Research-use-only. Not medical advice. This article is an educational overview of what published research has and hasn’t shown about peptide results. It does not recommend that anyone use any peptide, does not prescribe a dose, and is not a substitute for guidance from a qualified professional. The peptides discussed here are sold for laboratory and research use only and are not intended for human consumption.
Search any peptide plus “before and after” and you’ll get a wall of dramatic split-screen photos — glowing skin, healed shoulders, forty pounds gone. Here’s what almost none of them tell you: the lighting changed, the timeline is missing, and in most cases there’s no way to know what else the person was doing. This guide does the opposite. Instead of showing you photos, it shows you what the peer-reviewed research actually measured — how much, how fast, and how much of it is still unproven in humans — so you can tell a realistic expectation from a marketing fantasy.
The goal isn’t to talk you out of curiosity. It’s to hand you the same lens researchers use, so the next transformation photo you see gets weighed against evidence instead of against your hopes.

Why “before and after” peptide photos are almost impossible to trust
A photo feels like proof. It isn’t. A before-and-after pair is one of the weakest forms of evidence there is, because nearly every variable that actually determines a result is invisible in the frame. Before you read a single timeline below, it helps to see exactly what the image is hiding.
The five things a transformation photo never shows you
- Lighting, pump, and hydration. A different angle, warmer light, a flexed-and-pumped muscle, and a few hours of water manipulation can manufacture a “transformation” in a single afternoon — with no compound involved at all.
- Diet and training. The person may have overhauled their nutrition or started lifting the same week. There’s no way to separate the peptide’s contribution from everything else that changed.
- Other compounds. Many photos come from people running several things at once. Attributing the whole result to one peptide is a guess, not a finding.
- The real timeline. “Before” and “after” rarely carry dates. Six days and six months look identical in a JPEG.
- Cherry-picking. You’re seeing the one pair someone chose to post. You never see the people for whom nothing visible happened.
Anecdote vs. evidence — why a photo is not a study
A single case, however sincere, is an anecdote. A study is designed to strip out the confounders a photo leaves in: it uses a control group, a defined dose over a defined time, blinded and objective measurements, and enough participants that individual flukes wash out. That’s the entire difference. When research suggests a peptide “works,” it means a measured endpoint moved more than chance and more than the controls — not that one person looked different in two pictures. Throughout this guide, treat anecdote and evidence as two separate currencies that don’t convert into each other.
What the research actually measures (and what it can’t)
Scientists don’t photograph a result and call it a day — they quantify it. Understanding how they quantify it tells you what a realistic outcome even looks like.
Objective endpoints scientists use instead of photos
Depending on the peptide, researchers track things like percent change in body weight, collagen density measured on ultrasound, wrinkle depth from skin imaging, tendon load-to-failure or tissue integrity in mechanical testing, and blood biomarkers. These endpoints are chosen precisely because they can’t be faked with lighting. A number on an ultrasound or a scale is boring compared to a glowing selfie — and far more trustworthy. If a claim can’t be tied to an endpoint like these, it isn’t a research result; it’s a testimonial.
Preclinical (animal) vs. human clinical data — why the distinction changes everything
This is the single most important idea in the article, so it’s worth stating plainly: most striking peptide “before and after” narratives rest on animal studies, not human ones. A result in a rat is a genuine scientific signal — but it doesn’t mean the same thing will happen, at the same size, on the same timeline, or safely, in a person. Lab animals are often young, healthy, genetically uniform, dosed under tightly controlled conditions, and studied over short windows. Humans are none of those things. Every time you read a result below, notice whether it came from an animal model or a human clinical trial. That one word changes how much weight the finding can bear. When a term like agonist, reconstitution, or half-life comes up and you want a plain-English definition, our peptide glossary unpacks it.
Realistic timelines by peptide category
Different classes of peptide have completely different evidence bases and completely different clocks. Lumping them together is how hype spreads. Here’s what the research actually indicates, category by category — always framed as what studies measured, never as what any peptide “will” do for you.
Metabolic / GLP-1 class (retatrutide, semaglutide, tirzepatide)
This is the category with the strongest human clinical data — and, ironically, the one most misrepresented by “30-day transformation” posts. What the trials show is gradual and dose-titrated. Appetite and satiety changes can appear within the first week, but the scale moves slowly at first: real-world cohorts suggest only around 1% body-weight loss by roughly eight weeks, with meaningful loss building over three to six months and beyond.
