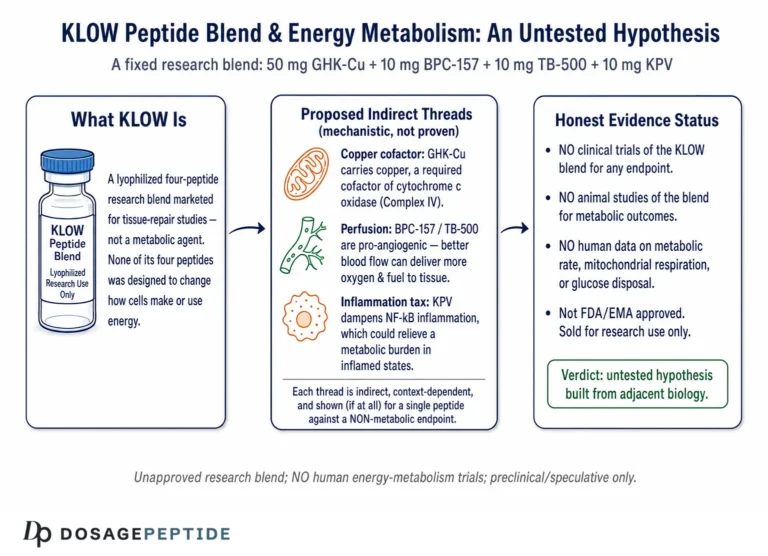
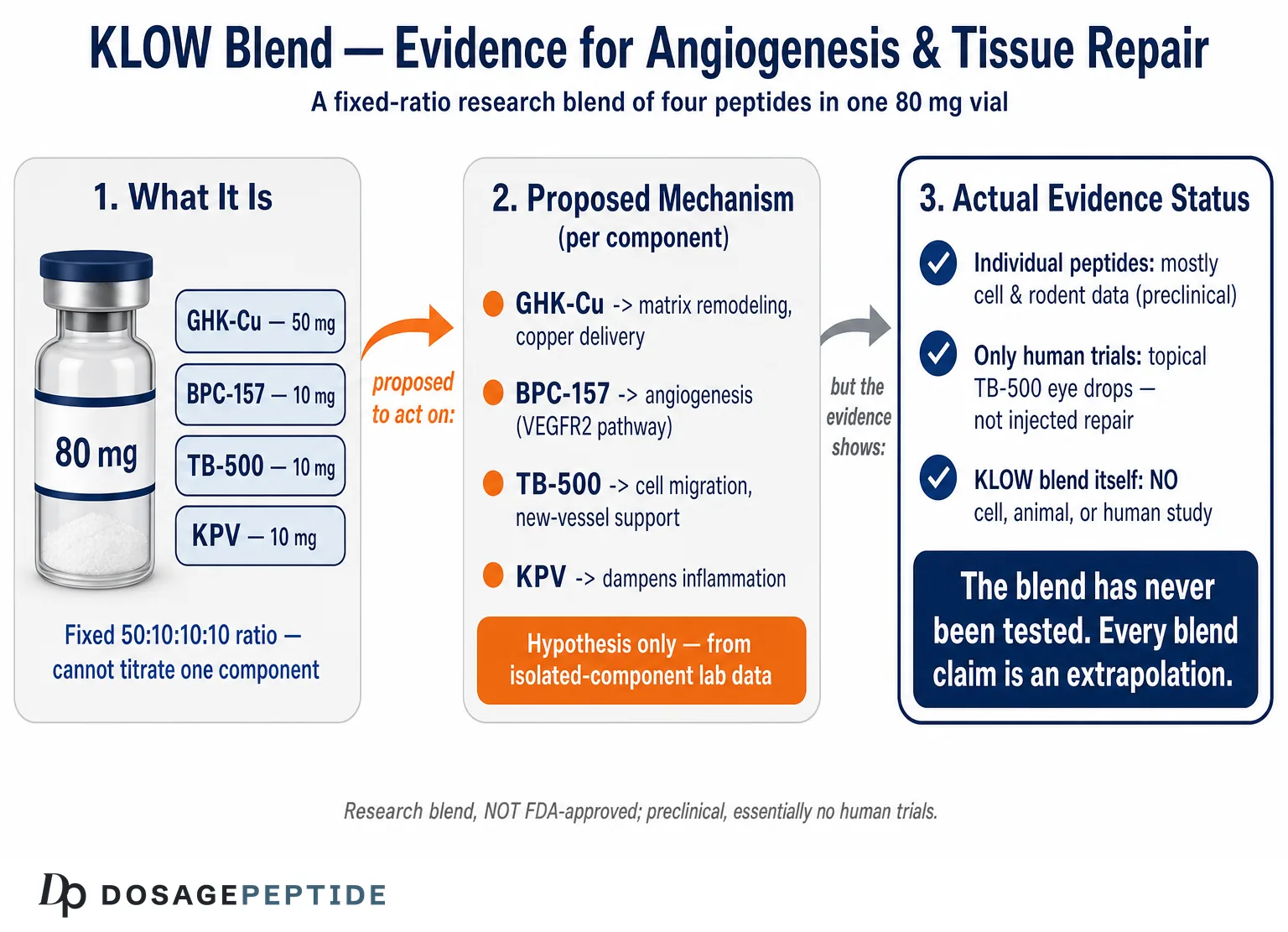
KLOW is a fixed-ratio research blend that packs four separate peptides into a single 80 mg vial: GHK-Cu (50 mg), BPC-157 (10 mg), TB-500 (10 mg), and KPV (10 mg). Each of those four molecules has, on its own, a body of preclinical literature touching on angiogenesis (the growth of new blood vessels) and tissue repair, and vendors frequently market the combination as a convenience “recovery stack.” The question posed in this article’s title — what evidence supports KLOW in angiogenesis and tissue repair — deserves a direct and honest answer before anything else: there is no published human trial, and no published animal study, that has tested the KLOW blend itself. The evidence that exists is entirely about the individual components, mostly in cell cultures and rodents, and it cannot be transferred wholesale to a four-peptide mixture that no one has formally studied.
