Sermorelin is one of the oldest and most extensively studied of the so-called “growth hormone peptides,” and it occupies an unusual place in the current wellness landscape. It is a genuine pharmaceutical molecule with a documented clinical history, yet the product that once carried that history — the branded injectable Geref — was voluntarily pulled from the United States market in the late 2000s. Today the compound survives almost entirely in two very different contexts: as a prescription drug produced by compounding pharmacies, and as a research chemical sold to laboratories. Neither of those routes is an FDA-approved consumer product, and that distinction matters enormously when trying to answer the question this article poses: does sermorelin actually support growth hormone output and tissue regeneration in aging adults?
The honest short answer is that sermorelin can measurably raise the body’s own growth hormone (GH) and insulin-like growth factor 1 (IGF-1) secretion in older people, and a small number of controlled human trials from the 1990s and 2000s support that. What is far less certain — and where most marketing dramatically overreaches — is whether those hormonal shifts translate into meaningful, durable improvements in body composition, physical function, cognition, or genuine “regeneration” of aging tissues. The biochemistry is real. The clinical endpoints that patients actually care about remain thinly evidenced, studied in small samples, and largely unreplicated at scale.
This guide walks through what sermorelin is, how it works at the receptor level, what the primary human and preclinical literature genuinely shows, how it compares with related molecules such as tesamorelin and CJC-1295, and where the evidence is weakest. Throughout, the aim is to separate three things that are frequently blurred together: what has been demonstrated in controlled trials, what is biologically plausible but unproven, and what is simply being asserted. Everything below is educational and research-oriented; none of it is medical advice or a recommendation to use sermorelin in humans.
What Sermorelin Is and Where It Came From
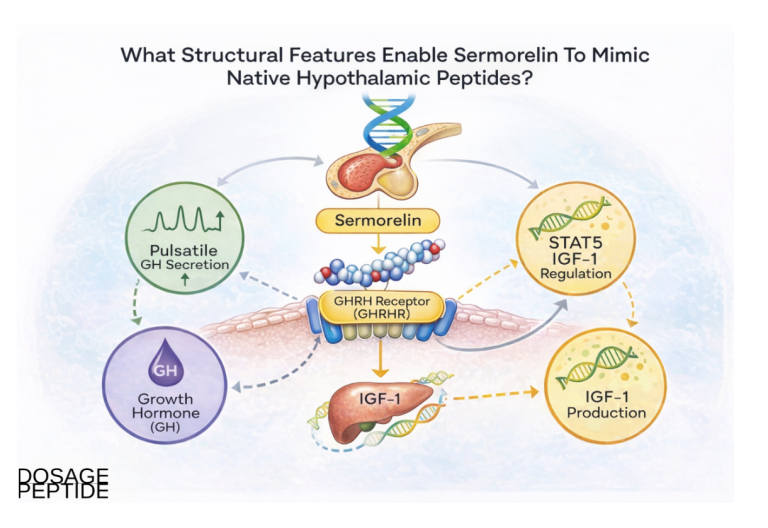
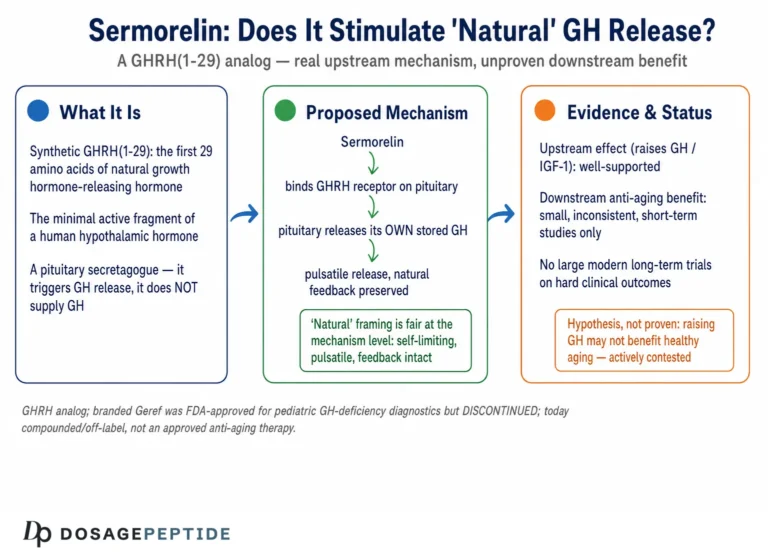
Sermorelin is a synthetic peptide corresponding to the first 29 amino acids of endogenous human growth hormone-releasing hormone (GHRH). Native GHRH is a 44-amino-acid hormone secreted by the hypothalamus, but decades of structure-activity research established that the biological activity of the full molecule is concentrated in its N-terminal region. The 1–29 fragment — often written GRF(1–29) or GHRH(1–29) — was identified as the shortest sequence that retains essentially full GH-releasing potency, which is why it became the template for a drug.13 In pharmaceutical form the molecule is supplied as sermorelin acetate, a lyophilized (freeze-dried) powder reconstituted before subcutaneous injection.
The compound’s regulatory history is specific and worth stating precisely, because it is routinely misrepresented. Sermorelin acetate was first approved by the U.S. Food and Drug Administration in 1990 under the brand name Geref for use as a diagnostic agent — a provocative stimulus to test whether a child’s pituitary could release growth hormone. A separate therapeutic approval followed in 1997 for the treatment of idiopathic growth hormone deficiency in children with growth failure.3 Note the population: the approved uses were in children, either to diagnose or to treat pediatric GH deficiency. Sermorelin was never FDA-approved as an anti-aging therapy, a body-composition drug, or a general wellness product for adults.
In 2008 the manufacturer, EMD Serono, notified the FDA that it was discontinuing sermorelin and requested withdrawal of the associated New Drug Applications; the agency withdrew marketing approval effective in 2009.34 Critically, this was a commercial decision, not a safety or efficacy verdict. In a 2013 Federal Register notice the FDA formally determined that Geref (sermorelin acetate) injection was “not withdrawn from sale for reasons of safety or effectiveness.”4 That determination is what later allowed compounding pharmacies to prepare sermorelin, and it is why you will still hear the phrase “withdrawn but not for safety reasons.” The market had simply shifted toward recombinant human growth hormone (somatropin) for pediatric indications, and a GHRH analog was no longer commercially worthwhile to maintain.
