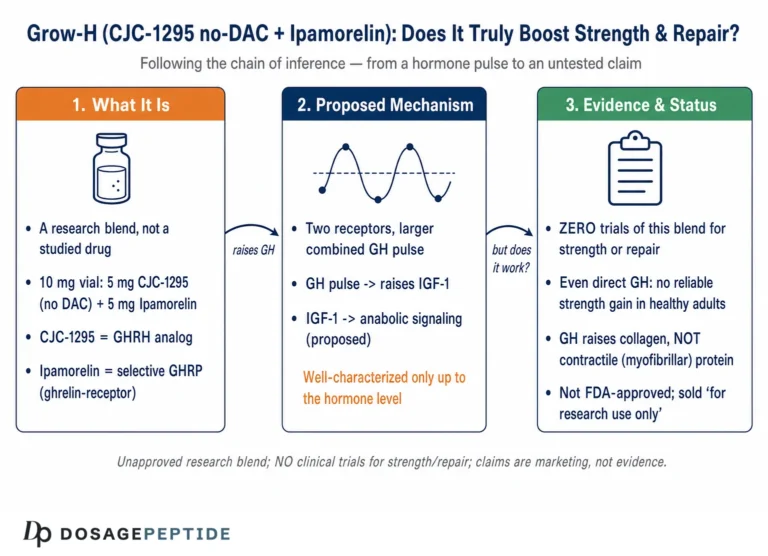
Grow-H is a marketing name for a two-component research peptide blend that pairs a growth-hormone-releasing hormone (GHRH) analog, CJC-1295 without DAC (also called modified GRF 1-29), with a selective growth-hormone secretagogue, ipamorelin. In its most common 10 mg presentation the vial is formulated as 5 mg of each peptide, and it is sold strictly as a research chemical rather than as a medicine. The central question researchers and educators keep returning to is deceptively simple: what does the current scientific literature actually establish about this specific combination, as opposed to what is claimed in vendor copy?
The honest answer is that the two individual peptides have a meaningful, if modest, published record, while the branded blend itself has essentially no dedicated controlled trials in humans. Nearly everything credible we can say about Grow-H is inferred from separate studies of CJC-1295 and ipamorelin, plus a broader body of endocrinology on how GHRH analogs and GH secretagogues behave when co-administered. That inferential chain is reasonable and mechanistically grounded, but it is not the same as direct evidence that “Grow-H” as a packaged product does what its listings imply.
This article walks through the evidence with that distinction front and center. It covers what the blend is and where its components originated, the receptor-level mechanism that motivates combining them, the actual level of proof behind each claim, comparisons with related compounds, the research models used, safety and tolerability signals, handling considerations in a laboratory context, the limitations that separate animal and short-term human data from clinical validation, and the regulatory reality that none of this is FDA-approved. Throughout, the aim is to neither dismiss nor oversell a compound that sits squarely in the investigational, preclinical-to-early-human category.
What Grow-H Is and Where Its Components Came From
Grow-H is not a single molecule. It is a fixed-ratio combination of two well-characterized research peptides, and understanding the blend requires understanding each part separately. The first component, CJC-1295 without DAC, is functionally identical to a fragment called modified GRF 1-29: a 29-amino-acid analog of endogenous human growth-hormone-releasing hormone. Native GHRH is a 44-residue hormone secreted by the hypothalamus, but its biological activity is concentrated in the first 29 amino acids. The “modified” version carries four amino-acid substitutions that protect it from rapid enzymatic breakdown by dipeptidyl peptidase-IV and related proteases, extending its functional window compared with the raw 1-29 fragment.3
The name CJC-1295 comes from the work of the biotechnology company ConjuChem, whose researchers described the underlying chemistry in a 2005 paper in Endocrinology. That study identified CJC-1295 as a long-lasting GRF analog and characterized how a Drug Affinity Complex (DAC) — a maleimido linker designed to bind covalently to circulating serum albumin — could extend the molecule’s plasma residence time from minutes to days.3 This is where a persistent point of confusion arises. “CJC-1295 with DAC” carries that albumin-binding linker and has a half-life measured in days. “CJC-1295 without DAC,” the form used in Grow-H, lacks the linker entirely and behaves like modified GRF 1-29, with a short half-life on the order of roughly 30 minutes. The two are pharmacologically distinct despite sharing a name, and evidence for one does not transfer cleanly to the other.
The second component, ipamorelin, comes from a different research lineage. It was first described by Raun and colleagues at Novo Nordisk in a 1998 paper in the European Journal of Endocrinology, where it was introduced as “the first selective growth hormone secretagogue.”1 Ipamorelin is a synthetic pentapeptide (Aib-His-D-2-Nal-D-Phe-Lys-NH2) that mimics the action of ghrelin at the growth-hormone secretagogue receptor. Its defining feature, established in that original work, was selectivity: it stimulated GH release in animal models without the meaningful spillover elevations in adrenocorticotropic hormone (ACTH), cortisol, or prolactin that characterized earlier secretagogues.1
| Attribute | CJC-1295 (no DAC) / Mod GRF 1-29 | Ipamorelin |
|---|---|---|
| Class | GHRH analog | GH secretagogue (ghrelin mimetic) |
| Receptor target | GHRH receptor (GHRH-R) | GHS-R1a (ghrelin receptor) |
| Structure | 29-amino-acid peptide, 4 substitutions | Pentapeptide |
| Approx. functional half-life | ~30 minutes | ~2 hours (reported range) |
| Typical vial share in Grow-H 10 mg | 5 mg | 5 mg |
| First key publication | Jetté et al., 20053 | Raun et al., 19981 |
The rationale for putting these two together is not arbitrary. GHRH analogs and GH secretagogues act on different receptors and, when combined, tend to produce a larger GH response than either alone.4 That physiological observation, which predates any commercial “Grow-H” product by decades, is the intellectual foundation of the blend. But it is worth stating plainly at the outset: the specific 5 mg + 5 mg fixed ratio, the branding, and the exact protocols circulated for the product are conventions of the research-chemical market, not outputs of a clinical development program. For readers who want the reconstitution and handling specifics, DosagePeptide maintains a dedicated CJC-1295 no DAC + ipamorelin (Grow-H 10 mg) protocol reference, framed explicitly for research use.