That framing matters. A title like this can imply that KLOW is an established angiogenic or regenerative therapy whose supporting evidence merely needs summarizing. It is not. KLOW is an unapproved combination of research chemicals, none of which is an FDA-approved drug for tissue repair, and the specific blend has never been validated in any controlled experiment.1 So the accurate way to read the question is as an open research question: given what is known about GHK-Cu, BPC-157, TB-500, and KPV individually, what mechanistic and preclinical signals might plausibly bear on angiogenesis and tissue repair, and how large is the gap between those signals and anything resembling proof in humans?
This page walks through that evidence component by component — what each peptide is, how it is proposed to act, the actual level of evidence (cell, animal, or human), how the four compare, the research models used, safety and handling considerations in a laboratory context, and the substantial limitations and regulatory realities. It is written for an educational and research audience only. Nothing here is medical advice, a protocol, or a suggestion that KLOW treats, cures, or prevents any condition.
What KLOW Is and Where Its Four Components Come From
KLOW is not a single molecule but an acronym-style trade name for a co-formulated blend. The most commonly sold version, and the one described on DosagePeptide’s own reference pages (manufacturer specification), contains GHK-Cu 50 mg, BPC-157 10 mg, TB-500 10 mg, and KPV 10 mg in one 80 mg vial.1 Because all four peptides share a single container, they are reconstituted and drawn together, and their ratio is fixed by the manufacturer — a researcher cannot titrate one component without changing the others. That design choice is central to understanding the evidence gap discussed later: even if each peptide were perfectly characterized alone, a fixed 5:1:1:1 mixture introduces variables (relative dose, potential physical or chemical interaction in solution, differing pharmacokinetics) that no published study addresses.
The four constituents come from very different biological origins:
| Component | Chemical class | Biological origin | Amount in 80 mg KLOW vial |
|---|---|---|---|
| GHK-Cu | Copper-bound tripeptide (glycyl-L-histidyl-L-lysine + Cu2+) | Isolated from human plasma by Loren Pickart in 1973; declines with age | 50 mg |
| BPC-157 | Synthetic pentadecapeptide (15 amino acids) | Partial sequence derived from a protein in human gastric juice | 10 mg |
| TB-500 | Peptide fragment of thymosin beta-4 (a 43-amino-acid protein) | Synthetic version of a segment of a near-ubiquitous cellular actin-binding protein | 10 mg |
| KPV | Tripeptide (lysine-proline-valine) | C-terminal fragment of alpha-melanocyte-stimulating hormone (alpha-MSH) | 10 mg |
GHK-Cu is the oldest and most studied of the four. The tripeptide glycyl-L-histidyl-L-lysine was first identified in human plasma in 1973 and shown to bind copper(II) with high affinity. Pickart and Margolina’s 2018 review in the International Journal of Molecular Sciences consolidated decades of work and analyzed gene-expression data suggesting GHK-Cu can influence the expression of a large fraction of human genes, many tied to tissue remodeling, antioxidant response, and DNA repair.2 Its plasma concentration falls with age, which is one reason it has been framed as a “reset” signal for repair pathways.
BPC-157 (“body protection compound”) is a synthetic pentadecapeptide whose sequence corresponds to a portion of a protein found in gastric juice. It has no natural free-standing existence; it is a designed research peptide. The bulk of its literature is Croatian preclinical work centered on the gastrointestinal tract, tendon, muscle, and vascular models.3,4
TB-500 is a synthetic peptide marketed as thymosin beta-4 (Tbeta4), although commercial “TB-500” is often the acetylated active fragment rather than the full 43-amino-acid protein. Thymosin beta-4 is one of the most abundant intracellular actin-sequestering proteins in mammalian cells and is released at sites of injury.7,8
KPV is the C-terminal three amino acids of alpha-MSH, a hormone with well-documented anti-inflammatory activity. KPV retains a substantial part of alpha-MSH’s anti-inflammatory effect while lacking the pigmentary (melanocyte-stimulating) activity of the parent hormone, which is why it is studied as an inflammation-modulating tool rather than a pigmentation agent.9
The marketing logic of KLOW is that these four cover complementary territory: GHK-Cu for extracellular-matrix remodeling and copper delivery, BPC-157 for angiogenesis and blood flow, TB-500 for cell migration and actin dynamics, and KPV for damping inflammation. That is a plausible hypothesis about synergy. It is not a demonstrated fact, and the leap from “four peptides with individually interesting mechanisms” to “an effective combined therapy” is exactly the leap the evidence does not support. Readers wanting the formulation specifics can consult the KLOW 80 mg vial reference page and the broader KLOW reconstitution and handling guide, both of which stress the research-only status of the blend.
Proposed Molecular Mechanisms in Angiogenesis and Repair
Angiogenesis and tissue repair are not single events but coordinated programs: endothelial cells must be activated, migrate, proliferate, and form tubes; the extracellular matrix must be degraded and rebuilt; fibroblasts and progenitor cells must be recruited; and inflammation must resolve on schedule. Each KLOW component is proposed to touch a different node of that program. Understanding the proposed mechanisms — and marking clearly where they are established versus speculative — is the core of evaluating the blend honestly.
