The title of this article asks a question that, on its surface, sounds like it should have a yes-or-no answer: do clinical studies show that TB-500 really speeds recovery and reduces inflammation? The honest response has to begin by taking apart two assumptions buried in the phrasing. The first is that there is a body of clinical evidence — that is, controlled studies in humans — specifically evaluating TB-500 for recovery and inflammation. The second is that “TB-500” and the natural molecule it is derived from, thymosin beta-4, are interchangeable. Neither assumption survives contact with the primary literature. As of mid-2026, there are no completed human randomized controlled trials of the compound sold as TB-500 for athletic recovery, injury healing, or inflammatory disease.13 The regenerative and anti-inflammatory data that circulate under its name come almost entirely from cell-culture experiments and animal models, and much of it was generated with the full-length parent peptide rather than the short synthetic fragment marketed to researchers.
So rather than affirm the premise, this piece treats it as an open research question and examines it carefully. There is genuinely interesting biology here. Thymosin beta-4 is one of the most abundant intracellular proteins in mammalian cells, it has a well-characterized molecular function, and it has generated a real preclinical literature spanning skin, cornea, heart, muscle, and ligament, plus a handful of human trials in specific medical indications that have nothing to do with gym-recovery marketing.2 The task is to map what is actually known, distinguish the parent protein from the fragment, separate rodent findings from human ones, and resist the pull of confident secondary sources that quietly upgrade “promoted healing in a mouse” into “proven to speed recovery.”
This article is written for researchers and scientifically literate readers who want an accurate evidence map, not a sales page. We will cover what TB-500 is and how it differs from thymosin beta-4, the actin-sequestering mechanism and the downstream signaling it feeds, the specific molecular basis for any anti-inflammatory effect, the preclinical recovery data organized by tissue, the state of human trials, how the compound compares with related repair peptides, dosing and handling in a research context, safety, and regulatory status — including the fact that TB-500 is explicitly banned in sport. Throughout, the governing principle is restraint. TB-500 is a research peptide, not an approved therapy for any condition, and nothing here should be read as suggesting it treats, cures, or prevents any disease.
What TB-500 Actually Is — a Fragment, Not the Whole Protein
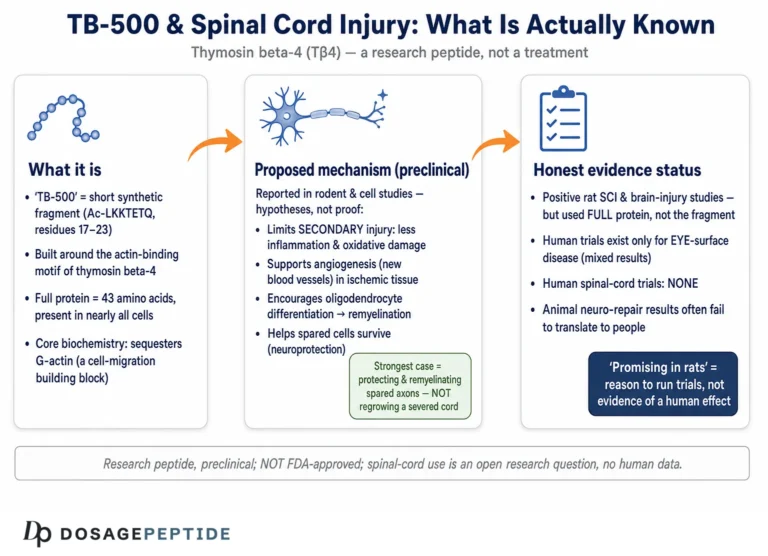
The single most important distinction for thinking clearly about this compound is the one that popular writing almost always blurs: TB-500 is not thymosin beta-4. Thymosin beta-4 (Tβ4) is a natural 43-amino-acid polypeptide, one of the most abundant of the beta-thymosins, found at high concentration in the cytoplasm of nearly all mammalian cell types and released into wound fluid, blood, and other tissues.3 It is a genuine biological molecule with an evolved function. TB-500, by contrast, is a synthetic construct. Most material sold under that name is a short peptide corresponding to the central actin-binding domain of Tβ4 — commonly the sequence around residues 17–23, often written as the acetylated heptapeptide Ac-Leu-Lys-Lys-Thr-Glu-Thr-Gln (Ac-LKKTETQ) — the motif responsible for the protein’s interaction with actin.14
This matters enormously, and it is a recurring source of confusion in commercial literature that treats the two as one. When a vendor cites a cardiac-repair study, a corneal-healing trial, or a wound-healing experiment, the overwhelming majority of that work was performed with full-length Tβ4, frequently the clinical-grade synthetic 43-mer (as in RegeneRx’s RGN-259 and RGN-137 programs), not with the LKKTETQ fragment.8 The fragment reproduces the actin-binding motif, but a 7-residue peptide is not guaranteed to reproduce all of the parent’s activities. Tβ4 has additional functional regions — an N-terminal domain implicated in some of its extracellular signaling and a distinct segment associated with its angiogenic activity — that a short central fragment may only partially capture. So every time you read that “TB-500 has been shown to” do something, the correct first question is: was that shown with TB-500, or with Tβ4? In most cases the answer is Tβ4, and the extrapolation to the fragment is an assumption, not a finding.