It is also worth being explicit about naming, because the research-chemical market is unusually loose with terminology and the confusion is not merely academic. “CJC-1295” is frequently used as a catch-all that lumps together the DAC and no-DAC forms, even though the Jetté 2005 paper reserved the name specifically for the tetrasubstituted, albumin-binding analog.3 Many vendors then apply the “CJC-1295” label to what is chemically modified GRF 1-29 — the same peptide backbone without the DAC linker. When a listing says “Grow-H contains CJC-1295 no DAC,” what it means, in strict pharmacological terms, is the short-acting modified GRF 1-29 fragment. This matters because the two forms have half-lives that differ by orders of magnitude, and the bulk of the citable human data attaches to the long-acting form. A reader who does not track this distinction will inevitably overestimate what is known about the blend, because they will unconsciously credit Grow-H with the multi-day pharmacokinetics that belong to a different molecule.23
The Molecular Mechanism: Two Receptors Converging on One Cell

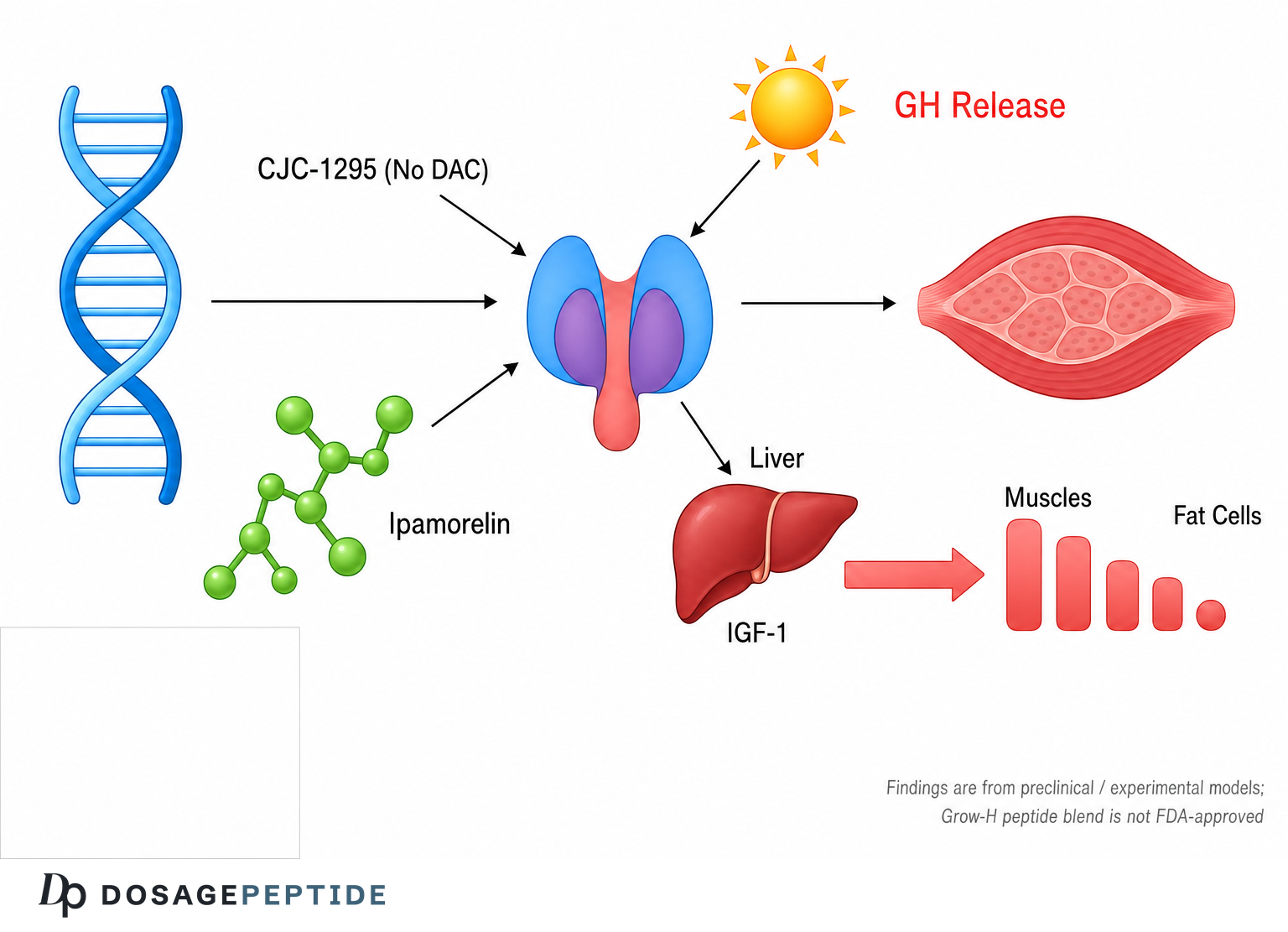
The mechanistic case for Grow-H rests on the biology of the somatotroph, the growth-hormone-producing cell of the anterior pituitary. Growth hormone secretion is governed by a push-pull system: GHRH from the hypothalamus stimulates GH synthesis and release, while somatostatin inhibits it, and the two forces oscillate to produce the characteristic pulsatile pattern of GH in healthy physiology. The two peptides in Grow-H each engage this system, but through separate receptors and separate intracellular pathways.