The headline trial figures are large, but slow-earned. In the semaglutide STEP-1 trial (Wilding et al., NEJM 2021), participants lost an average of about 14.9% of body weight — but that was measured at 68 weeks. In the tirzepatide SURMOUNT-1 trial, average loss reached up to roughly 22.5% at 72 weeks on the highest dose. Retatrutide, a newer triple-agonist still in clinical development, is being studied on a similar gradual, dose-escalated arc. The honest framing: these are results measured over more than a year of steadily increased dosing, not overnight change.
If you want to understand how the three compare mechanistically, our companion piece — Retatrutide vs. Semaglutide vs. Tirzepatide GLP-1 comparison — lays out the landscape. This article names no doses on purpose; if your research reaches the stage of specifics, those live on the single-peptide dosage protocols (including the retatrutide protocol page), not here.
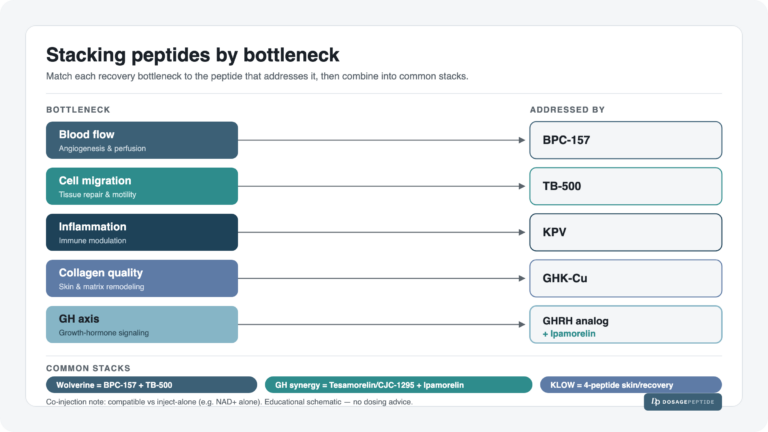
Repair / recovery class (BPC-157, TB-500, KLOW blend)
Here is where the gap between the internet narrative and the evidence is widest. BPC-157 has an enthusiastic “healed my tendon” reputation online, and the underlying research is genuinely interesting — but it is almost entirely from animal models. In rat studies, BPC-157 has been associated with improved tendon-to-bone integrity at around four weeks and biomechanical gains within roughly 10–14 days in tendon- and muscle-injury models. Those are real preclinical findings.
What they are not is proof of a human result. Systematic reviews of BPC-157 conclude that human clinical evidence remains very limited — largely case reports and case series rather than controlled trials. In other words: the dramatic recovery “before and afters” you see are extrapolated from rats, and the human data needed to confirm effect size, timeline, and safety in people simply hasn’t been produced yet. TB-500 (a synthetic thymosin beta-4 fragment) sits in a similar position — mechanistically plausible, studied preclinically, thin on human trials. The same caution applies to the KLOW blend, which combines these repair peptides with others: no such blend has been tested as a blend in a human trial.
If you’re researching how these are handled in research settings, the KLOW blend dosage protocol and the broader peptide blend protocols are where the specifics belong — not a photo.
Skin & cosmetic class (GHK-Cu / copper peptides)
GHK-Cu (a copper tripeptide) is the interesting exception: it’s the “money” peptide with the strongest human topical evidence, yet the real results are far more modest than the online split-screens imply. Controlled 12-week facial studies of topical copper-peptide creams — including work by Leyden and colleagues, in which a group of women applied a twice-daily facial cream — reported measurable improvements, such as an average increase of roughly 28% in skin collagen density on ultrasound, along with reductions in fine lines and wrinkle depth, with a companion study focused on the eye area. Pickart’s reviews summarize the broader mechanistic picture of collagen and remodeling outcomes.
Frame it honestly: this is incremental, topical, 12-week change measured by instruments — not the dramatic before/after a marketing page implies. It’s a genuine cosmetic signal, and it’s still not a transformation. It also says nothing about injectable or systemic use, which is a different question the topical trials didn’t test.
Growth-hormone-axis class (tesamorelin, sermorelin, ipamorelin)
Peptides in this group act on the growth-hormone axis, and the trial evidence varies a lot within the class. Tesamorelin has the most developed human data, studied in specific clinical populations over multi-month horizons with endpoints like change in visceral fat measured by imaging — again, gradual and measured over months, not weeks. Sermorelin and ipamorelin have thinner controlled human datasets. Across the whole category the pattern holds: where results exist, trials tracked them slowly and objectively, and any dramatic short-term “before and after” attributed to this class is running well ahead of what the studies documented.