The practical consequence is that there is no FDA-approved sermorelin product on the U.S. market today. What exists instead are (a) compounded sermorelin dispensed under a prescription through the pharmacy compounding framework, and (b) research-grade sermorelin sold explicitly for laboratory use and labeled not for human consumption. A site like DosagePeptide.com catalogs sermorelin within its research-reference material precisely because the molecule has no approved consumer form; see the Sermorelin (10 mg vial) dosage protocol and the Sermorelin (5 mg vial) dosage protocol pages for how the compound is described in a strictly research context.
Historically, the scientific rationale for developing a GHRH analog was elegant. Rather than replacing growth hormone directly — which overrides the body’s own regulatory machinery — a GHRH analog nudges the pituitary to release its own GH in the normal pulsatile pattern, subject to the body’s built-in braking system. Researchers such as Richard Walker argued that this “secretagogue” approach could, in principle, be a more physiological way to address the age-related decline in GH secretion than injecting recombinant hormone.5 Whether that theoretical elegance produces clinically meaningful outcomes is the central question the rest of this article examines.
How Sermorelin Works: The Molecular Mechanism
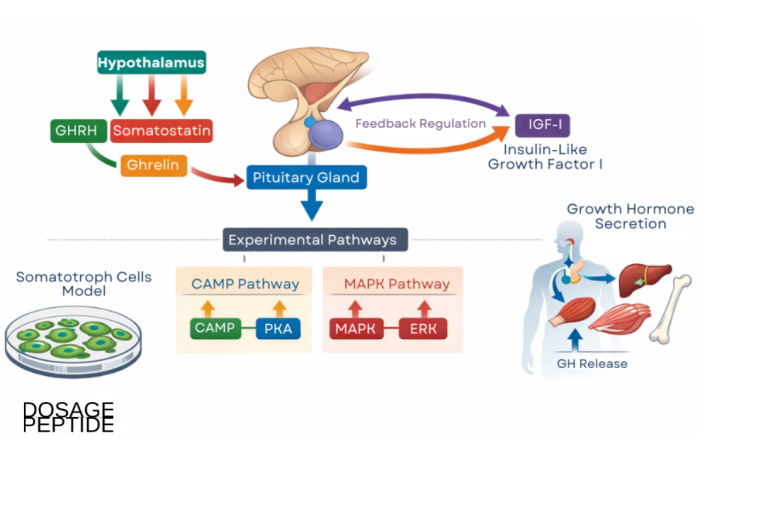
Sermorelin’s mechanism is the same as that of endogenous GHRH, which is exactly the point of using the 1–29 fragment. The peptide binds to the growth hormone-releasing hormone receptor (GHRHR), a class B G-protein-coupled receptor expressed on the surface of somatotroph cells in the anterior pituitary gland. Receptor binding activates a stimulatory G-protein (Gs), which in turn activates adenylyl cyclase. The resulting rise in intracellular cyclic AMP (cAMP) activates protein kinase A and triggers calcium influx, and this cascade drives both the synthesis and the pulsatile release of growth hormone stored within the somatotrophs.16 In other words, sermorelin does not contain any growth hormone; it is an upstream signal that instructs the pituitary to make and release its own.
This upstream position in the hormonal cascade produces several features that distinguish sermorelin from recombinant GH. First, the GH released in response to sermorelin is subject to the body’s existing negative-feedback control. The hypothalamus secretes somatostatin, an inhibitory hormone that suppresses GH release, and circulating IGF-1 feeds back to restrain the axis. Because sermorelin works through the normal receptor, an excess of GH or IGF-1 tends to be counter-regulated by somatostatin, which theoretically makes it much harder to drive GH to grossly supraphysiologic levels than it is with direct GH injection.15 This is frequently summarized as sermorelin “preserving the feedback loop,” and it is a genuine pharmacological difference — though it should not be mistaken for a guarantee of safety.
Second, sermorelin tends to preserve the pulsatile character of GH secretion. Endogenous GH is not released as a steady trickle; it comes in bursts, with the largest pulses occurring during slow-wave sleep. A GHRH stimulus given at night can amplify these natural nocturnal pulses rather than flattening them into a continuous elevation, and the pulsatile pattern itself appears to matter for downstream signaling. This is the biological reason many research protocols specify bedtime administration.7
Third, and importantly for interpreting efficacy, sermorelin’s action depends on a functioning pituitary. If the somatotrophs are still capable of producing GH, sermorelin can coax them to do so. If the pituitary itself is exhausted or damaged — as opposed to simply under-stimulated by an aging hypothalamus — a GHRH analog has little to work with. Age-related GH decline (sometimes called the “somatopause”) is thought to be driven substantially by reduced hypothalamic GHRH output and increased somatostatin tone rather than by outright pituitary failure, which is the theoretical basis for expecting older adults to still respond to sermorelin.58
The molecule’s pharmacokinetics reinforce how it behaves. Sermorelin has a very short circulating half-life — on the order of 11 to 12 minutes after subcutaneous or intravenous administration — with peak concentrations reached within roughly 5 to 20 minutes and rapid clearance thereafter.9 That brevity is deliberate and, in one sense, advantageous: a short, sharp GHRH signal mimics a natural burst and then clears, allowing the axis to reset. But it also means that a single injection produces only a transient window of receptor stimulation, which is one of the core limitations that later, longer-acting analogs were engineered to overcome. The next section turns from mechanism to what actually happens when this cascade is triggered repeatedly in aging humans.
What the Human Evidence Actually Shows
Here it is essential to be precise about the level of evidence, because the gap between “raises a hormone marker” and “improves health” is where most claims about sermorelin fall apart. The strongest, most consistent finding across the human literature is a biochemical one: GHRH(1–29) administration reliably increases GH secretion and, with repeated dosing, raises circulating IGF-1 in older adults whose baseline levels have declined with age. The clinical endpoints that would justify calling it a “regeneration” therapy are far more tentative.