CJC-1295 without DAC acts as an agonist at the GHRH receptor (GHRH-R), a G-protein-coupled receptor expressed on somatotrophs. Binding activates the Gs protein, raises intracellular cyclic AMP, and engages the protein kinase A (PKA) cascade.5 The downstream effect is twofold: it promotes transcription and synthesis of new growth hormone, effectively “loading” the cell, and it stimulates release of stored GH. Because the no-DAC form is short-acting, its signal is a relatively brief, GHRH-like pulse rather than the prolonged elevation seen with the albumin-bound DAC version.3
Ipamorelin acts on a completely different receptor, the growth-hormone secretagogue receptor type 1a (GHS-R1a), which is the endogenous receptor for ghrelin. This receptor couples to the Gq protein and phospholipase C, driving inositol trisphosphate production and a rise in intracellular calcium.14 The calcium signal triggers release of GH from the primed cell. Ghrelin-receptor agonists like ipamorelin also appear to blunt somatostatin tone to a degree, effectively lifting the brake on GH secretion while GHRH steps on the accelerator.
This is the crux of the synergy argument. Because the two peptides converge on the same somatotroph through independent, non-competing pathways — cAMP/PKA from GHRH-R and calcium/PLC from GHS-R1a — their combined effect on GH output is generally reported as greater than additive rather than merely the sum of each.4 One agent primes and fills the cell with releasable GH; the other maximizes the release event. The literature on GHRH-plus-secretagogue co-administration, which spans decades and multiple secretagogue molecules, consistently documents this amplified response.4
| Signaling feature | CJC-1295 no DAC (GHRH-R) | Ipamorelin (GHS-R1a) |
|---|---|---|
| G-protein coupling | Gs | Gq |
| Second messenger | cyclic AMP | Ca2+ / IP3 |
| Kinase pathway | PKA | PLC |
| Primary cellular action | GH synthesis + release (“priming”) | GH release (“triggering”) |
| Effect on somatostatin | Minimal direct effect | May attenuate somatostatin tone |
It is worth dwelling on why two pathways converging on the same cell would multiply rather than simply add. In classical signal-transduction terms, the cAMP/PKA arm activated by GHRH and the calcium/PLC arm activated by the ghrelin receptor are not redundant; they act at different steps of the secretion process. GHRH-driven cAMP not only mobilizes releasable GH but also up-regulates the transcription of the GH gene and of the somatotroph’s own machinery, including the GHS receptor itself, effectively sensitizing the cell to the secretagogue.5 The ghrelin-receptor arm, meanwhile, produces the sharp intracellular calcium transient that drives exocytosis of the primed granules. When both signals arrive together, the cell is both maximally loaded and maximally triggered, which is the mechanistic explanation for the supra-additive GH pulses documented across decades of GHRH-plus-secretagogue co-administration studies.4 This is why the combination is considered more than a convenience: the two peptides are not doing the same job twice, they are completing complementary halves of a single secretory event.
A second mechanistic point concerns the role of somatostatin, the inhibitory counterpart to GHRH. Endogenous GH pulsatility emerges from the interplay of GHRH surges and somatostatin withdrawal. Ghrelin-receptor agonists appear to act partly by functionally antagonizing somatostatin’s restraining influence on the somatotroph, which means ipamorelin may enlarge the GH pulse not only by directly triggering release but also by lifting the brake that would otherwise limit it.4 Because both Grow-H peptides are short-acting, however, the somatostatin system is not permanently overridden; it reasserts itself between pulses, allowing the natural oscillation to continue. This preservation of the feedback architecture is a theoretical advantage of a short-acting blend over interventions that clamp GH continuously high.
A crucial mechanistic nuance is that this system is designed to preserve pulsatility. Because ipamorelin and no-DAC CJC-1295 are both relatively short-acting, the combined signal is a pulse rather than a continuous flood of GH. This matters because chronic, non-pulsatile GH elevation is physiologically abnormal and is one of the concerns with any secretagogue approach. In animal models the selectivity of ipamorelin means the GH pulse is not accompanied by proportionate spikes in cortisol or prolactin, which distinguishes it from older peptides such as GHRP-6 and GHRP-2.1 Readers exploring the individual pharmacology can consult the DosagePeptide ipamorelin protocol guide and the CJC-1295 no DAC single-peptide reference for component-level detail. It bears repeating that all of this mechanistic reasoning describes what should happen based on receptor biology; it is the hypothesis the blend is built on, not proof of a clinical outcome.
What the Evidence Actually Shows — and at What Level
Being precise about evidence level is the most important thing this article can do. It is tempting to read “there are published studies on CJC-1295 and ipamorelin” as “Grow-H is evidence-based,” but those are very different statements. Here is the evidence, sorted honestly by strength.
