanocyte activity and can darken and multiply moles, which at minimum can complicate the early detection of melanoma, a serious concern in its own right.
Why do vendors sell it if regulators have warned against it?
Vendors label Melanotan II a “research chemical not for human consumption,” which they use as a legal position to sell a product that is not an approved medicine. Regulators including the FDA, MHRA, and TGA have nonetheless treated its sale for human use as unlawful and issued warnings and enforcement actions.1,9 The label does not reflect how the product is typically used, and it does not make the compound safe or approved.
How is Melanotan II handled in a legitimate research setting?
It is supplied as a lyophilized powder, reconstituted with sterile bacteriostatic water to a defined concentration (for example, 5 mg/mL from 2 mL in a 10 mg vial), stored frozen before and refrigerated after reconstitution, and used within roughly one to two weeks.3 These are laboratory handling conventions, documented for accuracy on the compound’s protocol page, and are not instructions for human self-administration, which is neither approved nor endorsed.
References
- U.S. Food and Drug Administration. Notice of Opportunity for Hearing and enforcement materials regarding unapproved injectable melanotan/tanning products (Manookian; Melanocorp warning-letter coverage). Available at: https://www.fda.gov/regulatory-information/electronic-reading-room/notice-opportunity-hearing-nooh-manookian-edward-8516
- Dorr RT, Lines R, Levine N, et al. Evaluation of melanotan-II, a superpotent cyclic melanotropic peptide in a pilot phase-I clinical study. Life Sci. 1996;58(20):1777-1784. PubMed: https://pubmed.ncbi.nlm.nih.gov/8637402/
- Reconstitution and concentration conventions for Melanotan II (10 mg vial). Dosage Peptide protocol reference: https://www.dosagepeptide.com/single-peptide-dosages/melanotan-ii-10mg-vial-dosage-protocol/
- Melanotan II chemical identity and structure only (Ac-Nle4-cyclo[Asp5,D-Phe7,Lys10]-alpha-MSH(4-10)-NH2; C50H69N15O9; CAS 121062-08-6). ChemSpider (structural database): https://www.chemspider.com/Chemical-Structure.83450.html
- Melanotan II – melanocortin receptor pharmacology overview. ScienceDirect Topics: https://www.sciencedirect.com/topics/biochemistry-genetics-and-molecular-biology/melanotan-ii
- Nelson ME, Bryant SM, Aks SE. Melanotan II injection resulting in systemic toxicity and rhabdomyolysis. Clin Toxicol (Phila). 2012;50(10):1169-1173. https://www.tandfonline.com/doi/abs/10.3109/15563650.2012.740637
- Melanocortin receptor agonist melanotan-II microinjected in the nucleus accumbens decreases appetitive and consumptive responding for food. PMC/PubMed: https://pmc.ncbi.nlm.nih.gov/articles/PMC10152796/
- Melanotan-II promotes peripheral nerve regeneration and has neuroprotective properties in the rat. ScienceDirect: https://www.sciencedirect.com/science/article/abs/pii/S001429990202945X
- Habeeb Bacchus W, et al. An unhealthy glow? A review of melanotan use and associated clinical outcomes. ScienceDirect: https://www.sciencedirect.com/science/article/abs/pii/S2211266915000055
- Eruptive dysplastic nevi following melanotan use. Actas Dermo-Sifiliograficas: https://actasdermo.org/en-eruptive-dysplastic-nevi-following-melanotan-articulo-S1578219012001357
- U.S. Food and Drug Administration. FDA approves first treatment to increase pain-free light exposure in patients with a rare disorder (SCENESSE / afamelanotide 16 mg implant for erythropoietic protoporphyria; approved October 8, 2019; granted first-in-class status). FDA press announcement: https://www.fda.gov/news-events/press-announcements/fda-approves-first-treatment-increase-pain-free-light-exposure-patients-rare-disorder
- European Medicines Agency. Scenesse (afamelanotide) — European public assessment report (EU marketing authorisation for prevention of phototoxicity in adults with erythropoietic protoporphyria). https://www.ema.europa.eu/en/medicines/human/EPAR/scenesse
- U.S. Food and Drug Administration. FDA approves new treatment for hypoactive sexual desire disorder in premenopausal women (VYLEESI / bremelanotide; approved June 21, 2019). FDA press announcement: https://www.fda.gov/news-events/press-announcements/fda-approves-new-treatment-hypoactive-sexual-desire-disorder-premenopausal-women
- Changes in oral mucosa associated with Melanotan II injections: a case report. PMC: https://pmc.ncbi.nlm.nih.gov/articles/PMC12942211/
- The Conversation. No, you don’t need the “Barbie drug” to tan: why melanotan-II is so risky. https://theconversation.com/no-you-dont-need-the-barbie-drug-to-tan-whatever-tiktok-says-heres-why-melanotan-ii-is-so-risky-247445
- Al-Obeidi F, Castrucci AM, Hadley ME, Hruby VJ. Potent and prolonged-acting cyclic lactam analogues of alpha-melanotropin: design based on molecular dynamics. J Med Chem. 1989;32(12):2555-2561. (Primary medicinal-chemistry design paper for the Nle4/D-Phe7/Asp5-Lys10 lactam-bridge modifications and the short native alpha-MSH half-life.) PubMed: https://pubmed.ncbi.nlm.nih.gov/2555512/
- Medicines and Healthcare products Regulatory Agency (MHRA). Consumer warning: “‘Tan jab’ is an unlicensed medicine and may not be safe” — melanotan is an unlicensed medicine that is illegal to sell or supply in the UK and could cause serious harm. MHRA press release/consumer alert, documented at: https://www.cancerresearchuk.org/about-cancer/causes-of-cancer/sun-uv-and-cancer/fake-tan-and-melanotan-injections
- Bednarek MA, MacNeil T, Kalyani RN, Tang R, Van der Ploeg LHT, Weinberg DH. Analogs of MTII, lactam derivatives of alpha-melanotropin, modified at the N-terminus, and their selectivity at human melanocortin receptors 3, 4, and 5. Biochem Biophys Res Commun. 1999;261(1):209-213. (Primary radioligand-binding data on MT-II low-nanomolar affinity and receptor selectivity.) PubMed: https://pubmed.ncbi.nlm.nih.gov/10405347/
- Molinoff PB, Shadiack AM, Earle D, Diamond LE, Quon CY. PT-141: a melanocortin agonist for the treatment of sexual dysfunction. Ann N Y Acad Sci. 2003;994:96-102. (Peer-reviewed bremelanotide/MC4R central mechanism.) PubMed: https://pubmed.ncbi.nlm.nih.gov/12851303/
Disclaimer: This article is provided for educational and research purposes only and does not constitute medical advice. Melanotan II is not approved by the FDA or other major regulators for any use, and its sale for human consumption has been the subject of regulatory warnings. Nothing here endorses, recommends, or provides instructions for human use. Any research involving this compound should be conducted only by qualified professionals in compliance with all applicable laws, institutional oversight, and ethical standards. Individuals with health questions should consult a licensed physician.