GHK-Cu — matrix remodeling and copper-dependent angiogenesis. Copper is a mandatory cofactor for enzymes involved in angiogenesis and for lysyl oxidase, which cross-links collagen and elastin. GHK-Cu is proposed to act as a copper-delivery vehicle and as a transcriptional modulator. In irradiated human dermal fibroblasts, GHK-Cu has been reported to upregulate vascular endothelial growth factor (VEGF) and basic fibroblast growth factor (bFGF), both pro-angiogenic signals.2 In human umbilical vein endothelial cell (HUVEC) studies, GHK-Cu formulations increased endothelial proliferation and raised expression of VEGF, FGF-2, and cell-cycle drivers such as cyclin D1.2,15 The 2018 gene-expression review frames GHK-Cu as a broad, pleiotropic modulator rather than a single-target growth-factor mimic.2 The caveat: much of this is in vitro or in constructed matrix models, and gene-expression breadth is not the same as clinical benefit.
BPC-157 — the VEGFR2-Akt-eNOS axis. The most concrete angiogenic mechanism among the four comes from Hsieh and colleagues (2017, Journal of Molecular Medicine). Using human endothelial cells, they showed BPC-157 increased both messenger RNA and protein expression of vascular endothelial growth factor receptor 2 (VEGFR2) — notably without raising VEGF-A itself — and promoted VEGFR2 internalization, which activates downstream signaling through the Akt-eNOS pathway, increasing nitric oxide production.3 In the chick chorioallantoic membrane assay, BPC-157 raised vessel density, and in rats with hind-limb ischemia it accelerated blood-flow recovery and increased vessel counts in ischemic muscle.3 Separate work links BPC-157 to the nitric-oxide system more broadly, affecting vascular tone via a Src-caveolin-1-eNOS pathway.5 These are coherent, mechanistically specific findings — but they are in cells and rodents.
TB-500 / thymosin beta-4 — actin sequestration and endothelial migration. Thymosin beta-4’s defining molecular function is G-actin sequestration: it binds monomeric actin and maintains a pool from which filaments can rapidly assemble, enabling the cytoskeletal reorganization that cell migration requires. Downstream of that, thymosin beta-4 has been reported to promote endothelial cell migration, tube formation, and endothelial progenitor cell recruitment, and to upregulate VEGF in a way that supports angiogenic sprouting.7,8 It also accelerates re-epithelialization in dermal wound models.8 One important nuance for KLOW: commercial “TB-500” is typically a fragment, and whether a fragment fully reproduces the intact protein’s angiogenic behavior is itself an open question.7
KPV — inflammation resolution, not direct angiogenesis. KPV’s role is different in kind. It is not primarily an angiogenic peptide; it is an anti-inflammatory one. Dalmasso and colleagues (2008, Gastroenterology) showed that KPV is taken up into intestinal epithelial and immune cells via the PepT1 transporter, where it inhibits NF-kappaB and MAP-kinase signaling, reducing pro-inflammatory cytokine production.9 Because unresolved inflammation impairs repair, a peptide that damps NF-kappaB could in theory create a more favorable environment for tissue healing — but that is an inference about context, not a demonstration that KPV drives repair or vessel growth.
Why the interaction question is not academic. It is tempting to treat “four complementary mechanisms” as though the effects simply add up, but pharmacology rarely works that way, and the specific chemistry of KLOW makes the assumption especially fragile. GHK-Cu carries a copper(II) ion, and copper is a redox-active metal that can, under some conditions, catalyze oxidative reactions. When a copper-bearing peptide shares a vial with three other peptides, the possibility of copper interacting with the other molecules — or of the other peptides competing for copper — is a real chemistry question that no published work on KLOW has examined. Similarly, the four peptides have very different sizes and presumably very different clearance rates: KPV is a tripeptide that is cleared and metabolized quickly, whereas the larger BPC-157 and thymosin beta-4 fragment behave differently. A fixed-ratio blend delivers all four at once, but their concentration-time curves after administration would diverge, meaning the “synergy” imagined at the moment of injection may not exist an hour later. These are not exotic objections; they are the standard questions any regulator or pharmacologist would ask of a combination product, and for KLOW they are simply unanswered.2
The nitric oxide theme. One thread worth highlighting is that two of the four components — BPC-157 and, indirectly, thymosin beta-4 via VEGF signaling — converge on nitric oxide and VEGF-related pathways.3,7 On one reading, that convergence could mean redundancy (two peptides pushing the same lever) rather than complementarity. On another, it could mean the blend leans heavily on a single mechanistic axis (VEGFR2/eNOS/NO) while GHK-Cu and KPV address matrix and inflammation. Either interpretation is speculative, but the point stands: mechanistic overlap between components complicates the simple “four different jobs” narrative, and only a direct study of the blend could resolve whether the components reinforce, duplicate, or interfere with one another.
Put together, the mechanistic story KLOW vendors tell is internally logical: matrix remodeling (GHK-Cu) plus new vessels (BPC-157, TB-500) plus cell migration (TB-500) plus reduced inflammation (KPV). But each arrow in that diagram rests on isolated-component data, and combining four active molecules can produce interactions — competitive, additive, or antagonistic — that single-peptide experiments cannot predict. The mechanism section is where KLOW looks most attractive on paper and where the absence of blend-specific data is most consequential.
The Actual Level of Evidence: An Honest Accounting
The single most important thing a reader can take from this article is a clear-eyed picture of what kind of evidence exists. Scientific evidence sits on a hierarchy, from mechanistic cell-culture work at the bottom, through animal studies, small human trials, and up to large randomized controlled trials and meta-analyses at the top. Where does each KLOW component sit, and where does the blend sit?
| Compound | Highest evidence level for repair/angiogenesis | Human data? | Blend (KLOW) data? |
|---|---|---|---|
| GHK-Cu | In vitro + rodent wound models; topical cosmetic use in humans | Human data mostly topical/cosmetic skin endpoints, not injected systemic repair | None |
| BPC-157 | Extensive rodent + in vitro; no completed published RCTs | Essentially none published for tissue repair | None |
| TB-500 / Tbeta4 | Rodent wound/cardiac models + human ophthalmic trials of thymosin beta-4 | Yes, but for eye-surface disease (topical), not injected systemic repair | None |
| KPV | Rodent colitis + in vitro; anti-inflammatory focus | None established for repair/angiogenesis | None |
| KLOW blend | None — no published study of the combination in any model | No | — |
The bottom row is the headline. Whatever one thinks of the individual peptides, KLOW as a formulation has zero direct evidence. There is no cell study, no animal study, and no human trial of the 50:10:10:10 mixture. Every claim made about the blend is an extrapolation from component data, and extrapolation across a combined formulation is one of the weakest forms of inference.