The strongest single piece of human data touches the wrong version of CJC-1295. The most-cited human trial in this space is Teichman and colleagues’ 2006 study in the Journal of Clinical Endocrinology & Metabolism. In healthy adults, single subcutaneous injections of CJC-1295 produced dose-dependent increases in mean GH concentrations of roughly 2- to 10-fold and IGF-1 increases of about 1.5- to 3-fold, with elevations sustained for days.2 This is legitimate, placebo-controlled human evidence — but it studied CJC-1295 with DAC, the long-acting albumin-binding form, not the no-DAC form used in Grow-H. The sustained multi-day elevation is precisely a property of the DAC linker. It cannot be assumed to describe the short-acting molecule in the blend.23
Ipamorelin’s foundational evidence is preclinical. The Raun 1998 characterization — establishing GH-releasing potency and the selectivity that spared ACTH, cortisol, and prolactin — was performed in in-vitro pituitary preparations and in animal models (swine and rats).1 That is high-quality preclinical work, but it is animal and cell-based, not a demonstration of long-term outcomes in humans. Ipamorelin has been examined in some early human contexts (for example, exploratory work on postoperative gut motility conducted by its original developer), but it was never advanced to approval for any indication, and there is no robust human body-composition or performance literature to draw on.
The bioconjugate chemistry is well established. The Jetté 2005 Endocrinology paper rigorously documented how CJC-1295’s structure activates the GRF receptor and how the DAC extends half-life in rats.3 Again, this is solid but preclinical, and it primarily concerns the DAC form.
The blend itself has essentially no dedicated controlled trials. Searching the primary literature and clinical-trial registries does not surface a registered, peer-reviewed randomized controlled trial of the specific CJC-1295-no-DAC-plus-ipamorelin combination — let alone one of a product marketed as “Grow-H.” What exists is the mechanistic expectation of synergy from the broader GHRH-plus-secretagogue literature.4 That expectation is reasonable, but “mechanistically expected” is a lower tier of evidence than “demonstrated in a trial.”
| Claim about Grow-H | Best available evidence | Evidence level |
|---|---|---|
| Each peptide raises GH in the expected direction | Raun 1998 (ipamorelin, animal); Teichman 2006 (CJC DAC, human) | Preclinical + early human (component-level) |
| Combining GHRH analog + secretagogue amplifies GH release | Broad GHRH+GHS co-administration literature4 | Mechanistic / class-level |
| Ipamorelin is selective (spares cortisol/prolactin) | Raun 19981 | Preclinical (in vitro + animal) |
| The no-DAC CJC form gives sustained multi-day GH | Not supported — Teichman studied the DAC form2 | Not established for this form |
| “Grow-H” product improves body composition in humans | No dedicated controlled trial identified | Not established |
It is instructive to consider what a genuinely evidence-based endorsement of Grow-H would require, because the gap between that standard and what exists is the whole story. It would require, at minimum, a randomized, placebo-controlled human trial of the exact blend at defined doses, with pre-registered endpoints that are actual outcomes rather than biomarkers — measured changes in lean mass, fat mass, recovery metrics, or sleep architecture — alongside systematic safety monitoring over a meaningful duration. It would ideally be replicated by an independent group, and it would use characterized, purity-verified peptide rather than research-market material of unknown content. None of these conditions is met for Grow-H. What we have instead is a chain of plausible inferences: ipamorelin releases GH selectively in animals; CJC-1295 (in its DAC form) raises GH and IGF-1 in humans; GHRH analogs and secretagogues synergize acutely; therefore the blend “should” raise GH. Each link is individually defensible, but a chain of plausible inferences is not the same as a demonstrated result, and it is precisely the kind of reasoning that controlled trials exist to test — and frequently overturn.124
There is also a temporal problem with the evidence that is easy to miss. The foundational papers date to 1998 and 2005 for the components, and the key human trial to 2006.123 In the roughly two decades since, these specific molecules have not accumulated the follow-on clinical literature one would expect if they were advancing toward real therapeutic use. That relative silence is itself informative: it suggests the peptides stalled at the investigational stage rather than progressing, which is the ordinary fate of most candidate compounds. Reading a sparse, aging evidence base as “established science” inverts what the sparseness actually implies.
The takeaway is not that Grow-H is fraudulent or that its components do nothing — the receptor pharmacology is real and the GH-raising direction of effect is well supported. The takeaway is that the evidence supporting the branded blend is indirect, largely preclinical, partly derived from a different (DAC) molecule, and entirely lacking the controlled human outcome trials that would justify claims about physique, recovery, anti-aging, or disease. Anyone citing “current research” to endorse Grow-H is, in practice, citing research on its parts and extrapolating.
How Grow-H Compares With Related Compounds
Placing Grow-H alongside its relatives clarifies both what makes the blend distinctive and where the honest boundaries of its evidence sit. The comparison spans other GHRH analogs, other secretagogues, and other popular blends.
Versus CJC-1295 with DAC. The most important comparison is internal to the CJC-1295 family. The DAC form binds albumin and produces a “GH bleed” — a sustained, days-long elevation of GH and IGF-1.2 The no-DAC form in Grow-H is short-acting and produces discrete pulses. Proponents of the no-DAC approach argue that preserving pulsatility is more physiological and avoids the abnormal continuous elevation; proponents of the DAC form point to the convenience of infrequent dosing and the direct human PK data from Teichman 2006.2 Neither position is settled by outcome trials in Grow-H’s use context. DosagePeptide maintains a separate CJC-1295 DAC protocol reference for those examining the long-acting variant.
Versus tesamorelin. Tesamorelin is the single most instructive comparator because it is a GHRH analog that actually completed the regulatory path. It is FDA-approved (as Egrifta) for the reduction of excess visceral abdominal fat in adults with HIV-associated lipodystrophy, with a newer F8 formulation approved in 2025.6 Tesamorelin demonstrates what a fully evidenced GHRH analog looks like: multiple large randomized controlled trials, a defined indication, a known safety profile, and regulatory oversight. Grow-H’s components have none of that. The comparison is not meant to imply Grow-H would fail such trials — only to show the enormous gap between an approved GHRH analog and a research-chemical blend.