The “realistic vs. fantasy” expectations table
This is the whole article in one screen. Read across each row: what studies actually measured, the realistic research timeline, how strong the evidence is, and the overpromise to distrust.
| Category | What studies measured | Realistic research timeline | Evidence strength | Common overpromise to distrust |
|---|---|---|---|---|
| Metabolic / GLP-1 (retatrutide, semaglutide, tirzepatide) |
% body-weight change; appetite/satiety | Satiety shifts in ~week 1; ~1% by ~8 weeks; ~15% (semaglutide, 68 wks) to ~22% (tirzepatide, 72 wks) at full dose over a year+ | Human RCTs (strong), but dose-titrated over months | “Lost 40 lbs in 30 days” — ignores the year-long titration |
| Repair / recovery (BPC-157, TB-500, KLOW) |
Tendon/tissue integrity, load-to-failure, angiogenesis | Animal-model gains at ~10–14 days to ~4 weeks; human timeline not established | Mostly animal models; human data limited to case reports | “Healed my rotator cuff in 2 weeks” — extrapolated from rats |
| Skin & cosmetic (GHK-Cu / copper peptides) |
Collagen density (ultrasound), wrinkle depth, fine lines | Incremental change over ~12 weeks of twice-daily topical use | Human topical trials (strongest of the cosmetic peptides), but modest | “Erased 10 years overnight” — real data is 12-week and subtle |
| Growth-hormone axis (tesamorelin, sermorelin, ipamorelin) |
Visceral fat (imaging), body-composition markers | Gradual, measured over multiple months; varies within the class | Tesamorelin has the most human data; others thinner | “Reversed aging in weeks” — trials tracked months |
Every figure above is a study average, not a promise. See the References section for the specific trials.
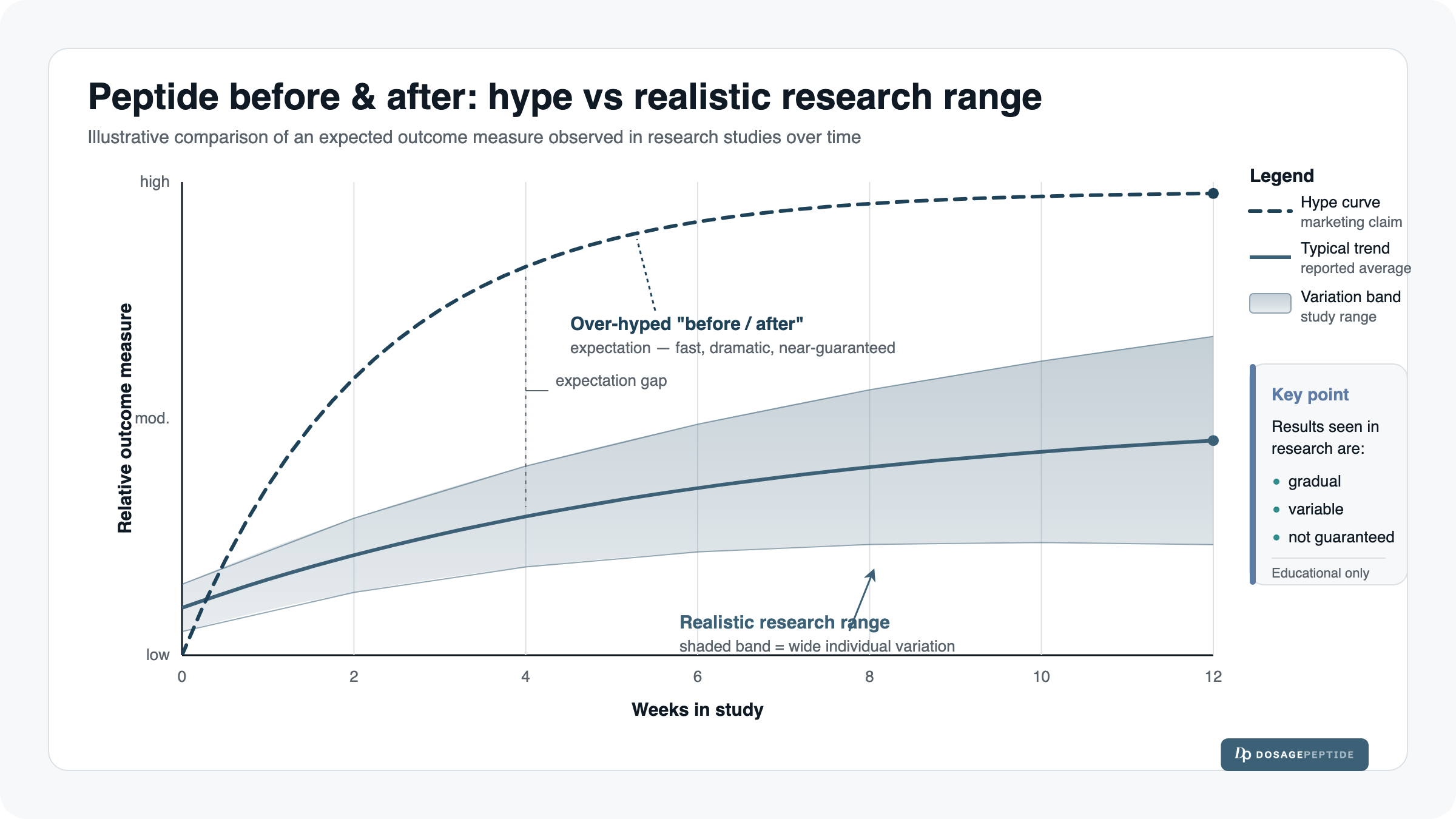
Why individual variation is the rule, not the exception