The foundational study is Corpas and colleagues (1992), who gave GHRH(1–29) twice daily to healthy older men and demonstrated that the treatment reversed the age-related decrease in GH and IGF-1, pushing values in elderly men toward the range seen in younger men.10 This established the core proof of concept: an aging GH axis remains responsive to GHRH stimulation. A related line of work by Vittone and colleagues (1997) examined single nightly injections of GHRH(1–29) in healthy elderly men. It documented increases in GH secretion, but its actual conclusion is an important corrective rather than an endorsement: single nightly dosing was less effective than multiple daily doses at eliciting GH- and IGF-1-mediated effects, and the regimen produced no significant change in body composition on DEXA. In other words, even when the aging axis responds, the dosing schedule matters — a once-daily bedtime stimulus may under-deliver relative to divided dosing.11
The most cited body-composition study is Khorram, Laughlin, and Yen (1997), a single-blind, placebo-controlled trial in which ten women and nine men aged 55 to 71 received four weeks of nightly placebo followed by 16 weeks of a GHRH(1–29) analog. The treatment significantly increased GH release and 12-hour mean GH levels in both sexes. The investigators reported a significant increase in lean body mass in the men (reported at about 1.26 kg), increased skin thickness in both sexes, improved insulin sensitivity, and a trend toward positive nitrogen balance.12 These are real, peer-reviewed findings — but note the caveats that responsible interpretation requires: the sample was tiny (fewer than 20 people), the study was single-blind rather than double-blind, the duration was months rather than years, and several endpoints were surrogate markers rather than hard functional outcomes such as strength, mobility, or fracture risk.
On cognition, the best evidence comes from Baker and colleagues (2012), a randomized, double-blind, placebo-controlled trial of GHRH in 152 adults — some with mild cognitive impairment and some cognitively healthy older adults — over 20 weeks. GHRH treatment was associated with favorable effects on aspects of cognition, particularly executive function, in both groups.13 This is one of the more methodologically robust trials in the entire GHRH literature. Even so, it used tesamorelin (a longer-acting GHRH analog) rather than sermorelin specifically, it measured cognitive test performance rather than prevention of dementia, and its findings have not been translated into an approved cognitive indication. It is suggestive, not conclusive.
| Study | Population | Design | Main reported finding | Evidence caveat |
|---|---|---|---|---|
| Corpas et al., 199210 | Healthy older vs. young men | GHRH(1–29) twice daily | Reversed age-related fall in GH and IGF-1 | Very small; biochemical endpoint only |
| Vittone et al., 199711 | Healthy elderly men | Single nightly GHRH(1–29) | Increased GH secretion | Single nightly dosing less effective than divided; no DEXA body-composition change |
| Khorram et al., 199712 | Men and women, 55–71 | Single-blind, placebo-controlled, 16 wk | ↑Lean mass (men), ↑skin thickness, ↑insulin sensitivity | <20 subjects; single-blind; no functional endpoints |
| Baker et al., 201213 | Older adults ± MCI | Randomized, double-blind, 20 wk | Favorable effect on executive cognition | Used tesamorelin, not sermorelin; test scores, not disease |
Taken together, the human evidence supports a narrow, defensible claim: in aging adults with an intact pituitary, GHRH analogs including sermorelin can raise endogenous GH and IGF-1 and produce modest, short-term shifts in surrogate markers of body composition and metabolism. It does not support the far broader claims — reversed aging, dramatic muscle gain, guaranteed cognitive protection, tissue “regeneration” — that dominate consumer marketing. Much of the sermorelin-specific human data is decades old, small, and never scaled into the large, long-duration randomized trials that would be needed to establish clinical benefit and long-term safety.
Sermorelin and the Aging Growth Hormone Axis
To understand why sermorelin is even a candidate for aging-related use, it helps to understand what happens to the GH–IGF-1 axis over the lifespan. Growth hormone secretion peaks around puberty and then declines progressively across adulthood, falling by roughly 14 percent per decade in many individuals, with a parallel decline in IGF-1. This gradual reduction is often termed the “somatopause,” drawing an analogy to menopause and andropause.8 The decline correlates with several changes that also accompany aging: increased visceral fat, reduced lean muscle mass, thinner skin, altered lipid profiles, poorer sleep quality, and reduced sense of vitality. This correlation is the seed of the entire “GH decline causes aging” hypothesis.
The crucial and frequently ignored point is that correlation is not causation, and the relationship may even run in a protective direction in some respects. Epidemiological and animal data complicate the simplistic “more GH is younger” narrative. Populations and animal models with reduced GH/IGF-1 signaling — such as individuals with Laron syndrome (GH receptor deficiency) — often show remarkable protection from cancer and diabetes and, in animal models, extended lifespan.8 This is the central paradox of GH-axis anti-aging strategies: the same signaling that supports tissue growth and repair in youth may, when sustained at high levels later in life, carry metabolic and proliferative costs. Any honest account of sermorelin must sit with this tension rather than ignore it.
Sermorelin’s theoretical appeal in this context is that it works with the aging axis rather than overriding it. Because the somatopause appears to be driven largely by reduced hypothalamic GHRH signaling and heightened somatostatin tone — not by a broken pituitary — a GHRH analog can, at least biochemically, restore a more youthful pattern of GH pulsatility while leaving the feedback brakes intact. Proponents argue this makes it a “gentler,” more self-limiting way to nudge the axis than injecting recombinant GH, which bypasses all of that regulation.5 The Corpas and Khorram studies are the empirical anchor for this argument: they show that the aging axis remains responsive and that surrogate markers can shift.1012
But the leap from “restores a hormonal pattern” to “restores youthful function” is precisely where evidence thins out. The landmark cautionary tale is the broader field of GH replacement in healthy older adults. A well-known 1990 study by Rudman and a later systematic review of GH use in the healthy elderly found that while GH could modestly increase lean mass and decrease fat mass, it came with a meaningful rate of side effects — joint pain, swelling, carpal tunnel syndrome, insulin resistance — and no convincing evidence of improved strength, function, or longevity.8 Because sermorelin ultimately acts by raising the same GH and IGF-1, there is no strong reason to assume it escapes these trade-offs entirely; it may simply produce a smaller, more physiological version of the same effect, with correspondingly smaller benefits and risks.