Versus older GHRPs (GHRP-2, GHRP-6, hexarelin). Ipamorelin’s main advantage over these earlier secretagogues is selectivity. GHRP-2 and GHRP-6 reliably raise GH but also stimulate ACTH, cortisol, and prolactin, and GHRP-6 in particular provokes strong appetite via ghrelin-like signaling.1 Ipamorelin’s cleaner profile in the Raun data is the reason it is often preferred in a blend intended to raise GH without collateral hormonal noise.1
Versus MK-677 (ibutamoren). MK-677 is an orally active, long-acting secretagogue. Unlike ipamorelin, it produces a sustained, non-pulsatile increase in GH and IGF-1 and has been studied in humans over months, including data on increased appetite, fluid retention, and transient insulin resistance. The trade-off is exactly the pulsatility question: MK-677’s convenience comes with continuous elevation, whereas the Grow-H approach aims to keep the signal pulsatile.
| Compound | Class | GH pattern | Regulatory status |
|---|---|---|---|
| Grow-H (CJC no-DAC + ipamorelin) | GHRH analog + GHS blend | Pulsatile | Research chemical, not approved |
| CJC-1295 with DAC | GHRH analog (long-acting) | Sustained (days) | Research chemical, not approved |
| Tesamorelin | GHRH analog | Restores pulsatile GH | FDA-approved (HIV lipodystrophy)6 |
| GHRP-2 / GHRP-6 | GH secretagogue | Pulsatile, less selective | Research chemical, not approved |
| MK-677 (ibutamoren) | Oral GH secretagogue | Sustained | Investigational, not approved |
Read as a group, these comparisons tell a consistent story. Grow-H occupies a mechanistically sensible niche — a selective secretagogue paired with a short-acting GHRH analog to produce amplified but still pulsatile GH release — but it sits on the unapproved, research-only side of a bright line, while the one member of the family that crossed into approval (tesamorelin) did so only after the kind of rigorous human trials that Grow-H has never undergone.6 A broader catalog of these paired peptides is indexed on the DosagePeptide peptide blends overview.
Research Models and Methodology Behind the Data
To weigh the evidence fairly, it helps to understand how the underlying studies were actually conducted, because methodology determines how far a result can be generalized. The Grow-H evidence base draws on three broad model types: in-vitro pituitary systems, animal models, and a small number of controlled human studies of the individual components.
In-vitro pituitary preparations. The earliest and most mechanistic evidence for ipamorelin came from isolated rat pituitary cells, where GH release could be measured directly in response to graded peptide concentrations.1 This kind of model is powerful for establishing potency, efficacy, and receptor selectivity because it removes confounding whole-body variables. It was in such systems, combined with receptor-binding assays, that ipamorelin’s affinity for the GHS receptor and its EC50 for GH release were quantified.1 The limitation is obvious: a dish of pituitary cells cannot tell you what happens to a whole organism’s body composition, recovery, or long-term hormonal axis.
Animal models. The Raun characterization of ipamorelin and the Jetté characterization of CJC-1295 both leaned heavily on rodent and swine models.13 Animal work allows measurement of in-vivo GH pulses, pharmacokinetics, and the critical selectivity endpoints — whether ACTH and cortisol rise alongside GH. In the ipamorelin data, doses far above the GH-releasing threshold still failed to drive proportionate cortisol or prolactin release, which is the basis of the “selective secretagogue” description.1 The Jetté work in rats established that the albumin-bioconjugate strategy actually extended plasma residence time and maintained GRF-receptor activation, identifying CJC-1295 as the lead long-acting analog.3 Animal models bridge the gap between cells and humans but still require caution: dosing, metabolism, and receptor distribution differ across species.
Controlled human studies. The Teichman 2006 trial is the methodological high point of the whole area. It used a randomized, double-blind, placebo-controlled, ascending-dose design in healthy adults aged 21 to 61, with one arm examining single doses over 28 days and another examining repeated weekly or biweekly dosing over 49 days.2 Endpoints were objective and quantitative: serial GH concentrations, IGF-1 levels, and safety monitoring. This is exactly the design that gives a result credibility — but, as emphasized earlier, it studied the DAC form.2
| Model type | What it can establish | What it cannot establish |
|---|---|---|
| In-vitro pituitary cells | Potency, receptor selectivity, EC50 | Whole-body outcomes, long-term effects |
| Animal (rat, swine) | In-vivo GH pulses, PK, cortisol/prolactin selectivity | Direct human dose translation |
| Controlled human trial | Human GH/IGF-1 response, safety signals | Effects of the exact blend (none tested) |
A further methodological subtlety is that even the human data used dosing and endpoints that do not map neatly onto how Grow-H is actually handled in practice. The Teichman trial administered single or infrequent doses of a long-acting compound and tracked GH and IGF-1 as pharmacodynamic markers over defined windows.2 That is a clean way to characterize a molecule’s pharmacology, but it tells you little about the effect of frequent, short-acting pulsatile dosing of a two-peptide blend sustained over months, which is the pattern the product is marketed around. When the studied protocol and the real-world protocol diverge this much, generalizing from one to the other introduces error that no amount of methodological rigor in the original study can correct. The rigor lives in the component papers; it does not automatically travel to the blend.