Even when a trial reports a clean average, that average is built from a wide spread of individual outcomes. Some participants far exceed it; some barely move; a few respond in the “wrong” direction. A published average is a description of a group under controlled conditions — it is emphatically not a forecast for any one person. This is the quiet truth behind both the impressive photos and the disappointed forum posts: both are real people at opposite ends of the same distribution.
Factors that move the result
- Baseline. Where someone starts — weight, skin condition, injury severity, age — heavily shapes how much change is even possible to observe.
- Adherence. Trials hit their numbers with strict, supervised consistency that real-world use rarely matches.
- Lifestyle. Diet, sleep, training, and stress interact with everything and are often the actual driver behind a photo.
- Sourcing and purity. Research-grade material varies; an impure or underfilled vial won’t behave like the compound used in a study.
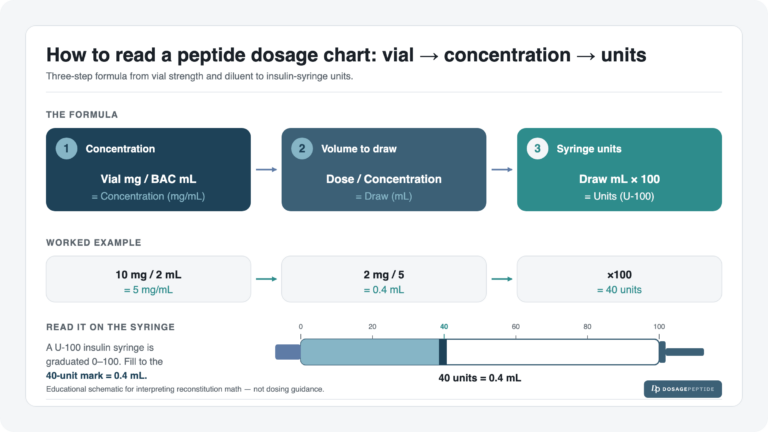
- Reconstitution accuracy. If the powder is mixed or measured incorrectly, the actual amount in a research dose can be far from intended — which shifts outcomes independent of the peptide itself. Getting this right is a real variable, which is why the mechanics matter: our peptide reconstitution guide walks through it, and the reconstitution dosage calculator takes the arithmetic off your hands.
Red flags: how to spot an overpromising before/after claim
You can screen most misleading content in about ten seconds. Be skeptical whenever you see:
- No timeline. If the post can’t tell you how long it took, it isn’t telling you anything.
- No diet or training disclosed. Silence on lifestyle usually means lifestyle did the heavy lifting.
- Only one photo pair. A single, curated before/after is the definition of cherry-picking.
- Visible lighting or pump changes. Different angle, warmer light, flexed muscle — instant fake transformation.
- “30 days” miracle framing. Real research timelines run in weeks-to-months for cosmetic effects and a year-plus for full metabolic results.
- No source study. A big claim with zero citation to a named trial.