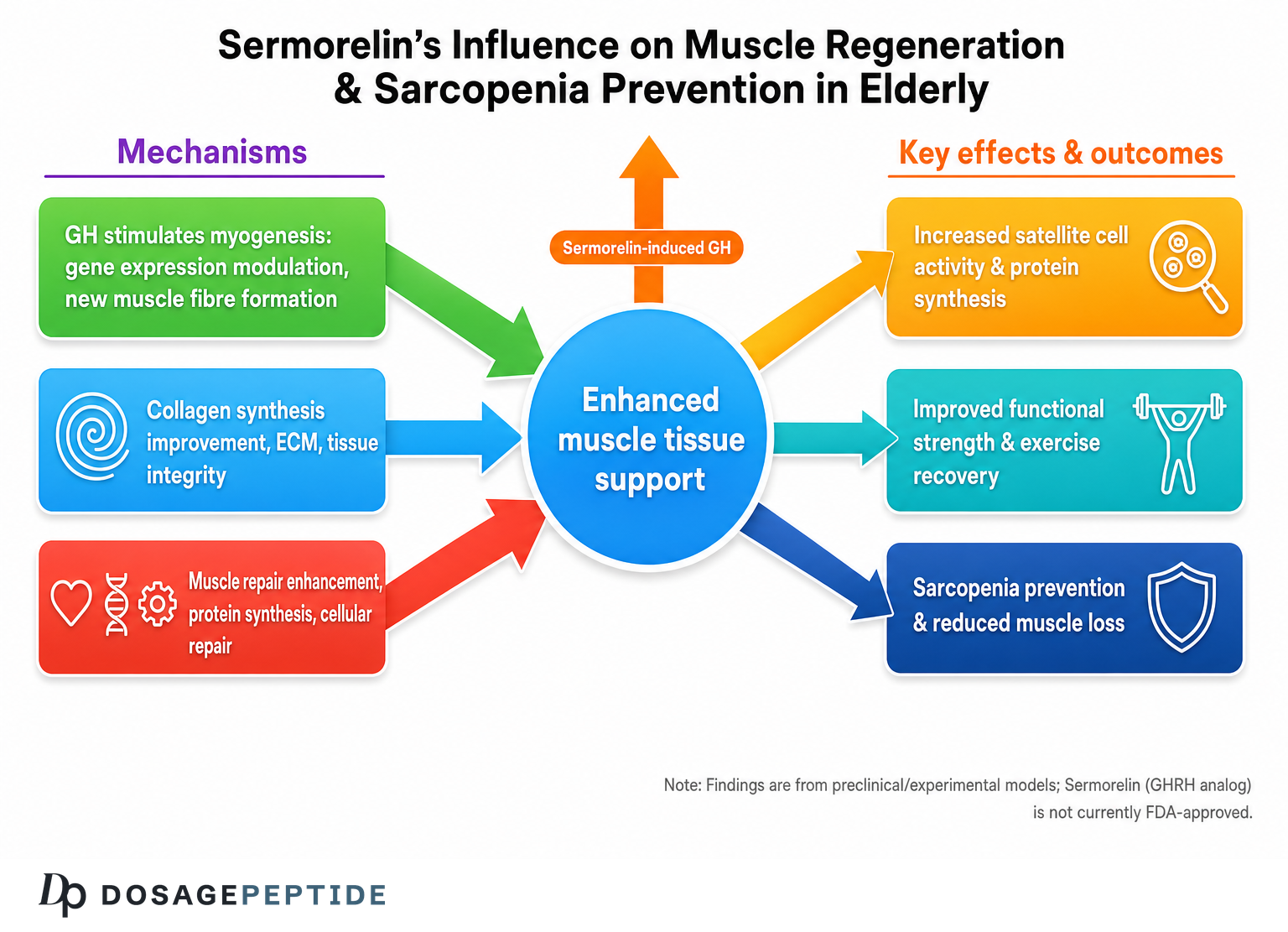
The concept of “regeneration” specifically deserves scrutiny. GH and IGF-1 do participate in tissue repair, protein synthesis, collagen turnover, and cellular proliferation, which is why increased skin thickness and positive nitrogen balance show up in the trials.12 But “participates in repair processes” is not the same as “regenerates aged organs” or “reverses aging.” There is no controlled human trial demonstrating that sermorelin regrows cartilage, reverses sarcopenia in a functionally meaningful way, heals injuries faster in humans, or extends healthspan. Those are hypotheses derived from mechanism and from short-term surrogate data, not established outcomes. Readers exploring the wider GH-peptide space can compare this cautious framing with the tesamorelin literature, which is the most rigorously studied GHRH analog for a specific human indication — see the overview of what tesamorelin is and how it works.
How Sermorelin Compares to Related GHRH Analogs and Secretagogues
Sermorelin is best understood as the prototype of a family of molecules that all try to solve the same problem — native GHRH is degraded within minutes — using different structural tricks. Understanding those differences clarifies both sermorelin’s appeal and its limitations. The molecules fall into two broad mechanistic classes: GHRH analogs (which act at the GHRH receptor, like sermorelin) and growth hormone secretagogues or ghrelin-mimetics (which act at a separate receptor, the GHS-R). These classes are sometimes combined because they stimulate GH through complementary pathways.114
Within the GHRH-analog class, the defining variable is metabolic stability. Sermorelin, as the bare 1–29 fragment, is the least modified and therefore the shortest-acting, with a half-life of roughly 11 to 12 minutes.9 CJC-1295 without DAC (also called modified GRF 1-29) introduces amino-acid substitutions — most importantly a D-alanine at position 2 to resist cleavage by the enzyme DPP-4 — that roughly double the effective half-life to around 30 minutes. CJC-1295 with DAC (Drug Affinity Complex) adds a linker that lets the peptide bind covalently to circulating albumin, extending the half-life to days and producing a sustained “GH bleed” rather than a discrete pulse. Tesamorelin is a stabilized full-length (1–44) analog with an N-terminal modification that resists degradation; it is the only member of this family with current FDA approval, specifically for reducing excess visceral fat in HIV-associated lipodystrophy.14
| Compound | Class | Approx. half-life | Key structural feature | Regulatory status |
|---|---|---|---|---|
| Sermorelin | GHRH analog (1–29) | ~11–12 min | Unmodified N-terminal fragment | Formerly approved (Geref, withdrawn 2008–09); now compounded/research only |
| CJC-1295 (no DAC) | GHRH analog | ~30 min | DPP-4-resistant substitutions | Not FDA-approved; research only |
| CJC-1295 (with DAC) | GHRH analog | ~6–8 days | Albumin-binding linker | Not FDA-approved; research only |
| Tesamorelin | GHRH analog (1–44) | ~26–38 min | Stabilized N-terminal group | FDA-approved for HIV lipodystrophy only |
| Ipamorelin / GHRP-6 | Ghrelin-mimetic (GHS-R) | ~2 h / ~short | Acts at a different receptor | Not FDA-approved; research only |
This comparison reframes the “is sermorelin effective” question. Sermorelin’s short half-life is a double-edged trait. On one hand, it produces a clean, transient pulse that closely mimics natural GHRH physiology and lets somatostatin feedback operate normally. On the other hand, later analogs were specifically engineered because that transient signal was seen as a limitation for producing sustained IGF-1 elevation. If a given research question is about maximal, sustained GH/IGF-1 exposure, the longer-acting molecules are “stronger”; if the question is about the most physiological, self-limiting stimulus, sermorelin’s brevity is arguably a feature. Neither is universally “better” — they answer different questions.