A useful way to hold this in mind is to keep three entities distinct. The parent protein is full-length Tβ4, a 43-residue multifunctional peptide with actin-sequestering, pro-migratory, pro-angiogenic, and anti-inflammatory activities documented across many tissues.2 The active motif is the actin-binding LKKTETQ region, the structural heart of the actin interaction. The research compound is TB-500, a synthetic peptide built around that motif and marketed for laboratory and (illicitly) athletic use. Reasoning slides from strong to weak as you move down this ladder: the parent has the richest evidence, the motif has a defined biochemical role, and the fragment inherits an assumption of equivalence that the data only partly justify. Collapsing all three into “TB-500” is the error that makes the compound sound far better validated than it is.
Why does the fragment exist at all, if the full protein is the better-studied molecule? Practical reasons: a short peptide is cheaper and easier to synthesize, more stable, and simpler to handle than a 43-mer. The name “TB-500” itself originated in the veterinary and gray-market performance world rather than in a pharmaceutical development program, which is part of why its identity is so loosely defined — different suppliers may sell the heptapeptide, a longer fragment, or even full-length Tβ4 under the same label, with no regulatory oversight guaranteeing what is in the vial. That ambiguity is not a footnote; it is central to interpreting any claim about the compound, because the biological activity of what a given researcher actually receives may differ from what the published Tβ4 literature describes.
The Actin-Sequestering Mechanism and What Follows From It
The best-characterized molecular function of thymosin beta-4 — and the one the TB-500 fragment is built to reproduce — is the sequestration of monomeric actin. Actin exists inside cells in two interconverting forms: globular monomers (G-actin) and filamentous polymers (F-actin). The assembly and disassembly of actin filaments drives cell shape change, crawling, and migration. Tβ4 binds G-actin with roughly 1:1 stoichiometry and a dissociation constant in the sub-micromolar range, holding a large reserve of monomers in a polymerization-ready but unpolymerized state.3 Because Tβ4 is so abundant, it functions as the cell’s principal actin buffer, setting the size of the free-monomer pool that can be rapidly mobilized when a cell needs to build new filaments and move.
This is the pivot point for the whole story. By regulating the availability of actin monomers, Tβ4 facilitates cell migration — and directed cell migration is fundamental to tissue repair. Keratinocytes must migrate to re-epithelialize a wound; endothelial cells must migrate to form new vessels; fibroblasts and myofibroblasts must migrate to lay down and contract matrix; and progenitor cells must migrate to sites of damage. Tβ4 promotes the migration of all of these cell types, which is the mechanistic core of its reputation as a repair molecule.4 The LKKTETQ motif is the part of the protein that engages actin, which is why the TB-500 fragment is expected to retain at least this pro-migratory function.
But actin sequestration is only the beginning, and here the biology becomes both more interesting and more uncertain. Tβ4 has documented effects that are not obviously explained by actin binding alone. A landmark study showed that Tβ4 forms a functional complex with the adaptor protein PINCH and integrin-linked kinase (ILK), activating the pro-survival kinase Akt; after coronary artery ligation in mice, Tβ4 treatment upregulated ILK and Akt activity, enhanced early cardiomyocyte survival, and improved cardiac function.1 This ILK/Akt survival axis is a genuinely distinct mechanism from monomer buffering, and it points to Tβ4 acting as a signaling molecule, not merely a cytoskeletal sponge. Separately, Tβ4 upregulates vascular endothelial growth factor and promotes endothelial differentiation and blood-vessel formation, contributing an angiogenic arm to its repair activity.5
There is a further wrinkle worth understanding, because it recurs across the primary literature: the oxidation state of the peptide appears to matter. Tβ4 contains a methionine residue that can be oxidized to Tβ4-sulfoxide, and several studies report that the sulfoxide form is the biologically active species for particular effects — it is the sulfoxide that attenuates inflammatory cell infiltration after cardiac injury, and both native and sulfoxidized Tβ4 chemoattract myoblasts.711 This is not a trivial detail. It means that the relationship between the molecule administered and the molecule that actually does the work is mediated by a redox conversion that depends on the local tissue environment. A researcher cannot simply assume that a given batch of TB-500 fragment, which may or may not include the relevant methionine and may or may not oxidize in the same way, reproduces the sulfoxide-dependent activities described for the full protein. The biology is more conditional than the confident single-mechanism story implies.
An honest mechanistic summary is therefore layered. The actin-sequestering function is solid, well-quantified, and plausibly reproduced by the TB-500 fragment. The downstream migratory consequences are well supported for the parent protein. The additional signaling activities — ILK/Akt survival, VEGF-driven angiogenesis, and the anti-inflammatory effects discussed below — are documented for Tβ4 but are less certain to transfer fully to a 7-residue fragment, because some of these activities have been mapped to regions of the protein outside the central actin-binding motif, and some depend on oxidation state. This is precisely the kind of nuance that marketing copy erases when it attributes the entire Tβ4 mechanistic portfolio to “TB-500.” For readers surveying how these repair-oriented peptides are catalogued and distinguished, the site’s dosage index organizes them by their proposed mechanistic profiles.
How TB-500 Might Reduce Inflammation: the Molecular Case
The anti-inflammatory half of the title’s question deserves its own mechanistic treatment, because it is often asserted casually and rarely explained. The claim is not baseless — there is real preclinical work behind it — but it is specific, and it is largely parent-protein data.