Looking at the components: GHK-Cu has the deepest and oldest literature, but the strongest human evidence is for topical cosmetic endpoints — skin firmness, appearance, wound-adjacent measures — not for injected systemic angiogenesis.2 BPC-157 has a large and mechanistically rich rodent literature, and a 2025 narrative review in Current Reviews in Musculoskeletal Medicine catalogs its musculoskeletal-healing signals, but that same review emphasizes the near-total absence of completed, peer-reviewed human trials and the resulting uncertainty.14 TB-500 / thymosin beta-4 is the only component with genuine controlled human trial data — but that data is for a topical ophthalmic formulation (RGN-259) in dry-eye and neurotrophic keratopathy, not for injectable systemic tissue repair. In a phase 2 dry-eye trial, thymosin beta-4 eye drops reduced ocular discomfort and corneal staining versus vehicle,10 and in a phase 3 neurotrophic keratopathy trial (SEER-1), complete corneal healing occurred in 6 of 10 treated versus 1 of 8 placebo subjects — but that primary endpoint did not reach statistical significance (p ≈ 0.066 by Fisher’s exact test), and the trial was terminated early with only 18 patients analyzed, so the numbers should not be over-read as demonstrated efficacy.11 A dermal-wound program in venous stasis ulcers reached early-phase trials but did not advance to approval.12 Those are real human results — for the eye surface, with a specific topical drug candidate, not for KLOW. KPV has rodent colitis data and in-vitro mechanism, and no established human repair or angiogenesis evidence.9
So the honest summary is: the KLOW components range from “well-studied topical cosmetic ingredient” (GHK-Cu) to “mechanistically interesting rodent peptide with no human repair trials” (BPC-157, KPV) to “peptide whose parent protein has real but eye-surface-specific human data” (TB-500). None of that adds up to evidence for the blend, and none of it demonstrates that KLOW promotes angiogenesis or tissue repair in a living human. The appropriate confidence level is “preclinical and hypothesis-generating,” full stop. Anyone presenting KLOW as a proven regenerative therapy is overstating the science by a wide margin. For context on how researchers think about stacking these peptides at all, DosagePeptide’s peptide stacks overview discusses the rationale and the uncertainty side by side.
How the Components Compare to Each Other and to Alternatives
Because KLOW’s appeal rests on the idea that its four peptides are complementary, it is worth comparing them directly — and comparing the blend to simpler, better-characterized combinations. The comparison also clarifies why a “more is better” formulation is not automatically superior.
Angiogenic strength (proposed). On mechanistic grounds, BPC-157 has the most specific angiogenic pathway data (VEGFR2-Akt-eNOS),3 and thymosin beta-4 has strong endothelial-migration and progenitor-recruitment data.7,8 GHK-Cu’s angiogenic contribution is more indirect — via copper-dependent enzymes and growth-factor upregulation in fibroblasts.2,15 KPV contributes little or nothing directly to angiogenesis; its value in the blend is proposed to be anti-inflammatory context.9 If angiogenesis were the sole target, KPV would arguably be the least justified inclusion on mechanistic grounds.
Matrix and structural repair. Here GHK-Cu leads, given its documented effects on collagen, elastin, and matrix-remodeling enzymes, followed by TB-500’s role in cell migration and BPC-157’s tendon/muscle signals.1,4,6 KPV again sits to the side.
| Property | GHK-Cu | BPC-157 | TB-500 | KPV |
|---|---|---|---|---|
| Primary proposed role | Matrix remodeling, copper delivery | Angiogenesis, cytoprotection | Cell migration, actin dynamics | Anti-inflammatory |
| Direct angiogenic pathway | Indirect (VEGF/FGF upregulation) | Direct (VEGFR2-Akt-eNOS) | Endothelial migration + VEGF | Minimal/none |
| Best human evidence | Topical cosmetic skin | None published (repair) | Topical ophthalmic (Tbeta4) | None (repair) |
| Depth of literature | Deep (since 1973) | Moderate, mostly one group | Moderate | Shallow |
Comparison to simpler blends. The most common two-peptide combination in this space is BPC-157 + TB-500, often marketed as a “recovery” pairing because it joins BPC-157’s angiogenic/cytoprotective signals with TB-500’s migration/actin effects. That two-peptide logic is easier to reason about than KLOW’s four-way mixture, and DosagePeptide covers it in the BPC-157 + TB-500 recovery blend explainer. Another related product, “Tri-Heal,” swaps GHK-Cu out and instead combines TB-500, BPC-157, and KPV at different ratios; see the Tri-Heal reference page for how the same peptides get recombined in different proportions. The existence of multiple overlapping blends underscores a key point: these formulations are commercial constructs, not clinically optimized regimens. No head-to-head study has ever compared KLOW to BPC-157 + TB-500, to Tri-Heal, or to any single component, so claims that the four-peptide version is “more effective” are entirely unsupported.