The methodological lesson for Grow-H specifically is that the research pyramid narrows sharply as it approaches the actual product. There is a broad base of in-vitro and animal work on the components, a thin layer of human data on adjacent molecules, and an empty apex where a trial of the blend itself should be. Sound methodology in the component studies does not retroactively validate an untested combination product; it only supports the plausibility of the mechanism. Any responsible reading treats the animal and in-vitro findings as hypothesis-generating for the blend, not as confirmation of it.
Safety and Tolerability Signals
Because Grow-H has never been through a dedicated safety trial, its tolerability profile is assembled from the component literature and from the known class effects of GHRH analogs and GH secretagogues. This is inherently incomplete, and it should be read as “what is reported for the parts” rather than “what is proven safe for the blend.”
Injection-site reactions are the most consistently documented issue across GHRH-analog research. In the controlled CJC-1295 human data, localized reactions — transient pain, erythema, induration, and swelling at the subcutaneous injection site — were among the adverse events attributed to the peptide, generally mild and self-limiting.2 These are typical of subcutaneous peptide administration and are technique-dependent.
Vasomotor effects such as transient facial flushing and a feeling of warmth are recognized GHRH-analog class effects, attributable to vasodilation, and they tend to be dose-related and to diminish with repeated exposure. Water retention, mild peripheral edema, and joint discomfort or transient paresthesia are the classic downstream effects of raising GH and IGF-1, seen across GH-axis interventions generally and reported with secretagogue use.
Ipamorelin’s selectivity is the notable positive signal. The defining finding of the Raun work was that ipamorelin raised GH without meaningfully raising ACTH, cortisol, or prolactin, even at doses well above the GH-releasing threshold.1 This selectivity is why ipamorelin is generally described as better tolerated than older GHRPs like GHRP-6, which drive strong hunger, or GHRP-2, which more readily elevates cortisol and prolactin.1 In a blend, using ipamorelin rather than a less-selective secretagogue is a deliberate choice to minimize collateral endocrine effects — though this is an animal-model inference, not a human safety guarantee.
Metabolic considerations deserve honest flagging. Sustained elevation of GH and IGF-1 can, in principle, affect glucose handling and insulin sensitivity; GH is a counter-regulatory hormone. Interestingly, some controlled CJC-1295 data reported IGF-1 elevation without detectable increases in fasting glucose or HbA1c over the study window, but those windows were short.2 The theoretical concern that any therapy chronically raising IGF-1 could influence cellular proliferation is a reason the entire GH-axis field is studied cautiously, and it is one more argument against casual, unmonitored use.
| Reported effect | Likely source | Character |
|---|---|---|
| Injection-site reaction | Subcutaneous peptide delivery | Mild, transient, technique-dependent2 |
| Facial flushing / warmth | GHRH-analog vasodilation | Dose-related, tends to wane |
| Water retention / joint aches | Elevated GH/IGF-1 | Class effect of GH-axis stimulation |
| Hunger | Ghrelin-receptor activation | Milder with ipamorelin than GHRP-61 |
| Cortisol/prolactin rise | Non-selective secretagogues | Minimal for ipamorelin in animal data1 |
Two structural gaps in the safety picture deserve emphasis. First, essentially all of the reassuring signals come from short observation windows — days to a few weeks in the human component data, and acute-to-subacute timeframes in the animal work.12 Effects that emerge only with months or years of repeated GH-axis stimulation, which is how such a blend would realistically be used, are simply outside the evidence. Second, there are no data at all in the populations most likely to be affected by an intervention that raises IGF-1: individuals with a personal or family history of malignancy, those with impaired glucose tolerance, older adults, or anyone on interacting medications. The absence of harm signals in a small cohort of healthy young-to-middle-aged adults over a short window cannot be extrapolated to these groups. Responsible interpretation treats “no serious adverse events were reported in the component trials” as a narrow, provisional statement rather than a general safety endorsement.
The overriding safety caveat is that none of this constitutes a validated human safety profile for Grow-H. There are no long-term data, no data in special populations, and no data on the specific combined product. The relatively benign short-term signals from the component studies should not be mistaken for a clean bill of health for chronic, real-world, unsupervised use of the blend.
Handling and Reconstitution in a Research Context
Because Grow-H is supplied as a lyophilized (freeze-dried) powder, any laboratory work with it involves reconstitution, and the handling details materially affect both peptide integrity and the accuracy of any concentration-dependent measurement. This section is descriptive of standard research practice and is not dosing guidance for human use.
Lyophilized peptides are stable for extended periods when kept cold and dry, which is why vendors ship them freeze-dried.3 Reconstitution is typically performed with bacteriostatic water (sterile water containing 0.9% benzyl alcohol), which both dissolves the powder and provides a preservative that supports multi-day stability of the resulting solution under refrigeration. The bacteriostatic agent matters for any protocol where a single vial is sampled repeatedly over time.
Technique is important. Reconstitution water is usually introduced slowly against the inner wall of the vial rather than injected directly onto the peptide cake, because peptides can be shear-sensitive and violent mixing risks denaturation. The vial is then swirled gently, not shaken, until the solution clears. A cloudy or persistently particulate solution is a red flag for degradation or contamination.