The most direct molecular evidence comes from work on the nuclear factor-κB (NF-κB) pathway, the master transcriptional switch that drives the expression of inflammatory cytokines and chemokines. In corneal epithelial cells, Tβ4 inhibited tumor necrosis factor-α (TNF-α)–induced NF-κB activation and suppressed the downstream expression of interleukin-8 (IL-8), a key neutrophil chemoattractant; intriguingly, the study also implicated Tβ4’s binding partners PINCH-1 and ILK in tuning this response.6 Dampening NF-κB signaling is a coherent, mechanistically specific way to reduce inflammation, because so many inflammatory mediators are NF-κB targets. This is the strongest single piece of molecular evidence for an anti-inflammatory action, and it ties back neatly to the same ILK/PINCH complex implicated in Tβ4’s survival signaling.
A second strand comes from cardiac injury models. Beyond promoting cell survival, Tβ4 (and notably its oxidized derivative, Tβ4-sulfoxide) has been reported to attenuate inflammatory cell infiltration and promote wound healing after myocardial injury, shifting the healing environment away from destructive inflammation.7 More broadly, review syntheses of the animal literature describe Tβ4 as down-regulating inflammatory chemokines and cytokines across multiple tissue-injury settings, in parallel with its pro-migratory and pro-angiogenic effects.2 The picture that emerges is of a molecule that does not simply accelerate rebuilding but also modulates the inflammatory phase of repair — potentially resolving it faster.
It is worth distinguishing two different ways a molecule can be “anti-inflammatory,” because the distinction bears on how one should read the Tβ4 data. One mode is blunt immunosuppression — broadly shutting down immune activity, the way a corticosteroid does — which reduces inflammation but also impairs the very processes needed to fight infection and clear debris. The other mode is resolution: helping an inflammatory response complete its normal arc and transition into the rebuilding phase rather than smoldering indefinitely. The Tβ4 literature points more toward the second mode. In injury models, the peptide does not appear to abolish the inflammatory response but rather to temper excessive infiltration and steer the wound environment toward repair, in parallel with recruiting reparative cells and building new vasculature.27 If that reading is correct, it is a more physiologically attractive profile than crude suppression — but it is also harder to demonstrate with a simple biomarker, and it remains, again, a preclinical characterization rather than a human clinical one.
Three caveats keep this honest. First, essentially all of this mechanistic work is in cells and animals; the NF-κB and cytokine data are not human clinical outcomes. Second, most of it used full-length Tβ4, so whether the TB-500 heptapeptide reproduces the NF-κB inhibition is an open question rather than an established fact. Third, “reduces a cytokine in a dish” is several inferential steps removed from “reduces clinically meaningful inflammation in a person,” and those steps are exactly where many promising anti-inflammatory candidates fail. The mechanistic case for an anti-inflammatory effect is real and specific, but it is preclinical and largely parent-protein. Readers exploring how this compound is framed relative to inflammatory disease can compare the discussion in the site’s article on whether TB-500 is a promising therapy for chronic inflammatory conditions, which examines the same evidence gap from a clinical angle.
The Preclinical Recovery Evidence, Tissue by Tissue
When people say TB-500 “speeds recovery,” they are usually gesturing at a scattered but real body of animal and cell studies. Organizing it by tissue makes both the promise and the limits visible. The consistent theme is that thymosin beta-4 accelerates repair processes in multiple tissues in rodents; the consistent limitation is that these are preclinical models, mostly with the parent protein, with no human recovery trials to anchor them.
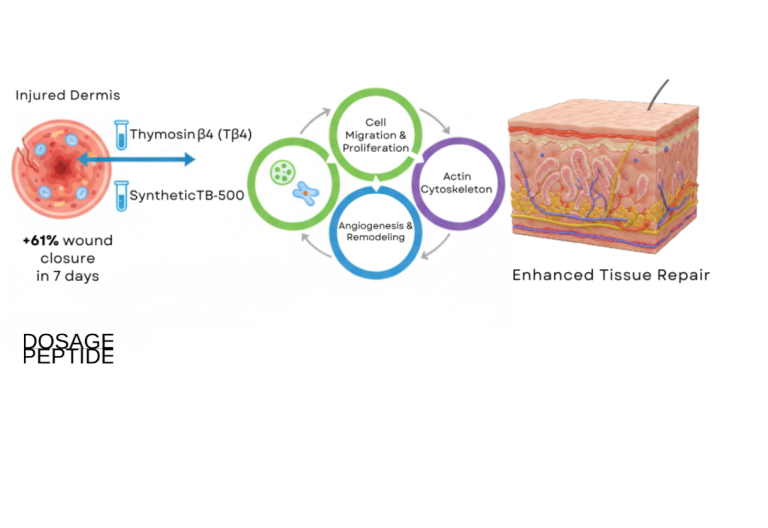
Skin and wound healing. This is the foundational evidence. In a classic study, Tβ4 applied topically or given intraperitoneally to rats increased wound re-epithelialization by roughly 42% at four days and up to 61% at seven days versus saline controls, with accelerated wound contraction, greater collagen deposition, and increased angiogenesis.4 The peptide also stimulated keratinocyte migration at strikingly low doses, consistent with the actin/migration mechanism. This wound-healing signal is the best-replicated Tβ4 finding across independent laboratories and animal species.