Because GHRH analogs and ghrelin-mimetics act on different receptors, combinations such as a GHRH analog plus ipamorelin are commonly studied in the research literature for synergistic GH release. The general observation is that pairing the two classes produces a larger GH pulse than either alone, since one amplifies the releasing signal while the other suppresses somatostatin.1 DosagePeptide.com maintains reference material on several of these related molecules and blends, including the Tesamorelin (10 mg vial) protocol and the CJC-1295 (no DAC) & Ipamorelin blend protocol. The key honesty point is that for none of these — sermorelin included — except tesamorelin’s narrow HIV indication is there an FDA-approved use in the general adult or aging population.
Research Models and Study Methodology
The way sermorelin and its relatives are studied shapes what we can and cannot conclude, so it is worth understanding the methodological landscape. GHRH-analog research spans four tiers of evidence, each answering a different kind of question and carrying a different weight: in vitro receptor and cell studies, animal models, human diagnostic-provocation studies, and human therapeutic trials. Marketing frequently borrows the excitement of the lower tiers (dramatic animal or cell findings) and presents it as though it were top-tier human proof.
At the in vitro level, researchers use pituitary cell cultures and GHRH-receptor-expressing cell lines to characterize binding affinity, cAMP signaling, and GH release. These studies confirm the receptor-level mechanism described earlier and allow structure-activity comparisons between analogs. They say nothing directly about clinical benefit — a molecule can be a potent GH secretagogue in a dish and still fail to help a living organism. In animal models, GHRH analogs have been studied for effects on growth, body composition, and, more recently, tissue-specific outcomes. A 2026 study in an Alzheimer’s disease mouse model, for example, reported that GHRH attenuated amyloid deposition and neuroinflammation — an intriguing preclinical signal, but one that is explicitly animal-model data and cannot be assumed to translate to humans.15
The human diagnostic literature is actually where sermorelin has its firmest footing, because that was its approved use. As a provocative test, sermorelin was administered and the resulting GH surge measured to assess pituitary reserve — a well-validated, reproducible pharmacodynamic effect.3 This is why we can say with confidence that sermorelin “works” in the narrow sense of reliably triggering GH release: that specific effect was the basis of an FDA-approved diagnostic. The controversy is entirely about whether repeated therapeutic dosing yields clinical benefit, which is a different and much harder question.
The human therapeutic trials — Corpas, Vittone, Khorram, and the tesamorelin cognition work — share a set of methodological limitations that recur so consistently they define the field. Sample sizes are small, often under 20 and rarely over 150. Durations are short, typically 16 to 26 weeks, far too brief to detect either durable functional benefit or long-latency risks such as cancer. Many endpoints are surrogate biomarkers (IGF-1, lean mass by imaging, skin thickness) rather than outcomes patients experience (strength, independence, injury recovery, quality of life). Blinding is sometimes single rather than double. And crucially, much of the sermorelin-specific work predates modern trial standards and has never been replicated at scale.101112
| Evidence tier | What it can show | What it cannot show |
|---|---|---|
| In vitro / cell studies | Receptor binding, cAMP signaling, GH release mechanism | Any clinical benefit or safety in a whole organism |
| Animal models | Directional effects on growth, tissue, body composition | Reliable prediction of human response |
| Human diagnostic provocation | That sermorelin reliably triggers GH release (validated) | Whether chronic dosing improves health |
| Human therapeutic trials | Short-term surrogate shifts (IGF-1, lean mass, cognition scores) | Long-term function, safety, and durability at scale |
The upshot for methodology is a discipline in reading claims: always ask which tier a given statement comes from. “Sermorelin increases GH” is a robust, top-tier-validated fact. “Sermorelin reduces neuroinflammation” is, at present, an animal-model observation. “Sermorelin regenerates aging tissue and reverses biological aging” is not supported at any tier by controlled human data. Keeping those distinctions straight is the single most useful skill for evaluating this compound honestly.
Safety, Tolerability, and Pharmacokinetics
Within its studied contexts, sermorelin has a reassuring short-term tolerability profile, which is one reason it was originally considered suitable for use in children. The most common adverse effects are local and mild: injection-site reactions such as redness, swelling, pain, or itching, reported in a meaningful minority of users and typically resolving within hours to a couple of weeks. Systemic effects reported in the diagnostic and therapeutic literature include facial flushing, headache, nausea, occasional vomiting, dizziness, altered taste (dysgeusia), pallor, and a sensation of chest tightness, generally at low frequency.916 In the historical clinical-trial dataset, discontinuations due to adverse effects were uncommon — of several hundred patients exposed, only a small number stopped therapy because of injection reactions.16
The pharmacokinetic profile underpins this tolerability. After subcutaneous injection, sermorelin reaches peak plasma concentration within about 5 to 20 minutes and is cleared with a half-life of roughly 11 to 12 minutes, so systemic exposure to the peptide itself is brief.9 The downstream GH pulse it triggers is likewise transient. This short exposure, combined with the intact somatostatin feedback loop, is the mechanistic reason sermorelin is much less prone than recombinant GH to drive the sustained supraphysiologic IGF-1 levels associated with GH’s more troubling side effects — fluid retention, joint pain, carpal tunnel syndrome, and insulin resistance. That is a genuine theoretical safety advantage, but “less prone” is not “immune,” and any therapy that raises GH and IGF-1 inherits some of the same theoretical concerns.