Concentration math is where most handling errors occur. For a 10 mg Grow-H vial (5 mg CJC-1295 no DAC + 5 mg ipamorelin), the total peptide mass is fixed, and the reconstitution volume determines concentration. A common approach is to reconstitute with 2 to 3 mL of bacteriostatic water; 3 mL yields roughly 3,333 mcg of total peptide per milliliter, while 2 mL yields 5,000 mcg/mL. Because the two peptides are present in equal mass, each contributes half of any given total-peptide draw. Getting this arithmetic right is essential for reproducibility, and a reconstitution calculator reduces the risk of order-of-magnitude mistakes. A general primer on the process is available in the DosagePeptide peptide reconstitution guide.
| Reconstitution volume (10 mg vial) | Total peptide concentration | Per-component concentration |
|---|---|---|
| 2 mL bacteriostatic water | 5,000 mcg/mL | 2,500 mcg/mL each |
| 2.5 mL bacteriostatic water | 4,000 mcg/mL | 2,000 mcg/mL each |
| 3 mL bacteriostatic water | ~3,333 mcg/mL | ~1,667 mcg/mL each |
Storage after reconstitution follows standard peptide practice: refrigeration at approximately 2–8 °C, protection from light, and avoidance of repeated freeze-thaw cycles, which are particularly damaging to peptide structure. Unreconstituted lyophilized powder can typically be held in a freezer for long-term storage, while the reconstituted solution is used within a shorter window. Sterile technique throughout — alcohol-swabbing the stopper, using fresh needles, avoiding contact between the needle and non-sterile surfaces — is standard to prevent microbial contamination of a multi-use vial. These practices exist to protect the validity of research measurements; they are not an endorsement of self-administration, which falls entirely outside the intended research-only scope of the material.
Limitations and the Human-Evidence Gap
Everything above converges on a single, unavoidable limitation: there is a wide gulf between the evidence that exists and the claims commonly made about Grow-H. Naming that gap precisely is the whole point of an evidence-cautious treatment.
The blend has not been trialed as a blend. This is the foundational limitation. Synergy between GHRH analogs and secretagogues is well documented at the level of acute GH release, but “acute GH release goes up” is not the same as “the branded product produces the muscle, fat-loss, recovery, sleep, or anti-aging outcomes it is marketed for.” Those downstream outcomes have not been measured for this combination in a controlled human study.4
The best human data are on a different molecule. The Teichman trial’s impressive multi-day GH and IGF-1 elevations are a property of CJC-1295 with DAC.2 The no-DAC form in Grow-H is short-acting by design.3 Importing the DAC study’s numbers to describe Grow-H is a category error that appears frequently in marketing copy and should be resisted.
Component human data are thin and old. Ipamorelin’s core evidence is a 1998 animal and in-vitro characterization.1 Despite being described as a promising selective secretagogue, it was never carried to approval for any indication, which itself is informative — many mechanistically attractive peptides do not survive the transition to demonstrated clinical benefit and acceptable risk.
Surrogate endpoints are not outcomes. Even where GH and IGF-1 rise, those are biomarkers, not clinical benefits. A rise in IGF-1 is a pharmacodynamic signal; whether it translates into meaningful, durable, net-positive effects in healthy individuals — and at what risk — is a separate question the current literature does not answer for this blend.
Research-chemical quality is an uncontrolled variable. Peer-reviewed studies use characterized, purity-verified material. Product sold on the research-chemical market varies in purity, actual peptide content, and freedom from contaminants, and there is no regulatory guarantee that a given vial contains what the label states or is free of endotoxin. This variability alone makes it impossible to generalize even the component literature to any particular vial of Grow-H.
Publication and source bias. Much of the “evidence” circulating online originates from vendors with a commercial interest, not from independent investigators. Genuine primary sources are limited to the handful of peer-reviewed papers on the components.123 The asymmetry between the volume of marketing content and the volume of real data is itself a reason for skepticism. The intellectually honest position is that Grow-H is an investigational blend whose plausibility rests on solid receptor pharmacology and whose real-world efficacy and long-term safety in humans remain unproven.
Regulatory Status
The regulatory picture is unambiguous and is the single most important piece of context for the entire discussion. Neither Grow-H nor its individual components is approved by the U.S. Food and Drug Administration, or by comparable agencies, for human therapeutic use. The blend is sold and should be understood strictly as a research chemical — that is, “for research use only, not for human consumption.”
The contrast with tesamorelin makes the point vividly. Tesamorelin is a GHRH analog in the same broad pharmacological family, and it is FDA-approved — as Egrifta, for reducing excess visceral abdominal fat in adults with HIV-associated lipodystrophy, with a further formulation approved in 2025.6 The difference is not the receptor mechanism; it is that tesamorelin’s sponsor completed the required program of controlled clinical trials, manufacturing controls, and regulatory review. CJC-1295 and ipamorelin never did. Their unapproved status is therefore not a technicality — it reflects a genuine absence of the evidence and oversight that approval requires.6
There is also an anti-doping dimension. Both classes of molecule in Grow-H are explicitly prohibited in sport. The World Anti-Doping Agency’s Prohibited List, under section S2 (Peptide Hormones, Growth Factors, Related Substances, and Mimetics), names GHRH and its analogs — including CJC-1295 — and lists growth-hormone secretagogues and GH-releasing peptides such as ipamorelin among banned substances, prohibited at all times, both in and out of competition.7 The list also uses class-based “and related substances” language, so a compound need not be named individually to be prohibited if it acts similarly.7 For any athlete subject to testing, Grow-H’s components carry the strictest doping-control implications.
| Dimension | Grow-H components | Tesamorelin (for contrast) |
|---|---|---|
| FDA approval | None | Approved (HIV lipodystrophy)6 |
| Legal framing | Research chemical, not for human use | Prescription medicine |
| WADA status | Prohibited (S2)7 | Prohibited (S2)7 |
| Controlled human efficacy trials | None for the blend | Multiple RCTs |
In short, the regulatory status is fully consistent with the evidence status. A compound with no dedicated controlled trials, thin and dated component data, and a mechanism validated mainly in animals is exactly the kind of compound that remains unapproved and confined to the research-only category. Nothing in the current literature changes that, and any framing of Grow-H as a treatment, therapy, or approved product misrepresents both the science and the law.