Cornea. The eye is where Tβ4 came closest to becoming a medicine. Preclinical corneal-injury models showed accelerated epithelial healing, and this translated into human ophthalmic trials (discussed below) — the only setting where the molecule has meaningful controlled human data.8
Heart. The cardiac literature is mechanistically rich. Tβ4 promoted cardiomyocyte and endothelial migration and survival, activated the ILK/Akt axis, and improved cardiac function after coronary ligation in mice; follow-up work described it as cardioprotective after myocardial infarction, reducing damage and subsequent fibrosis.17 This is compelling biology, but it is murine, and Tβ4’s cardiac-regeneration story has had its own controversies about reproducibility of the more dramatic regenerative claims.
Skeletal muscle. Directly relevant to athletic-recovery claims, injury to skeletal muscle induces local Tβ4 production, and Tβ4 acts as a chemoattractant for myoblasts — the muscle progenitor cells that rebuild damaged fibers — helping recruit them to the site of damage.11 In dystrophin-deficient (mdx) mice, chronic Tβ4 administration significantly increased the number of regenerating skeletal-muscle fibers compared with untreated animals, although the study did not demonstrate a corresponding improvement in measured muscle function.10 That dissociation — more regenerating fibers without a clear functional gain — is an important, sobering detail that recovery marketing omits.
Ligament. In a rat medial collateral ligament transection model, Tβ4 delivered in a fibrin sealant improved the mechanical properties of the healing ligament at four weeks relative to controls, suggesting a pro-repair effect in dense connective tissue.12 This is a single small animal study, but it is one of the few in a tissue directly relevant to the sprains and strains for which the compound is informally used.
The table below summarizes the preclinical recovery evidence and, crucially, flags which molecule was actually tested.
| Tissue / model | Reported effect | Molecule & system |
|---|---|---|
| Rat skin wounds | +42% to +61% re-epithelialization; more collagen, angiogenesis4 | Full-length Tβ4; rodent |
| Mouse myocardial infarction | ILK/Akt activation, myocyte survival, improved function, less fibrosis17 | Full-length Tβ4; rodent |
| Injured skeletal muscle | Chemoattracts myoblasts to damage site11 | Tβ4 (native + sulfoxide); mouse cells/tissue |
| mdx dystrophic mouse muscle | More regenerating fibers; no proven functional gain10 | Full-length Tβ4; rodent |
| Rat MCL ligament transection | Improved mechanical properties at 4 weeks12 | Full-length Tβ4 in fibrin; rodent |
| Cornea (preclinical + human) | Accelerated epithelial healing8 | Full-length Tβ4 (RGN-259) |
A recurring methodological point ties these tissue findings together and limits how far they travel. Almost all of these studies deliver Tβ4 locally or at doses scaled to a small rodent, over short observation windows, with structural or histological endpoints — re-epithelialization percentage, number of regenerating fibers, mechanical stiffness at four weeks. These are appropriate readouts for a proof-of-concept animal experiment, but they are not the endpoints that establish clinical recovery in humans: return to function, time to full activity, pain, re-injury rate, and durable outcomes measured over months. The leap from “more regenerating fibers in a mouse at four weeks” to “an athlete recovers faster from a hamstring strain” crosses species, dose scale, delivery route, endpoint type, and timescale all at once. Each of those is a place where preclinical promise routinely evaporates, which is why regulators require the human trials that, for TB-500 specifically, have not been done.
Two honest conclusions follow. First, there is a genuine, multi-tissue preclinical signal that thymosin beta-4 accelerates repair — this is not a fabricated reputation. Second, almost none of it is TB-500-the-fragment, none of it is human athletic-recovery data, and at least one directly relevant model (mdx muscle) showed structural regeneration without functional benefit. The gap between “Tβ4 accelerates re-epithelialization in a rat” and “TB-500 speeds recovery in an athlete” is wide, and it is filled with assumption, not evidence.
Where Are the Human Trials? Tβ4 Versus TB-500
This is the crux of the title’s question, and the answer requires splitting the molecule from its fragment one more time. Human clinical trials exist — but for full-length thymosin beta-4, in specific medical indications, and with results that are more instructive than they first appear.
The most advanced human program is ophthalmic. RGN-259, a 0.1% thymosin beta-4 ophthalmic solution, was tested in neurotrophic keratopathy in a randomized, placebo-controlled, double-masked Phase III trial. In that study, complete healing of persistent corneal epithelial defects occurred in 60% of Tβ4-treated subjects versus 12.5% on placebo at the four-week primary endpoint, with a durable difference two weeks after treatment stopped.8 That is a real, statistically meaningful human efficacy signal — for a topical eye formulation of the full 43-mer protein, in a specific ocular-surface disease. Importantly, the broader development picture is mixed: a separate European Phase III dry-eye trial (SEER-3) of the same agent missed its primary endpoint, reportedly because of an unusually strong placebo response, illustrating how fragile even a promising peptide signal can be in confirmatory trials.
The dermal program tells a similar “promising but unfinished” story. RGN-137, a topical Tβ4 gel, was evaluated in Phase II trials for chronic wounds — pressure ulcers and venous stasis ulcers — and a European randomized study reported acceptable safety and tolerability with signals of enhanced healing, but these were early-phase results that did not proceed to definitive Phase III approval.9 Cardiac and other applications have largely remained preclinical or exploratory.