The most important of those concerns is the relationship between IGF-1 and cell proliferation. IGF-1 is a growth factor, and chronically elevated IGF-1 has been associated in epidemiological studies with increased risk of certain cancers. Because sermorelin raises endogenous IGF-1, the standard and appropriate contraindication is active malignancy — GHRH analogs are generally considered inappropriate in anyone with active cancer, and this caution appears throughout the clinical literature and prescribing guidance for the drug class.58 Critically, no long-term human trial of sermorelin has been large or lengthy enough to quantify cancer risk from chronic use in aging adults. The absence of a documented signal in short trials is not the same as demonstrated long-term safety; it simply reflects that the studies were too small and too brief to find such a signal even if it exists.
Other practical safety considerations follow from the mechanism. Because sermorelin can raise blood glucose and affect insulin sensitivity in complex ways, it warrants caution in people with diabetes or impaired glucose tolerance. Conditions that alter the GH axis — untreated hypothyroidism, use of glucocorticoids, obesity, and hyperglycemia — can blunt the GH response, meaning both efficacy and dosing are confounded by an individual’s physiology.39 These interactions are well characterized from the diagnostic era, when a blunted response could produce a false diagnosis of GH deficiency.
Finally, the safety picture for research-grade material is fundamentally different from the safety picture for the historical pharmaceutical. The tolerability data above come from a well-characterized, pharmaceutical-grade product used under medical supervision. Research chemicals sold outside that framework carry additional, unquantified risks related to purity, correct identity, endotoxin contamination, incorrect labeled mass, and reconstitution error — none of which are properties of the molecule itself but all of which affect real-world safety. Any statement that “sermorelin is safe” must be qualified by which sermorelin, made how, and used under what supervision.
Handling and Reconstitution in a Research Context
Sermorelin is supplied as a lyophilized powder because peptides of this type are unstable in solution and degrade over time; the freeze-dried form preserves the molecule until it is needed. In a research setting, the powder is reconstituted with a sterile diluent — most commonly bacteriostatic water, which contains a small amount of benzyl alcohol as a preservative that permits multi-day storage of the reconstituted solution. Sterile or standard water for injection can also be used but lacks a preservative and is generally reserved for single-use scenarios. The handling principles below are described strictly for laboratory reference; they are not instructions for human use.
The core arithmetic of reconstitution is straightforward but must be done deliberately. The final concentration equals the mass of peptide in the vial divided by the volume of diluent added. For example, adding 2 mL of bacteriostatic water to a 10 mg vial yields a concentration of 5 mg/mL; adding 3 mL to that same vial yields roughly 3.33 mg/mL; and reconstituting a 5 mg vial with 3 mL yields about 1.67 mg/mL. Because research doses are typically discussed in micrograms while vials are labeled in milligrams, unit conversion (1 mg = 1000 mcg) is the single most common source of error. The Sermorelin dosage protocol reference lays out worked reconstitution ratios and the corresponding draw volumes for common concentrations.
| Vial size | Diluent added | Resulting concentration | Volume for a 300 mcg reference amount |
|---|---|---|---|
| 10 mg | 2 mL | 5000 mcg/mL | 0.06 mL |
| 10 mg | 3 mL | ~3333 mcg/mL | ~0.09 mL |
| 5 mg | 2 mL | 2500 mcg/mL | 0.12 mL |
| 5 mg | 3 mL | ~1667 mcg/mL | ~0.18 mL |
Proper handling technique matters because it protects the integrity of the peptide and the validity of any research using it. The diluent should be introduced slowly down the inner wall of the vial rather than squirted directly onto the powder, which can shear and denature the peptide; the vial is then swirled gently, never shaken, until fully dissolved. Reconstituted sermorelin is stored refrigerated, typically at 2 to 8 degrees Celsius, and protected from light; the lyophilized powder is more stable and can be kept frozen for longer-term storage. Repeated freeze-thaw cycles of the reconstituted solution should be avoided because each cycle degrades peptide.2
Aseptic practice is standard: the rubber stopper is swabbed with alcohol before each needle entry, and a fresh sterile needle and syringe are used for each draw to prevent contamination of the vial. Because bacteriostatic water only inhibits, rather than eliminates, microbial growth, reconstituted vials are generally considered usable for a limited window — multi-dose-vial guidance commonly cites a beyond-use window of about 28 days refrigerated — after which any remaining solution is discarded. These are the same sterile-handling and beyond-use-dating principles that apply to any multi-dose injectable preparation.17 Again, this material is presented as laboratory-handling context for a research compound, not as a protocol for administration to humans.
Limitations and the Human-Evidence Gap
Having surveyed what sermorelin can do, it is worth consolidating what it cannot yet claim — because this is where responsible interpretation departs most sharply from marketing. The central limitation is simple to state: there is a wide gap between sermorelin’s well-established ability to raise a hormone and any demonstrated ability to improve the outcomes people actually seek. That gap has never been closed by adequate human trials, and pretending otherwise is the field’s defining failure of honesty.
First, the sermorelin-specific efficacy evidence for aging adults rests on a handful of small studies, most of them from the 1990s, with fewer than 20 participants in the key body-composition trial.12 No large, multi-year, double-blind randomized controlled trial has ever tested whether sermorelin improves hard endpoints — muscle strength, physical function, fall or fracture rates, injury recovery, disability-free survival, or mortality — in an aging population. The strongest cognitive data actually come from tesamorelin, a different molecule, and measure test scores rather than disease prevention.13 Extrapolating from these to sweeping anti-aging benefit is not scientifically warranted.