Why more components is not automatically better. There is a persistent intuition in the peptide market that a longer ingredient list signals a more powerful product. The opposite can be true. Every additional active molecule adds a variable, a potential interaction, a possible impurity, and another unknown to the safety picture — while the incremental benefit, if any, is unmeasured. In regulated drug development, combination products face a higher evidentiary bar precisely because regulators require proof that each component contributes and that the combination is safe together; combinations are not approved simply because each ingredient has some standalone rationale. KLOW inverts that logic: it assembles four peptides on the strength of individual mechanistic stories and asks the buyer to assume the assembly works. From an evidence standpoint, a well-characterized single peptide with human data would be preferable to a four-peptide blend with none, even though the blend “does more” on paper. The number of components is a marketing feature, not an evidentiary one.
Ratio matters, and the ratio is arbitrary. KLOW fixes GHK-Cu at five times the dose of each other peptide (50:10:10:10). Where does that ratio come from? Not from any comparative study — there is none. It appears to reflect the fact that GHK-Cu is typically used at higher masses than the others in standalone contexts, plus the convenience of round numbers that sum to 80 mg. A different vendor could just as defensibly sell a 20:20:20:20 blend, and nothing in the literature would adjudicate between them. This arbitrariness is a useful tell: when a formulation’s ratios are set by convenience rather than by dose-response data, it is a strong signal that the product is a commercial construct rather than an optimized therapeutic.
Approved alternatives. It is also worth naming the honest comparator: for genuine tissue-repair indications, approved options exist — recombinant PDGF (becaplermin) for diabetic foot ulcers, negative-pressure wound therapy, and standard surgical and physiotherapy approaches — all of which have controlled human evidence that KLOW lacks entirely. A fair comparison does not pit KLOW against nothing; it pits KLOW’s preclinical component data against interventions that have actually been tested in people. On that scale, KLOW is not a competitor to established care; it is an unproven research mixture.
Research Models and Methodology Behind the Evidence
Evaluating the KLOW evidence requires understanding how the underlying studies were done, because the model dictates how far a finding can be trusted. The component literature spans several methodologies, each with characteristic strengths and blind spots.
In vitro (cell-culture) models. Much of the mechanistic angiogenesis data — BPC-157’s VEGFR2 upregulation, GHK-Cu’s endothelial proliferation, thymosin beta-4’s migration assays — comes from cultured cells, frequently HUVECs (human umbilical vein endothelial cells).2,3,7 Standard readouts include scratch/wound-closure assays (measuring migration), tube-formation assays on Matrigel (measuring capillary-like organization), and Western blots or qPCR for signaling proteins and receptors. These experiments are powerful for isolating mechanism but say nothing about dosing, delivery, degradation, or whole-organism effects. A peptide that doubles endothelial migration in a dish may never reach relevant tissue concentrations after injection.
Ex vivo and embryonic assays. The chick chorioallantoic membrane (CAM) assay and aortic-ring assays bridge cell culture and live animals; BPC-157’s vessel-density increase was shown in the CAM model.3 These add tissue architecture but remain far from a human injury.
Rodent injury models. This is where BPC-157, thymosin beta-4, and KPV have their richest data. Typical designs include rat Achilles or quadriceps transection (tendon/muscle healing), hind-limb ischemia (angiogenesis and blood-flow recovery), full-thickness or incisional dermal wounds, and chemically induced (DSS or TNBS) colitis for KPV.3,4,6,8,9 Outcomes are measured as histological vessel counts, tensile strength, re-epithelialization percentage, laser-Doppler perfusion, or colitis severity scores. Rodent models are essential and informative, but they are also where translation most often fails: rodents heal differently from humans, doses are frequently high relative to body weight, blinding and randomization are inconsistently reported, and much BPC-157 work originates from a small number of affiliated laboratories, which raises independent-replication concerns.14
Human trials. The only rigorous human data among the components is for thymosin beta-4 as a topical ophthalmic agent (RGN-259). Those were randomized, placebo-controlled, double-masked trials — the gold-standard design — measuring corneal fluorescein staining, symptom scores, and complete-healing rates in dry-eye and neurotrophic keratopathy.10,11 A venous-stasis-ulcer program (registered on ClinicalTrials.gov as NCT00832091) reached early-phase testing.12 These are methodologically sound, but they test a specific topical drug for eye-surface or dermal-ulcer disease, not an injected four-peptide blend for general repair. There is no registered or published trial of KLOW.
Gene-expression / systems approaches. GHK-Cu’s evidence includes a distinctive methodology: transcriptome-wide analysis using databases like the Broad Institute Connectivity Map, which compares the gene-expression “signature” a compound induces against reference signatures. This is how the claim that GHK-Cu influences a large fraction of human genes arises.2 It is a legitimate hypothesis-generating tool, but a broad transcriptomic footprint is not evidence of clinical efficacy; many compounds perturb thousands of genes without therapeutic benefit.
Reading the methodology honestly, the evidence pyramid for KLOW’s components is bottom-heavy: lots of in-vitro and rodent work, one legitimately strong but narrowly-scoped human program (topical thymosin beta-4), and nothing at all for the blend. A responsible reader weights findings accordingly — treating cell and rodent data as mechanistic hypotheses, not as proof that injecting KLOW will build blood vessels or heal tissue in a person.
Safety and Tolerability: What Is and Isn’t Known
Safety data for KLOW is as thin as efficacy data — and in some ways thinner, because adverse-event reporting requires systematic human study that has not happened. What follows is drawn from component-level observations and from general pharmacological reasoning, and it should be read as a catalog of unknowns rather than a reassurance.
No blend-specific safety data. There is no toxicology study, no pharmacokinetic study, and no adverse-event dataset for the KLOW combination. Combining four biologically active peptides can, in principle, change the safety profile of each — through additive effects, altered clearance, or physical interactions in solution. None of this has been characterized.