It is worth pausing on why the human evidence is shaped this way — concentrated in topical eye and skin applications rather than in the systemic recovery uses that dominate the marketing. Part of the answer is regulatory practicality. A localized ophthalmic or dermal formulation targets an accessible tissue, delivers the peptide directly to the injury, keeps systemic exposure low, and can be studied with a clear, objective endpoint such as complete epithelial closure. A systemic injectable for “faster recovery” in otherwise healthy people is a far harder proposition: the endpoint is fuzzy, the population is not sick, the safety bar for dosing healthy individuals is high, and a mechanism that promotes angiogenesis and cell migration invites scrutiny about long-term risk. These are exactly the conditions under which sponsors pursue narrow, well-defined medical indications and avoid broad systemic claims — which is precisely the opposite of how TB-500 is positioned in the gray market. The mismatch between where the science went (focused, topical, disease-specific) and where the marketing goes (broad, injected, wellness-oriented) is itself a signal worth heeding.
Now the decisive point: none of this is TB-500 as sold to researchers and athletes, and none of it is systemic (injected) administration for musculoskeletal recovery or general anti-inflammatory use. The completed human trials used topical formulations of full-length Tβ4 for eye and skin disease. A 2026 scoping review that searched PubMed, Europe PMC, and ClinicalTrials.gov through early 2026 for Tβ4 and TB-500 in tissue healing and musculoskeletal repair reached the conclusion that anchors this entire article: the human clinical evidence base for TB-500 in these applications is essentially absent, with the literature dominated by preclinical work and the parent protein.13 In other words, for the specific claim in the title — that clinical studies show TB-500 speeds recovery and reduces inflammation — the correct answer is that such clinical studies do not exist. What exists is preclinical Tβ4 data plus narrow human trials of topical Tβ4 in ophthalmology and dermatology.
How TB-500 Compares With Related Repair Peptides
Placing TB-500 beside other compounds researchers encounter in the tissue-repair space clarifies where it stands. The most common comparison is with BPC-157, another peptide with a large rodent healing literature and a similar absence of rigorous human trials; the two are frequently discussed together and sometimes combined in informal protocols. The contrast with an approved biologic and with the parent protein is also instructive.
| Compound | Proposed mechanism | Human evidence status |
|---|---|---|
| TB-500 (Tβ4 fragment) | Actin sequestration, cell migration; anti-inflammatory (inferred from Tβ4) | No completed human recovery/inflammation trials13 |
| Thymosin β4 (full length, e.g. RGN-259) | Actin binding, ILK/Akt survival, VEGF angiogenesis, NF-κB inhibition | Phase III in neurotrophic keratopathy (topical); mixed dry-eye results; Phase II dermal ulcers89 |
| BPC-157 | Angiogenesis, growth-factor/nitric-oxide modulation (proposed) | Overwhelmingly rodent; no rigorous human efficacy trials |
| GHK-Cu | Copper delivery, matrix remodeling, wound signaling | Cosmetic/topical human data; no injury-recovery RCTs |
The pattern is clear. Full-length Tβ4 is the only member of this group with a genuine controlled human efficacy signal, and only in a narrow topical ophthalmic indication. TB-500 the fragment, BPC-157, and GHK-Cu all share the same fundamental status for recovery and inflammation: mechanistically interesting, supported by animal and cell studies, and unproven in humans for those uses. TB-500 is not an outlier here — it sits squarely in the “promising preclinical, unvalidated clinical” category, with the added complication that its identity as a fragment introduces uncertainty even about whether it reproduces the parent’s full activity. Readers weighing it against BPC-157 in particular may find the site’s overview of what BPC-157 is and how the healing-peptide claims are structured and the analysis of whether BPC-157 helps with inflammation and joint pain useful for calibrating expectations across the class.
There is a further lesson embedded in the comparison. Full-length Tβ4, the best-validated version of this biology, still could not convert a strong Phase III ophthalmic signal into an unambiguous multi-trial success, stumbling in a confirmatory dry-eye study. If the parent protein — better characterized, clinically formulated, and studied in dedicated trials — finds robust efficacy this hard to nail down, a loosely defined fragment used off-label for a completely different purpose has, realistically, an even steeper evidentiary hill to climb.
Dosing in a Research Context
Because there are no human efficacy trials, there is no established therapeutic dose for TB-500 in humans, and any figures quoted online derive from animal studies, veterinary practice, or anecdotal bodybuilding protocols rather than from controlled human pharmacology. This section is strictly educational context, not a usage recommendation, and the absence of validated human dosing is itself a key finding.
What the animal literature provides is dosing anchored to the model, not to a person. The mdx dystrophic-mouse study, for example, administered 150 micrograms of Tβ4 twice weekly over six months — a regimen designed for a laboratory mouse, in mass terms that do not translate directly to humans by simple scaling.10 Wound-healing studies used topical or intraperitoneal dosing in rats, again model-specific.4 The human ophthalmic trials used a fixed-concentration topical eye-drop formulation (0.1% Tβ4), a delivery route and exposure profile entirely different from the systemic subcutaneous injection typical of gray-market TB-500 use.8 None of these establishes a safe or effective injected dose for a human seeking faster recovery.
The informal “protocols” that circulate — typically expressed as milligram-per-week loading and maintenance schedules for reconstituted subcutaneous TB-500 — have no controlled-trial basis whatsoever. They are extrapolations, often traceable to forum culture rather than to any pharmacokinetic study of the fragment in humans. A researcher documenting handling parameters should treat any such number as an unvalidated convention, not a dose with an evidentiary foundation. The honest bottom line is that “how much TB-500 speeds recovery” cannot be answered because neither the efficacy nor the dose has been established in humans. The mechanics of how researchers convert vial contents to concentrations for benchtop work are covered generically in the site’s peptide reconstitution guide, which is written for educational reference rather than as human-dosing guidance.