- An affiliate incentive. If the person profits when you buy, weigh the photo accordingly.
If you’re going to research a peptide, do it methodically
Curiosity is fine; the fix for hype is method, not abstinence. That means starting from evidence rather than images: identify the category, find the actual human-versus-animal evidence for it, accept that timelines are long and variation is wide, and treat every “before and after” as a hypothesis to check, not a result to expect.
Where the actual numbers live
This article deliberately contains no doses — that’s not evasion, it’s the point. Numbers belong on the pages built to carry them responsibly. If your research reaches the stage of specifics, the single-peptide dosage protocols and peptide blend protocols are where they’re documented, the peptide reconstitution guide covers mixing, and the reconstitution dosage calculator handles the math. Terms you don’t recognize along the way live in the peptide glossary.
Frequently asked questions
How long do peptides take to “work”? It depends entirely on the category and the endpoint. Human GLP-1 trials measure appetite change in the first week but full weight results over a year or more of titration; cosmetic copper-peptide skin studies run about 12 weeks; repair-peptide evidence is mostly from short-window animal models with no established human timeline. There’s no single answer, and any source that gives you one is oversimplifying.
Are the dramatic before/after photos online fake? Not necessarily fabricated — but they’re uncontrolled and unverifiable. Even genuine photos can’t show diet, training, other compounds, the real timeline, or the people it didn’t work for. Treat them as anecdotes, never as evidence.
Which peptide has the most real human evidence for a visible result? Among commonly discussed “money” peptides, the GLP-1 metabolic class has the strongest human clinical trial data, and GHK-Cu has the strongest human topical cosmetic data — though its measured results are modest and incremental, not dramatic.
Why is BPC-157 singled out for caution? Because its strong “healing” reputation rests almost entirely on animal (rat) models, while systematic reviews confirm human clinical evidence is very limited. The mechanism is interesting; the human proof isn’t there yet.
Can I expect the trial average if I research a peptide? No. A trial average is a group result under controlled conditions and is not a promise for any individual. Baseline, adherence, lifestyle, purity, and reconstitution accuracy all shift real-world outcomes.
The bottom line
Peptide “before and after” content sells a feeling: instant, dramatic, guaranteed. The research tells a slower, humbler, more honest story — gradual metabolic change measured over a year in human trials, modest 12-week cosmetic gains from topical copper peptides, and a repair-peptide narrative that is still, for the most part, a story about rats. None of that means the science is uninteresting. It means the realistic expectation and the marketing fantasy are two very different things, and now you can tell them apart. When you see the next split-screen photo, ask the questions a researcher would: measured how, over how long, in animals or in humans, compared to what — and let the answer, not the image, set your expectations.
Research-use-only. Not medical advice. Nothing here recommends, prescribes, or endorses the use of any peptide, and no peptide “will” produce any specific result. All figures cited are study averages, not promises for any individual, and animal-model findings are not evidence of human outcomes. Products referenced are for laboratory and research use only and are not intended for human consumption. Consult a qualified professional before making any health decision.
References
- Wilding JPH, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP-1). New England Journal of Medicine. 2021;384(11):989–1002 (NEJMoa2032183). — Average weight loss ~14.9% at 68 weeks; gradual, dose-titrated timeline.
- Jastreboff AM, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). New England Journal of Medicine. 2022. — Weight loss up to ~22.5% at 72 weeks on the highest dose.
- Real-world GLP-1 cohort data indicating roughly 1% body-weight loss by about 8 weeks, illustrating the early, gradual phase of response.
- BPC-157 preclinical tendon and myotendinous-junction studies in rat models — e.g., Biomedicines 2021;9(11):1547 (PMC8615275) — reporting biomechanical and tissue-integrity gains over short windows.
- Systematic review of BPC-157 confirming that human clinical evidence remains very limited (case reports/series) — “Regeneration or Risk?” (PMC12446177).
- Leyden J, et al. 12-week topical copper-peptide (GHK-Cu) facial and eye-area clinical studies reporting increased collagen density on ultrasound (~28% average) and reduced wrinkle depth/fine lines.
- Pickart L, Margolina A. Regenerative and mechanistic reviews of GHK / GHK-Cu skin and collagen outcomes (PMC4508379; PMC6073405).
- Evidence-hierarchy principle: controlled, blinded, endpoint-based studies outrank uncontrolled before/after photographs, because a control group and objective measurement remove the confounders a single image cannot.