Second, the word “regeneration” is doing heavy, unearned lifting in most sermorelin marketing. GH and IGF-1 are involved in protein synthesis, collagen turnover, and cellular repair, and short-term trials show plausible surrogate signals like increased skin thickness and positive nitrogen balance.12 But no controlled human study demonstrates that sermorelin regenerates cartilage, reverses age-related muscle loss in a functionally meaningful way, heals wounds or injuries faster in humans, rejuvenates organs, or slows biological aging by any validated measure. Those are mechanistic hypotheses and preclinical hints, not clinical facts. The Alzheimer’s-model neuroprotection finding is real and interesting but is animal-model data that has not been shown to translate.15
Third, the long-term safety question is genuinely open, not merely under-advertised. Because every study has been short, no one has quantified the cancer risk, glucose-metabolism impact, or other long-latency effects of chronically raising IGF-1 in aging adults using sermorelin.8 Given the biology — IGF-1’s pro-proliferative role and the paradoxical longevity protection seen with reduced GH signaling — this is not a trivial gap. It is entirely possible that modest, physiological, pulsatile GH elevation is benign over years; it is also possible that it is not. The data to distinguish these do not exist.
Fourth, response is highly individual and confounded. Sermorelin’s effect depends on residual pituitary capacity, which varies widely; it is blunted by obesity, hyperglycemia, hypothyroidism, and glucocorticoids; and the natural age-related decline in the axis means older individuals may respond less than younger ones.38 This individual variability means population-level averages, even if favorable, translate unpredictably to any single person. Finally, much of what circulates as “sermorelin research” online is not primary literature at all but vendor content, anecdote, and repackaged marketing — a low-quality information environment that makes the genuine evidence gap easy to overlook.
Regulatory Status: Not Currently FDA-Approved
The regulatory status of sermorelin is frequently the most distorted element of online discussion, so it deserves an unambiguous statement. There is no FDA-approved sermorelin product available in the United States today. The molecule was approved decades ago and is not approved now, and the two facts are routinely conflated to imply a legitimacy that the current product does not have.34
To restate the timeline precisely: sermorelin acetate received FDA approval as Geref for diagnostic use in 1990 and for treatment of pediatric idiopathic growth hormone deficiency in 1997. In 2008 the manufacturer voluntarily discontinued the product and requested withdrawal of the New Drug Applications, and the FDA withdrew approval effective in 2009. In 2013 the FDA published a Federal Register determination that Geref had not been withdrawn for reasons of safety or effectiveness — a technical finding that is often misquoted as an endorsement.4 It is not an endorsement; it is a statement that the withdrawal was commercial, which in turn opened the door for the drug to be legally compounded.
Today sermorelin reaches people through two channels, neither of which is an approved consumer drug. The first is pharmacy compounding: a licensed prescriber can order sermorelin for a specific patient, and a compounding pharmacy prepares it under the compounding provisions of federal law. Compounded drugs are not FDA-approved as such — the agency does not review them for safety, efficacy, or manufacturing quality the way it does approved products — and their use for anti-aging and wellness indications is off-label and outside sermorelin’s ever-approved uses. The second channel is the research-chemical market, where sermorelin is sold explicitly for laboratory research and labeled not for human consumption. Material in this channel is not intended, tested, or legal for use in people.5
It is also worth situating sermorelin against its regulatory cousins. Among GHRH analogs, only tesamorelin currently holds FDA approval, and that approval is narrow: reduction of excess visceral abdominal fat in patients with HIV-associated lipodystrophy. It is not approved for aging, general body composition, cognition, or wellness. CJC-1295 (with or without DAC) and the ghrelin-mimetic secretagogues such as ipamorelin have no FDA approval at all and exist purely as research compounds. In sports contexts, GHRH analogs including sermorelin are prohibited by the World Anti-Doping Agency as growth-hormone secretagogues, which is a further reason their status is not equivalent to that of an approved medicine.14
For readers navigating this space, the practical bottom line is to treat regulatory status as a primary filter on any claim. A molecule can be biologically active, historically approved, and widely discussed and still not be an approved, quality-assured therapy today — sermorelin is exactly that case. DosagePeptide.com’s broader peptide dosage reference hub presents these compounds consistently within a research-and-education frame for that reason: the site is describing what the literature says about research chemicals, not recommending unapproved drugs for human use.
Frequently Asked Questions
Is sermorelin FDA-approved?
Not currently. Sermorelin acetate was FDA-approved as Geref for diagnostic use in 1990 and for pediatric growth hormone deficiency in 1997, but the manufacturer voluntarily withdrew it in 2008 and the FDA withdrew approval in 2009. The withdrawal was for commercial, not safety or efficacy, reasons — but the practical result is that there is no FDA-approved sermorelin product on the U.S. market today.34 It exists only as a compounded prescription drug (which is not FDA-approved as such) or as a research chemical labeled not for human use.
Does sermorelin actually raise growth hormone in older adults?
Yes, in the narrow biochemical sense this is well established. Controlled studies in older adults, including Corpas et al. (1992) and Khorram et al. (1997), showed that GHRH(1–29) administration increases GH secretion and raises IGF-1 toward more youthful levels, provided the pituitary is still functional.1012 What remains unproven is whether these hormonal changes produce meaningful, durable improvements in strength, function, or health outcomes.
Can sermorelin reverse aging or regenerate tissue?
There is no controlled human evidence for that claim. GH and IGF-1 participate in repair processes, and short trials show surrogate signals like increased skin thickness, but no randomized trial demonstrates that sermorelin regenerates organs, reverses sarcopenia functionally, or slows biological aging.12 Neuroprotective effects have been seen in animal models but not confirmed in humans.15 “Regeneration” is a marketing extrapolation, not an established outcome.
How is sermorelin different from HGH injections?
HGH injections deliver growth hormone directly, bypassing the body’s regulation and risking sustained supraphysiologic levels. Sermorelin instead stimulates the pituitary to release its own GH through the GHRH receptor, so output remains subject to somatostatin feedback and the natural pulsatile pattern.15 This makes grossly excessive GH levels harder to reach, which is a genuine theoretical safety difference — but it also means the effects are more modest, and it does not eliminate the concerns that come with raising IGF-1.
How does sermorelin compare to tesamorelin and CJC-1295?