Component-level considerations. For GHK-Cu, the copper content is a genuine consideration: copper is essential but toxic in excess, and repeated systemic administration raises theoretical concerns about copper accumulation that topical cosmetic use does not.2 For BPC-157 and TB-500, the pro-angiogenic mechanism is a double-edged sword: promoting new blood-vessel growth is desirable in a healing wound but potentially undesirable anywhere unwanted vascularization would be harmful, which is the basis of the frequently-raised (though not proven) theoretical concern about angiogenic peptides and tumor biology.3,14 This concern is theoretical — there is no human evidence that these peptides cause or accelerate cancer — but the absence of long-term human safety data means the concern cannot be dismissed either. For KPV, immunosuppressive/anti-inflammatory activity in principle could blunt appropriate immune responses, though its safety margin in animal models has appeared wide.9
Sterility, purity, and product-quality risks. Because these are research chemicals sold outside pharmaceutical manufacturing controls, real-world risk often comes not from the peptides’ intrinsic pharmacology but from product quality: incorrect labeled content, bacterial endotoxin, heavy-metal contamination, incorrect peptide identity, or non-sterile fill. Independent testing of gray-market peptides has repeatedly found products that do not match their labels. In a blend, this risk multiplies across four components. Any injection of a non-sterile or contaminated preparation carries risk of local infection, abscess, or systemic reaction entirely independent of the peptides themselves.
| Safety domain | State of knowledge for KLOW |
|---|---|
| Blend toxicology | No data |
| Blend pharmacokinetics/interactions | No data |
| Long-term human safety (any component, injected) | Essentially none |
| Theoretical angiogenesis/oncology concern | Unresolved; no human evidence either way |
| Copper accumulation (GHK-Cu, systemic) | Theoretical, uncharacterized for this dose/route |
| Product-quality/sterility risk | Significant in gray-market supply |
The bottom line on safety is that “no reported problems” is not the same as “shown to be safe.” Absence of evidence of harm, in a setting where no one is systematically looking for harm, is weak reassurance. A cautious reading treats KLOW’s safety as genuinely unknown, particularly for repeated or systemic use over time.
Handling and Reconstitution in a Research Context
Because KLOW is handled as a lyophilized (freeze-dried) research powder, a brief, strictly technical note on reconstitution is warranted — not as usage instructions for administration to any person, but as laboratory-handling context, since improper handling degrades the peptides and confounds any experimental interpretation. Nothing in this section should be read as endorsing self-administration.
The KLOW vial contains 80 mg of combined peptide as a dried solid. Reconstitution means dissolving that solid in a sterile diluent — typically bacteriostatic water (water with 0.9% benzyl alcohol, which suppresses bacterial growth for multi-draw storage). A commonly referenced approach for the 80 mg vial is adding 3.0 mL of bacteriostatic water, which yields a concentration of roughly 26.7 mg of total peptide per milliliter (of which about 16.7 mg/mL is GHK-Cu and 3.3 mg/mL each of BPC-157, TB-500, and KPV).1 The exact diluent volume is a matter of the researcher’s concentration math, not a fixed rule; the DosagePeptide dosages hub and the KLOW handling guide walk through reconstitution arithmetic and the reasoning behind diluent choices.
Key handling principles that affect data quality:
- Add diluent slowly down the vial wall, not directly onto the powder with force. Peptides are shear-sensitive; a hard stream can fragment or denature them. Let the vial sit and swirl gently — never shake vigorously.
- Do not mix components separately. Because KLOW is pre-blended, all four dissolve together; there is no way to reconstitute one peptide independently. This is a structural limitation of the fixed-ratio format.
- Storage. Lyophilized peptide is most stable frozen or refrigerated and protected from light. Once reconstituted, solutions are generally refrigerated (2–8 °C) and are far less stable than the dry powder; bacteriostatic water extends usable window relative to plain sterile water, but reconstituted peptide still degrades over days to weeks.
- Copper coloration. GHK-Cu gives solutions a characteristic blue tint from the copper(II) ion; this is expected for the GHK-Cu component and is not, by itself, a sign of spoilage.
- Sterility. Any breach of sterile technique introduces contamination risk that no peptide chemistry can offset.
These are the same handling considerations that apply to any research peptide, and they matter here mostly because degraded or contaminated material makes any downstream observation uninterpretable. In a controlled research setting, handling discipline is what separates a measurable result from noise. It does not, however, change the fundamental evidence picture: careful reconstitution of an unvalidated blend still yields an unvalidated blend.
Limitations and the Human-Evidence Gap
Everything above converges on a single, unavoidable conclusion: the gap between what is claimed for KLOW and what has actually been demonstrated is enormous. It is worth stating the limitations explicitly, because they are the real “evidence” a careful reader should carry away.
1. No study of the blend exists. This is the deepest limitation and it cannot be over-emphasized. Every other peptide combination question — synergy, ratio, interaction, net effect — is unanswerable because the experiment has never been done. The blend’s efficacy for angiogenesis or tissue repair is not “weakly supported”; it is unstudied.
2. Component data is preclinical. With the narrow exception of topical ophthalmic thymosin beta-4, the repair/angiogenesis evidence for all four peptides is in cells and rodents.3,8,9 Preclinical-to-human translation fails far more often than it succeeds; the history of angiogenesis and wound-healing therapeutics is littered with rodent successes that produced no human benefit.
3. Route and indication mismatch. The human thymosin beta-4 data is topical and ophthalmic; the human GHK-Cu data is topical and cosmetic.10,11,2 Neither speaks to injected systemic use for musculoskeletal or general tissue repair, which is how KLOW is typically marketed. Evidence for one route and indication does not transfer to another.
4. Replication and source concentration. A substantial share of BPC-157’s literature comes from a limited set of affiliated laboratories, and independent replication of the more dramatic findings is thin.14 Findings that have not been independently reproduced warrant extra caution.
5. Publication and commercial bias. Much of the accessible “evidence” a reader encounters online is vendor content, not primary literature. Vendors have a commercial interest in positive framing, and much web content restates the same handful of studies while omitting the “in rodents” and “no human trials” caveats. This article deliberately grounds each claim in primary sources for that reason.