Safety and Tolerability
Safety data for TB-500 specifically are thin, and this deserves the same candor as the efficacy question. What can be said is bounded and comes mostly from the parent protein.
In the human trials of full-length Tβ4 — the topical ophthalmic and dermal studies — the peptide was generally well tolerated over the studied durations, with safety profiles reported as acceptable and comparable to placebo.89 The European venous-ulcer study specifically noted acceptable safety and tolerability across the doses tested.9 This is genuinely reassuring for those particular formulations, routes, durations, and populations, but the qualifiers do heavy work. Several caveats temper any extrapolation to injected TB-500 in a healthy person seeking recovery:
- Molecule mismatch. The reassuring human safety data are for full-length Tβ4, not the TB-500 fragment. A different molecule can have a different safety and immunogenicity profile.
- Route mismatch. Human safety was established with topical (eye-drop, gel) delivery; systemic subcutaneous injection is a different exposure with different considerations, and it has not been characterized in controlled human trials.
- Duration. Trials ran weeks to a few months. Long-term, repeated systemic administration has no human safety characterization.
- Angiogenesis and cell migration are double-edged. A molecule whose mechanism is to promote new blood-vessel formation and cell migration raises a theoretical concern in any setting where those processes could be harmful — for example, an undiagnosed malignancy, where enhanced angiogenesis is undesirable. This is a mechanistic caution, not a demonstrated harm, but it is the kind of risk that only proper clinical study can resolve.
- Product quality. Because TB-500 is sold as a research chemical outside regulated manufacturing, real-world material varies in purity, identity, and endotoxin content. Contaminants and mislabeling are risks that have nothing to do with the peptide’s intrinsic pharmacology and everything to do with sourcing.
The reasonable reading is that thymosin beta-4, in the specific topical clinical settings studied, did not throw up major short-term safety signals — but that this provides limited assurance about injected TB-500 used chronically in healthy people, and none at all about efficacy. Absence of demonstrated harm in one context is not the same as demonstrated safety in another, and it is certainly not evidence of benefit.
Handling and Reconstitution in a Research Context
Because TB-500 is most often encountered as a lyophilized (freeze-dried) powder in a sealed vial, a brief, strictly educational note on laboratory handling is warranted — with the emphasis that this reflects standard research-peptide practice, not a usage recommendation, and that TB-500 is not an approved therapeutic for any indication.
Lyophilized peptides are generally reconstituted with sterile or bacteriostatic water for laboratory purposes. The diluent is directed slowly against the inside wall of the vial rather than sprayed onto the powder, and the vial is gently swirled rather than shaken, because vigorous agitation can shear peptide bonds and denature the material. The volume of diluent simply sets the concentration: a fixed mass of peptide dissolved in a larger volume yields a lower concentration per unit volume, which is the arithmetic behind any reconstitution chart. Beta-thymosin peptides are relatively soluble and stable, but the same general rules apply.
| Parameter | Typical research-context practice |
|---|---|
| Lyophilized storage | Cool, dark conditions; long-term stability favored by freezing |
| After reconstitution | Refrigerated; used within a limited window |
| Light and heat | Minimize exposure; both can degrade peptides |
| Agitation | Swirl gently; avoid shaking or foaming |
| Freeze-thaw | Repeated cycles degrade peptides; avoid |
| Sterility | Aseptic technique; bacteriostatic water for multi-use practice |
It bears repeating that meticulous handling changes nothing about the evidence question. A perfectly reconstituted, high-purity vial of TB-500 is still a compound with no human recovery-efficacy data. Good technique preserves whatever biological activity the molecule has; it does not create efficacy where none has been demonstrated. For the underlying vocabulary — terms such as lyophilization, sequestration, and re-epithelialization used throughout this article — the site’s peptide glossary offers plain-language definitions for educational reference.
Regulatory Status and the WADA Prohibition
TB-500’s regulatory picture is unambiguous in one respect and murky in another, and precision matters.
No therapeutic approval. TB-500 is not approved as a drug for recovery, inflammation, injury healing, or any other condition by the U.S. Food and Drug Administration, the European Medicines Agency, or any comparable major regulator. The compound is sold and used as a “research chemical,” a designation that carries no assurance of efficacy, safety, purity, or even identity. Even full-length thymosin beta-4, despite its more advanced clinical program, has not achieved marketing approval for the systemic regenerative uses often attributed to TB-500; its furthest-developed application remains an investigational topical ophthalmic product.8
Explicit prohibition in sport. This is the clearest regulatory fact about the compound and the one most relevant to its real-world user base. The World Anti-Doping Agency added thymosin-β4 and its derivatives — naming TB-500 explicitly as an example — to the Prohibited List under section S2.3, covering growth factors and growth-factor modulators that affect muscle, tendon, or ligament protein synthesis, vascularization, energy utilization, regenerative capacity, or fiber-type switching.14 It is prohibited at all times, both in and out of competition, and is classified as a non-specified substance, which carries the more serious sanction category. Anti-doping laboratories have developed methods to detect TB-500 and its metabolites in urine and plasma. For any athlete subject to WADA-compliant testing, use of TB-500 constitutes an anti-doping rule violation regardless of the state of the efficacy evidence — a point worth underscoring precisely because the compound is marketed to the recovery-seeking athletic audience most exposed to that risk.