All three act at the same GHRH receptor but differ in stability. Sermorelin is the shortest-acting (half-life ~11–12 minutes). CJC-1295 without DAC roughly doubles that; CJC-1295 with DAC extends it to days via albumin binding. Tesamorelin is a stabilized full-length analog and the only one with current FDA approval, limited to HIV-associated lipodystrophy.914 None except tesamorelin’s narrow indication is approved for use in the general or aging population.
What are the known side effects of sermorelin?
The most common are mild and local: injection-site redness, swelling, pain, or itching. Systemic effects reported in the clinical literature include flushing, headache, nausea, dizziness, and altered taste, generally at low frequency.916 The more serious theoretical concern is that any therapy raising IGF-1 could influence cell proliferation, which is why active cancer is a standard contraindication and why long-term safety in aging adults remains unquantified.8
Why is sermorelin sold as a “research chemical”?
Because it has no FDA-approved consumer form. With the branded drug withdrawn, sermorelin is legally available only as a compounded prescription or as material sold for laboratory research and explicitly labeled not for human consumption. Research-grade material is not tested or approved for safety, purity, or human use, and purity and labeling accuracy in that market are unregulated — a real-world risk separate from the molecule’s own pharmacology.5
Is the evidence strong enough to recommend sermorelin for anti-aging?
No. The efficacy data are small, old, short in duration, and focused on surrogate markers rather than the functional outcomes that would justify an anti-aging recommendation, and long-term safety is unestablished.12 Sermorelin reliably raises GH and IGF-1, which is a real biochemical effect, but that is a long way from evidence that it makes aging adults healthier, and no large modern trial has bridged that gap.
References
- Ishida J, Saitoh M, Ebner N, et al. Growth hormone secretagogues: history, mechanism of action, and clinical development. JCSM Rapid Communications. 2020;3(1):25–37. onlinelibrary.wiley.com/doi/full/10.1002/rco2.9
- Frokjaer S, Otzen DE. Protein drug stability: a formulation challenge. Nat Rev Drug Discov. 2005;4(4):298–306. pubmed.ncbi.nlm.nih.gov/15803194
- Prakash A, Goa KL. Sermorelin: a review of its use in the diagnosis and treatment of children with idiopathic growth hormone deficiency. BioDrugs. 1999;12(2):139–157. pubmed.ncbi.nlm.nih.gov/18031173
- U.S. Food and Drug Administration. Determination That GEREF (Sermorelin Acetate) Injection Were Not Withdrawn From Sale for Reasons of Safety or Effectiveness. Federal Register. March 4, 2013. federalregister.gov/documents/2013/03/04/2013-04827
- Walker RF. Sermorelin: a better approach to management of adult-onset growth hormone insufficiency? Clinical Interventions in Aging. 2006;1(4):307–308. pmc.ncbi.nlm.nih.gov/articles/PMC2699646
- Mayo KE, Godfrey PA, Suhr ST, Kulik DJ, Rahal JO. Growth hormone-releasing hormone: synthesis and signaling. Recent Prog Horm Res. 1995;50:35–73. pubmed.ncbi.nlm.nih.gov/7740167
- Van Cauter E, Plat L, Copinschi G. Interrelations between sleep and the somatotropic axis. Sleep. 1998;21(6):553–566. pubmed.ncbi.nlm.nih.gov/9779514
- Garcia JM, Merriam GR, Kargi AY. Growth Hormone in Aging. In: Endotext. NCBI Bookshelf, NBK279163. ncbi.nlm.nih.gov/books/NBK279163
- Sermorelin: pharmacology, pharmacokinetics, mechanism of action, and adverse effects. DrugBank Online, accession DB00010. go.drugbank.com/drugs/DB00010
- Corpas E, Harman SM, Piñeyro MA, Roberson R, Blackman MR. Growth hormone (GH)-releasing hormone-(1-29) twice daily reverses the decreased GH and insulin-like growth factor-I levels in old men. J Clin Endocrinol Metab. 1992;75(2):530–535. pubmed.ncbi.nlm.nih.gov/1379256
- Vittone J, Blackman MR, Busby-Whitehead J, et al. Effects of single nightly injections of growth hormone-releasing hormone (GHRH 1-29) in healthy elderly men. Metabolism. 1997;46(1):89–96. sciencedirect.com/science/article/pii/S0026049597901748
- Khorram O, Laughlin GA, Yen SS. Endocrine and metabolic effects of long-term administration of [Nle27]growth hormone-releasing hormone-(1-29)-NH2 in age-advanced men and women. J Clin Endocrinol Metab. 1997;82(5):1472–1479. academic.oup.com/jcem/article-abstract/82/5/1472
- Baker LD, Barsness SM, Borson S, et al. Effects of growth hormone-releasing hormone on cognitive function in adults with mild cognitive impairment and healthy older adults: results of a controlled trial. Arch Neurol. 2012;69(11):1420–1429. pubmed.ncbi.nlm.nih.gov/22869065
- Sinha DK, Balasubramanian A, Tatem AJ, et al. Beyond the androgen receptor: the role of growth hormone secretagogues in the modern management of body composition in hypogonadal males. Transl Androl Urol. 2020;9(Suppl 2):S149–S159. pmc.ncbi.nlm.nih.gov/articles/PMC7108996
- Growth hormone-releasing hormone attenuates amyloid deposition and neuroinflammation in Alzheimer’s disease models. Cell Death & Disease. 2026. nature.com/articles/s41419-026-08699-w
- Sermorelin (injection route): description, side effects, and dosage. Mayo Clinic. mayoclinic.org/drugs-supplements/sermorelin-injection-route
- Centers for Disease Control and Prevention. Questions about multi-dose vials (beyond-use dating and aseptic access). Injection Safety. cdc.gov/injection-safety/hcp/faqs/multidose-vials
Disclaimer: This article is provided for educational and research purposes only. It is not medical advice, and nothing in it should be interpreted as a recommendation to obtain, use, or administer sermorelin or any other peptide. Sermorelin is not an FDA-approved product; it is available only as a compounded prescription drug or as a research chemical labeled not for human consumption. It is not intended to diagnose, treat, cure, or prevent any disease. Growth hormone secretagogues carry real and incompletely characterized risks, and any decision involving them should be made only in consultation with a qualified, licensed healthcare professional who can evaluate an individual’s full medical context.