Frequently Asked Questions
Is Grow-H FDA-approved for any use?
No. Neither the Grow-H blend nor its individual components — CJC-1295 without DAC and ipamorelin — is approved by the FDA for any human indication. It is sold strictly as a research chemical, labeled for research use only and not for human consumption. The only closely related GHRH analog that carries FDA approval is tesamorelin, a distinct molecule approved for a specific medical condition.6
What exactly is in a Grow-H vial?
The common 10 mg presentation contains two peptides in equal mass: 5 mg of CJC-1295 without DAC (a GHRH analog, functionally the same as modified GRF 1-29) and 5 mg of ipamorelin (a selective growth-hormone secretagogue).13 The two are combined because they act on different receptors and are expected to amplify GH release synergistically.4
Is there a clinical trial of the Grow-H blend itself?
No dedicated, registered, peer-reviewed randomized controlled trial of this specific combination product could be identified in the primary literature. The evidence base consists of separate studies of the individual peptides plus the broader endocrinology of combining GHRH analogs with secretagogues.124 Claims about the blend are inferred from its parts, not demonstrated for the whole.
Does the famous CJC-1295 human study apply to Grow-H?
Only partially, and with an important caveat. The most-cited human study, Teichman et al. 2006, showed dose-dependent, multi-day GH and IGF-1 elevations — but it studied CJC-1295 with DAC, the long-acting albumin-binding form.2 Grow-H uses the no-DAC form, which is short-acting.3 The sustained elevations in that trial are a feature of the DAC linker and should not be assumed to describe Grow-H.
Why is ipamorelin often described as “selective”?
In its original 1998 characterization, ipamorelin stimulated GH release in animal and in-vitro models without meaningfully raising ACTH, cortisol, or prolactin, even at doses well above the GH-releasing threshold.1 That selectivity distinguishes it from older growth-hormone-releasing peptides such as GHRP-2 and GHRP-6, which more readily elevate those other hormones.1 The finding, however, comes from preclinical models, not long-term human studies.
What are the reported side effects?
From the component and class literature, reported effects include mild, transient injection-site reactions, facial flushing or warmth from vasodilation, water retention and joint discomfort related to elevated GH/IGF-1, and hunger from ghrelin-receptor activation (milder with ipamorelin than with GHRP-6).12 These are drawn from studies of the parts; there is no validated human safety profile for the blend itself, and no long-term data.
Is Grow-H banned in sport?
Yes. Under the World Anti-Doping Agency Prohibited List, section S2, both GHRH analogs like CJC-1295 and growth-hormone secretagogues like ipamorelin are prohibited at all times, in and out of competition.7 The list’s class-based language also captures related substances that are not named individually. Any athlete subject to testing should treat Grow-H’s components as banned.
How is Grow-H handled in a research setting?
It ships as a lyophilized powder and is reconstituted with bacteriostatic water, typically 2 to 3 mL for a 10 mg vial, yielding a total-peptide concentration of roughly 3,333 to 5,000 mcg/mL with each component contributing half.3 Standard practice includes gentle swirling rather than shaking, refrigerated storage, protection from light, avoidance of freeze-thaw cycles, and sterile technique. These are laboratory handling practices, not instructions for human use.
References
- Raun K, Hansen BS, Johansen NL, et al. Ipamorelin, the first selective growth hormone secretagogue. Eur J Endocrinol. 1998;139(5):552-561. https://academic.oup.com/ejendo/article-abstract/139/5/552/6748390
- Teichman SL, Neale A, Lawrence B, et al. Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults. J Clin Endocrinol Metab. 2006;91(3):799-805. https://academic.oup.com/jcem/article-abstract/91/3/799/2843281
- Jetté L, Léger R, Thibaudeau K, et al. Human growth hormone-releasing factor (hGRF)1-29-albumin bioconjugates activate the GRF receptor on the anterior pituitary in rats: identification of CJC-1295 as a long-lasting GRF analog. Endocrinology. 2005;146(7):3052-3058. https://academic.oup.com/endo/article/146/7/3052/2500187
- Ishida J, Saitoh M, Ebner N, et al. Growth hormone secretagogues: history, mechanism of action, and clinical development. JCSM Rapid Communications. 2020;3(1):25-37. https://onlinelibrary.wiley.com/doi/full/10.1002/rco2.9
- Growth hormone-releasing hormone receptor (GHRH-R) and its signaling. National Center for Biotechnology Information, PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12137518/
- Theratechnologies Inc. FDA approval of EGRIFTA WR (tesamorelin, F8 formulation), 2025 — indicated for reduction of excess visceral abdominal fat in adults with HIV-associated lipodystrophy. https://www.theratech.com/news-releases/news-release-details/theratechnologies-receives-fda-approval-egrifta-wrtm-tesamorelin/
- World Anti-Doping Agency. The Prohibited List — S2: Peptide Hormones, Growth Factors, Related Substances and Mimetics. https://www.wada-ama.org/en/prohibited-list
Disclaimer: This article is provided for educational and research purposes only and does not constitute medical, clinical, or dosing advice. Grow-H and its components (CJC-1295 without DAC and ipamorelin) are unapproved research chemicals, are not FDA-approved for human use, and are not intended to diagnose, treat, cure, or prevent any disease. Nothing here should be interpreted as encouraging human administration. The available evidence is preclinical and limited, and no controlled human trial of the specific blend exists. Consult a qualified healthcare professional regarding any health-related decision, and comply with all applicable laws and anti-doping regulations.