A recurring source of confusion deserves explicit correction. The existence of human clinical trials for thymosin beta-4 is sometimes cited as though it confers legitimacy on TB-500 for recovery. It does not. Being studied in a Phase II or III trial for a specific indication (corneal or dermal wounds) is not the same as being approved, and it is certainly not approval of a different molecule (the fragment) for a different purpose (systemic athletic recovery) by a different route (injection). Conflating “thymosin beta-4 was in clinical trials” with “TB-500 is a validated recovery therapy” is one of the most common errors in the marketing literature, and readers should be alert to it whenever they see confident efficacy language resting on a trial citation for the parent protein.
The regulatory synthesis is straightforward: TB-500 is an unapproved research peptide, its parent protein has narrow investigational human data but no approval for the uses TB-500 is sold for, and TB-500 is explicitly banned in sport. For any legitimate exploration of this biology, the appropriate path is formal preclinical and clinical investigation under regulatory oversight, not off-label or informal use. Those tracking how the class evolves may follow related coverage such as the analysis of whether TB-500 could support regeneration in spinal-cord injury, another area where preclinical promise has not yet met human proof.
Frequently Asked Questions
Do clinical studies show that TB-500 speeds recovery?
No. There are no completed human randomized controlled trials of TB-500 — the synthetic thymosin beta-4 fragment — for athletic recovery, injury healing, or general tissue repair. A 2026 scoping review searching the major trial and literature databases concluded that the human clinical evidence base for TB-500 in tissue healing and musculoskeletal repair is essentially absent, dominated instead by preclinical animal and cell studies.13 The recovery reputation rests on rodent experiments — accelerated wound re-epithelialization, myoblast recruitment, ligament repair — performed mostly with full-length thymosin beta-4, not the fragment sold as TB-500.411
Does TB-500 reduce inflammation, and is that proven in humans?
There is a real mechanistic case for an anti-inflammatory effect, but it is preclinical. Thymosin beta-4 inhibited TNF-α–induced NF-κB activation and suppressed IL-8 expression in corneal epithelial cells, and it reduced inflammatory cell infiltration in cardiac injury models.67 These are cell-culture and animal findings, largely with the parent protein. No human clinical trial has demonstrated that TB-500 reduces clinically meaningful inflammation, so the honest answer is: mechanistically plausible, preclinically supported, clinically unproven.
Is TB-500 the same thing as thymosin beta-4?
No, and this is the most important distinction. Thymosin beta-4 is a natural 43-amino-acid protein. TB-500 is a synthetic fragment built around its central actin-binding motif (the LKKTETQ sequence, roughly residues 17–23).14 Most published healing and cardiac studies used the full-length protein, not the fragment. Whether TB-500 reproduces the entire activity profile of Tβ4 — including its anti-inflammatory and angiogenic signaling, some of which maps to regions outside the central motif — is an open question, not an established fact.3
Have any thymosin beta-4 products been tested in humans?
Yes, but for specific medical indications and mostly by topical delivery. A 0.1% thymosin beta-4 eye solution (RGN-259) showed complete corneal healing in 60% of treated patients versus 12.5% on placebo in a Phase III neurotrophic-keratopathy trial, though a separate European dry-eye Phase III study missed its endpoint.8 A topical Tβ4 gel (RGN-137) reached Phase II for chronic skin ulcers with acceptable safety and healing signals.9 None of these tested injected TB-500 for athletic recovery.
What is the actual mechanism of TB-500?
Its core function is actin sequestration: it binds monomeric G-actin roughly 1:1 and buffers the cellular pool of actin available for polymerization, which facilitates the cell migration central to tissue repair.3 Thymosin beta-4 additionally activates the ILK/Akt cell-survival pathway and promotes VEGF-driven angiogenesis, and it can dampen NF-κB–driven inflammation.156 The fragment is expected to retain the actin/migration function; whether it retains the rest is less certain.
Is TB-500 legal, and is it banned in sport?
TB-500 is not an approved drug anywhere; it is sold as an unregulated research chemical. It is explicitly prohibited in sport by the World Anti-Doping Agency, which lists thymosin-β4 and its derivatives (naming TB-500) under section S2.3 as prohibited growth factors, banned at all times in and out of competition.14 Detection methods for TB-500 and its metabolites exist. For any tested athlete, use is an anti-doping rule violation.
How does TB-500 compare to BPC-157 for recovery?
They occupy the same evidence tier. Both have substantial rodent healing literatures and no rigorous human efficacy trials for injury recovery. TB-500’s biology centers on actin/migration and (via the parent protein) angiogenesis and anti-inflammatory signaling; BPC-157’s proposed mechanisms center on angiogenesis and growth-factor/nitric-oxide modulation. Neither is proven in humans for recovery, and both are best regarded as investigational research compounds rather than validated therapies.13
Does more regenerating tissue mean better function?
Not necessarily, and TB-500 illustrates the point. In dystrophic mdx mice, chronic thymosin beta-4 increased the number of regenerating muscle fibers but did not produce a clear improvement in measured muscle function.10 This dissociation — more repair activity at the tissue level without a matching functional gain — is common in regenerative research and is exactly why structural findings in animals cannot be assumed to translate into faster, better recovery in people.
Is there a safe, established dose of TB-500 for recovery?