6. Dosing is guesswork. Because there are no dose-finding studies for the blend, any specific dose figure is inferred from component data or convention, not established from controlled trials. There is no validated “effective dose” for KLOW because there is no trial that could have established one.
7. Long-term safety is unknown. As covered above, the absence of long-term human safety data — particularly regarding the theoretical angiogenesis/oncology concern and copper exposure — is a real limitation, not a technicality.3,14
8. Confounded real-world reports. Anecdotal reports of benefit — the “it worked for me” testimonials common in peptide communities — are among the weakest forms of evidence for a repair claim. Tissue healing follows its own timeline regardless of intervention, so improvement after using a peptide is easily confused with the natural resolution that would have occurred anyway. Add the placebo effect, concurrent rest or physiotherapy, and selective reporting (people who feel worse rarely post), and uncontrolled testimonials cannot distinguish a genuine effect from coincidence. This is exactly the confound that randomized, placebo-controlled trials exist to eliminate — and exactly the kind of trial KLOW has never had. Treating personal reports as evidence of angiogenic or regenerative efficacy is a category error, not a shortcut around the missing data.
None of this means the underlying peptides are uninteresting. GHK-Cu, BPC-157, thymosin beta-4, and KPV are legitimate subjects of ongoing scientific investigation, and some — thymosin beta-4 especially — have advanced into real clinical development for specific indications. The problem is not the molecules; it is the leap from “individually interesting molecules in preclinical models” to “an effective, safe, combined therapy for angiogenesis and tissue repair in humans.” That leap is not supported by evidence. The intellectually honest position is that KLOW is a research-stage combination whose central promise remains an open, untested hypothesis.
Regulatory Status
KLOW and its components sit in an unambiguous regulatory position: none is an FDA-approved drug, and the blend has no regulatory recognition of any kind. Understanding the specifics helps explain why these products are sold as “research chemicals” and why that label is meaningful.
No FDA approval. Neither KLOW as a blend nor any of its four peptides is approved by the FDA (or the EMA) as a drug for tissue repair, angiogenesis, or any other indication. There is no approved labeling, no established dosing, and no regulated manufacturing standard for these products as sold.1,13
The compounding pathway and Category 2. A key regulatory development concerns compounding. Under Section 503A of the Federal Food, Drug, and Cosmetic Act, compounding pharmacies may prepare medications from bulk drug substances only under defined conditions. In late 2023, the FDA placed BPC-157 (along with a number of other peptides) into “Category 2” of its interim bulk-substances policy — the category for substances that raise significant safety concerns or lack sufficient data, effectively meaning they should not be compounded.13 In April 2026 the FDA removed BPC-157 from Category 2 following withdrawal of its nomination, but critically it was not moved to Category 1 (permitted for compounding); it has no USP/NF monograph and remains without approval — a regulatory gray zone rather than a green light.13 Underscoring how unsettled this remains, the FDA scheduled a Pharmacy Compounding Advisory Committee (PCAC) meeting to review BPC-157 and TB-500 for July 23–24, 2026, meaning the compounding status of both peptides is still actively under reconsideration rather than resolved.
“Research use only” and its meaning. These products are sold labeled “for research use only,” “not for human consumption.” That designation is legally and practically significant: it places the products outside the drug-quality regulatory framework. There is no requirement that a research-use-only product meet pharmaceutical standards for sterility, identity, or potency, which is precisely why product-quality risk (discussed under safety) is so relevant. The label is not a marketing formality; it reflects that these substances have not been evaluated or authorized for use in people.
Thymosin beta-4’s distinct path. Among the components, thymosin beta-4 is the outlier: as the drug candidate RGN-259 it has been formally studied in FDA-regulated clinical trials for eye-surface disease, and has held orphan-drug and fast-track designations for specific ophthalmic indications.11,12 But that regulatory activity attaches to a specific topical ophthalmic product and indication — it does not confer any approval or legitimacy on injectable TB-500 or on KLOW.
International variation. Regulatory treatment varies by jurisdiction, and some of these peptides are also prohibited in competitive sport (thymosin beta-4 and related peptides appear on World Anti-Doping Agency prohibited lists). Researchers and readers are responsible for understanding the rules that apply in their own country and context.
The regulatory summary, then, mirrors the scientific one: KLOW is unapproved, unstandardized, and sold outside the drug framework, with a component (BPC-157) whose recent regulatory history underscores just how unsettled the field is. Regulatory status is not a substitute for efficacy evidence, but here the two point the same direction — toward “unproven research material,” not “established therapy.”
Frequently Asked Questions
Is there any human study showing KLOW promotes angiogenesis or tissue repair?
No. There is no published human trial — and no published animal or cell study — of the KLOW blend itself. All available evidence concerns the four individual peptides, mostly in cell cultures and rodents. The only rigorous human data among the components is for topical thymosin beta-4 (an eye-drop formulation) in dry-eye and corneal disease, which does not demonstrate anything about an injected four-peptide blend.1,10,11
Which KLOW component has the strongest evidence?
It depends on what you mean by “strongest.” GHK-Cu has the deepest and oldest literature but mainly for topical/cosmetic skin endpoints. Thymosin beta-4 (the basis of TB-500) has the only gold-standard randomized controlled human trials — but for topical ophthalmic use, not systemic repair, and even there the pivotal neurotrophic-keratopathy endpoint narrowly missed statistical significance. BPC-157 has the most mechanistically specific angiogenesis data (VEGFR2-Akt-eNOS) but only in cells and rodents, with essentially no human trials.1,2,3,10,11
Does combining four peptides make KLOW more effective than a single peptide?