No. Because no human efficacy trials exist, there is no validated human dose. Figures circulating online are extrapolations from animal studies (which used model-specific dosing such as 150 micrograms twice weekly in mice) or from forum anecdote, not from human pharmacology.10 The human trials that do exist used topical Tβ4 formulations at fixed concentrations, not injected fragment doses, so they provide no basis for a recovery-dosing regimen.8
References
- Bock-Marquette I, Saxena A, White MD, DiMaio JM, Srivastava D. Thymosin beta4 activates integrin-linked kinase and promotes cardiac cell migration, survival and cardiac repair. Nature. 2004;432(7016):466-472. PMID: 15565145. https://pubmed.ncbi.nlm.nih.gov/15565145/
- Goldstein AL, Hannappel E, Sosne G, Kleinman HK. Thymosin β4: a multi-functional regenerative peptide. Basic properties and clinical applications. Expert Opin Biol Ther. 2012;12(1):37-51. PMID: 22074294. https://pubmed.ncbi.nlm.nih.gov/22074294/
- Goldstein AL, Hannappel E, Kleinman HK. Thymosin beta4: actin-sequestering protein moonlights to repair injured tissues. Trends Mol Med. 2005;11(9):421-429. PMID: 16099219. https://pubmed.ncbi.nlm.nih.gov/16099219/
- Malinda KM, Sidhu GS, Mani H, et al. Thymosin beta4 accelerates wound healing. J Invest Dermatol. 1999;113(3):364-368. PMID: 10469335. https://pubmed.ncbi.nlm.nih.gov/10469335/
- Philp D, Kleinman HK. Animal studies with thymosin beta4, a multifunctional tissue repair and regeneration peptide. Ann N Y Acad Sci. 2010;1194:81-86. PMID: 20536453. https://pubmed.ncbi.nlm.nih.gov/20536453/
- Qiu P, Kurpakus-Wheater M, Sosne G. Thymosin β4 inhibits TNF-α-induced NF-κB activation, IL-8 expression, and the sensitizing effects by its partners PINCH-1 and ILK. FASEB J. 2011;25(6):1815-1826. PMID: 21343177. https://pubmed.ncbi.nlm.nih.gov/21343177/
- Srivastava D, Saxena A, DiMaio JM, Bock-Marquette I. Thymosin beta4 is cardioprotective after myocardial infarction. Ann N Y Acad Sci. 2007;1112:161-170. PMID: 17600280. https://pubmed.ncbi.nlm.nih.gov/17600280/
- Sosne G, Kleinman HK, Springs C, et al. 0.1% RGN-259 (Thymosin β4) Ophthalmic Solution Promotes Healing and Improves Comfort in Neurotrophic Keratopathy Patients in a Randomized, Placebo-Controlled, Double-Masked Phase III Clinical Trial. Int J Mol Sci. 2022;24(1):554. PMID: 36613994. https://pubmed.ncbi.nlm.nih.gov/36613994/
- Guarnera G, De Rosa A, Camerini R. Thymosin beta-4 and venous ulcers: clinical remarks on a European prospective, randomized study on safety, tolerability, and enhancement on healing. Ann N Y Acad Sci. 2007;1112:407-412. PMID: 17495250. https://pubmed.ncbi.nlm.nih.gov/17495250/
- Spurney CF, Cha HJ, Sali A, et al. Evaluation of skeletal and cardiac muscle function after chronic administration of thymosin β-4 in the dystrophin deficient mouse. PLoS One. 2010;5(1):e8976. PMID: 20126456. https://pubmed.ncbi.nlm.nih.gov/20126456/
- Tokura Y, Nakayama Y, Fukada S, et al. Muscle injury-induced thymosin β4 acts as a chemoattractant for myoblasts. J Biochem. 2011;149(1):43-48. PMID: 21186187. https://pubmed.ncbi.nlm.nih.gov/21186187/
- Xu B, Yang M, Li Z, et al. Thymosin β4 enhances the healing of medial collateral ligament injury in rat. Regul Pept. 2013;184:1-5. PMID: 23523891. https://pubmed.ncbi.nlm.nih.gov/23523891/
- McGuire F, Hughes E, Maak T, Cushman DM. Thymosin Beta-4 and TB-500 in Tissue Healing, Regeneration, and Musculoskeletal Repair: A Scoping Review. Appl Sci. 2026;16(12):6202. doi:10.3390/app16126202. https://www.mdpi.com/2076-3417/16/12/6202
- World Anti-Doping Agency. The Prohibited List (Section S2.3, Growth Factors and Growth Factor Modulators — thymosin-β4 and its derivatives, e.g. TB-500). https://www.wada-ama.org/en/prohibited-list
Educational and research-use disclaimer: This article is provided solely for scientific and educational purposes. TB-500 is a synthetic fragment of thymosin beta-4 and is not approved by the FDA, EMA, or any comparable regulator for the treatment, cure, or prevention of injury, inflammation, or any other disease, and no human clinical trials have demonstrated that it speeds recovery or reduces inflammation. The regenerative and anti-inflammatory data discussed here are predominantly preclinical (cell and animal) and were largely generated with full-length thymosin beta-4 rather than the TB-500 fragment. TB-500 is explicitly prohibited in sport by the World Anti-Doping Agency. Nothing here is medical advice or a recommendation for human use. Any legitimate investigation of this compound should occur within properly authorized preclinical or clinical research under appropriate oversight. Readers should consult qualified professionals and applicable regulations before making any decisions.