There is no evidence for this. No study has compared KLOW to any single component or to simpler blends like BPC-157 + TB-500. The “four is better” premise is a marketing hypothesis, not a demonstrated fact, and combining active molecules can produce additive, negligible, or even antagonistic effects that no one has measured.1
Is KLOW approved or legal?
KLOW is not FDA-approved for any use, and none of its components is approved as a drug for tissue repair. These products are sold “for research use only,” outside the pharmaceutical-quality framework. BPC-157 was placed in the FDA’s Category 2 (do-not-compound) list in 2023 and removed in 2026 without being approved — a regulatory gray zone, not an endorsement — and remains under active review (a PCAC meeting on BPC-157 and TB-500 was scheduled for July 2026).13
What are the main safety concerns?
The honest answer is that KLOW’s safety is unknown — there is no blend toxicology, pharmacokinetic, or long-term human data. Component-level considerations include a theoretical (unproven) concern about pro-angiogenic peptides and unwanted vessel growth, possible copper accumulation from GHK-Cu with systemic use, and — often the largest real-world risk — product-quality problems (contamination, mislabeling, non-sterility) in gray-market supply.2,3,14
Why does the copper-containing solution turn blue?
The blue tint comes from the copper(II) ion in the GHK-Cu component. It is an expected optical property of GHK-Cu in solution and is not, by itself, an indicator of degradation. It does not tell you anything about the other three peptides or about sterility.2
How is KLOW different from BPC-157 + TB-500 or from Tri-Heal?
They are different commercial recombinations of overlapping peptides. BPC-157 + TB-500 is a two-peptide “recovery” pairing; Tri-Heal combines TB-500, BPC-157, and KPV; KLOW adds GHK-Cu on top of those three. None has been compared head-to-head in any study, so no formulation can be said to be superior on evidence.1
Can I use this article as a protocol or dosing guide?
No. This is an educational review of the evidence, not a protocol, and it does not recommend administering KLOW to anyone. There is no validated human dose for the blend because no dose-finding trial exists. Any specific numbers seen online are inferred from component data or convention, not established by controlled research.
References
- DosagePeptide. KLOW (80 mg vial) composition and research-only status (manufacturer specification). dosagepeptide.com/peptide-blends/klow-80-mg-vial-dosage-protocol.
- Pickart L, Margolina A. Regenerative and Protective Actions of the GHK-Cu Peptide in the Light of the New Gene Data. Int J Mol Sci. 2018;19(7):1987. PMID: 29986520.
- Hsieh MJ, Liu HT, Wang CN, et al. Therapeutic potential of pro-angiogenic BPC157 is associated with VEGFR2 activation and up-regulation. J Mol Med (Berl). 2017;95(3):323–333. doi:10.1007/s00109-016-1488-y. PMID: 27847966.
- Modulatory effect of gastric pentadecapeptide BPC 157 on angiogenesis in muscle and tendon healing. PMID: 20388964.
- Hsieh MJ, et al. Modulatory effects of BPC 157 on vasomotor tone and the activation of Src-Caveolin-1-endothelial nitric oxide synthase pathway. Sci Rep. 2020;10:17078. doi:10.1038/s41598-020-74022-y. PMID: 33051481.
- Chang CH, Tsai WC, Lin MS, Hsu YH, Pang JHS. The promoting effect of pentadecapeptide BPC 157 on tendon healing involves tendon fibroblast outgrowth, cell survival, and migration. J Appl Physiol. 2011;110(3):774–780.
- Goldstein AL, Hannappel E, Sosne G, Kleinman HK. Thymosin beta4: a multi-functional regenerative peptide. Expert Opin Biol Ther. 2012;12(1):37–51.
- Malinda KM, Sidhu GS, Mani H, et al. Thymosin beta4 accelerates wound healing. J Invest Dermatol. 1999;113(3):364–368. PMID: 10469335.
- Dalmasso G, Charrier-Hisamuddin L, Nguyen HTT, et al. PepT1-mediated tripeptide KPV uptake reduces intestinal inflammation. Gastroenterology. 2008;134(1):166–178. PMID: 18061177.
- Sosne G, Kim C, Dunn SP. Thymosin beta4 significantly improves signs and symptoms of severe dry eye in a phase 2 randomized trial. Cornea. 2015;34(5):491–496. PMID: 25826322.
- 0.1% RGN-259 (Thymosin beta4) Ophthalmic Solution in Neurotrophic Keratopathy: Randomized, Placebo-Controlled, Double-Masked Phase III (SEER-1) Trial. 2023. PMC9820614.
- Study of Thymosin Beta 4 in Patients With Venous Stasis Ulcers. ClinicalTrials.gov identifier NCT00832091.
- U.S. Food and Drug Administration. Interim Policy on Compounding Using Bulk Drug Substances Under Section 503A; Category 1/Category 2 bulk drug substances lists (BPC-157 listing 2023; removal 2026; PCAC review scheduled July 2026). fda.gov.
- Regeneration or Risk? A Narrative Review of BPC-157 for Musculoskeletal Healing. Curr Rev Musculoskelet Med. 2025. doi:10.1007/s12178-025-09990-7.
- Enhanced angiogenic effects of RGD, GHK peptides and copper(II) compositions in a synthetic cryogel ECM model. Mater Sci Eng C (Elsevier). doi:10.1016/j.msec.2020.111593.
Educational and research-use disclaimer: This article is provided for educational and research purposes only. KLOW and its component peptides (GHK-Cu, BPC-157, TB-500, KPV) are unapproved research chemicals, not medicines. Nothing here is medical advice, a treatment protocol, or a claim that KLOW diagnoses, treats, cures, or prevents any disease. The KLOW blend has not been evaluated in any human or animal study, and the described mechanisms are preclinical and hypothesis-generating. Consult qualified professionals and comply with all applicable laws and institutional requirements before conducting any research.