The title of this article asks how “NAD+ 500mg” influences cellular damage repair and longevity in human studies, and the honest place to begin is by taking that question apart, because it packs several assumptions into a tidy-sounding phrase. It implies, first, that there is an established human dose of NAD+ — 500 mg — that people take; second, that this dose measurably repairs cellular damage; and third, that doing so extends human lifespan or healthspan in a way that clinical trials have shown. None of those three implications survives contact with the actual literature intact. NAD+ (nicotinamide adenine dinucleotide) is one of the most important molecules in all of biology, and the case that its age-related decline contributes to cellular ageing is genuinely strong. But the leap from that mechanistic story to “take 500 mg and repair your cells and live longer” is exactly where preclinical enthusiasm outruns human evidence.
So this piece treats the title as an open research question rather than a settled claim. We will look at what NAD+ is, why it falls with age, and the elegant biochemistry that connects it to DNA repair, sirtuin signalling, and mitochondrial function — the machinery of “cellular damage repair.” Then we will confront the awkward facts that most human data concern the precursors nicotinamide riboside (NR) and nicotinamide mononucleotide (NMN) rather than NAD+ itself; that raising blood NAD+ is easy and reproducible while changing hard outcomes has proven difficult; and that not a single randomized controlled trial has demonstrated that any NAD+-boosting regimen extends human lifespan or reverses ageing.3 NAD+ and its precursors are sold as dietary supplements, not approved as drugs for repair or longevity, and the gap between the marketing and the data is one of the widest in the whole supplement field.
This article is written for researchers and scientifically literate readers who want an accurate map of what is known, what is merely plausible, and what is simply hype. The guiding posture is restraint: the biology is fascinating and the decline is real, but curing ageing with a capsule remains, as of mid-2026, an unproven hypothesis.
Reframing the Question: What “NAD+ 500mg” Actually Means
Before evaluating efficacy, it is worth being precise about what someone is even referring to when they say “NAD+ 500 mg,” because the phrase conflates at least three distinct things that behave very differently in the body.
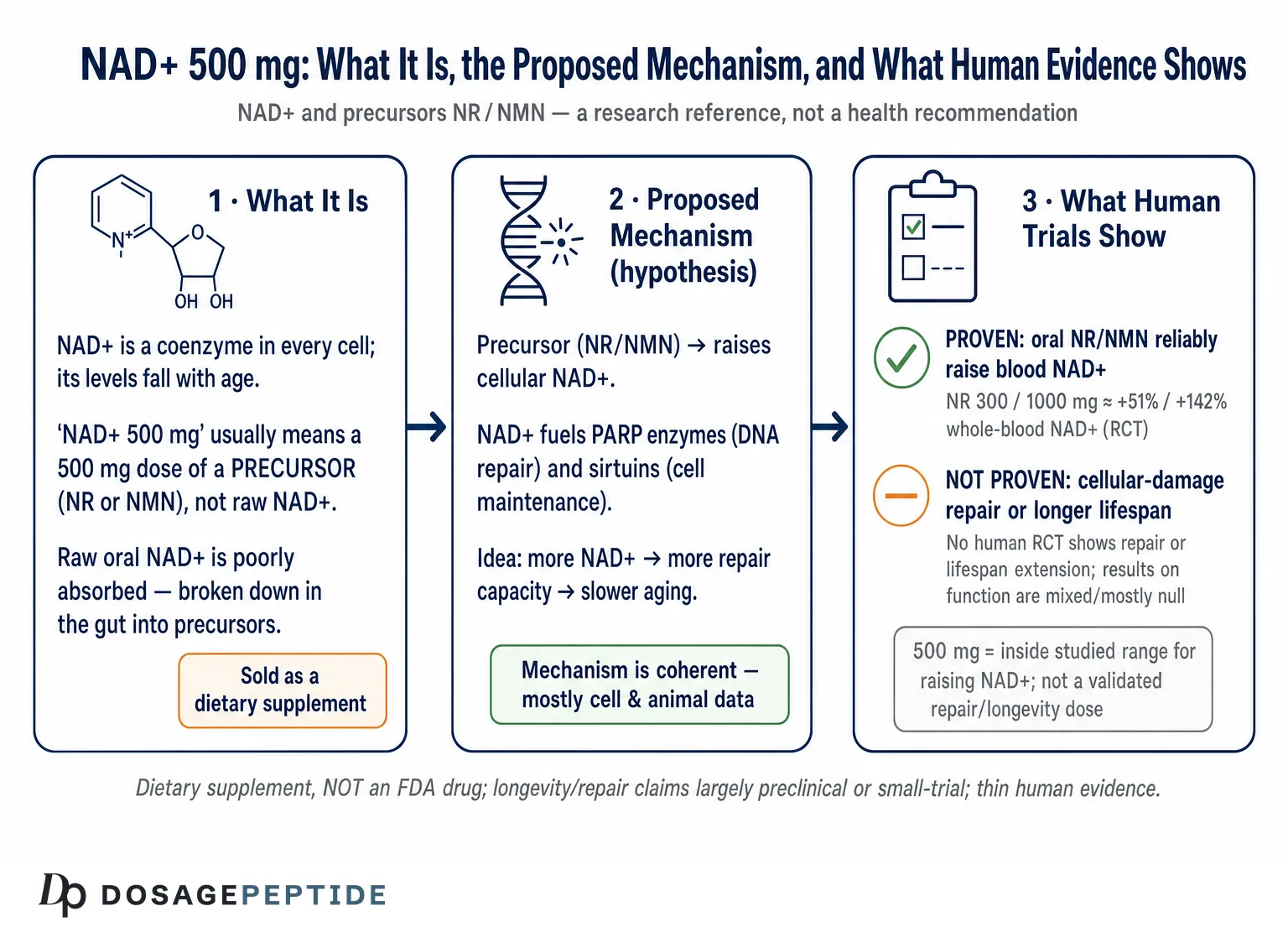
The first is NAD+ itself — the intact dinucleotide. Taken orally as a raw powder or capsule, NAD+ is a large, charged molecule that is poorly absorbed intact; the prevailing understanding is that ingested NAD+ is largely broken down in the gut into smaller building blocks (nicotinamide, nicotinamide riboside, and related metabolites) before or during absorption, and it is those fragments, not the parent molecule, that the body reassembles into new NAD+ inside cells.1 This is why serious human pharmacology has largely bypassed oral NAD+ in favour of its precursors.
The second is a precursor such as NR or NMN, dosed in the hundreds of milligrams — and here 500 mg is a genuinely representative figure, sitting between the commonly studied 250–300 mg and 1000 mg doses. When popular sources say “NAD+ 500 mg,” they very often mean a 500 mg dose of a precursor marketed under the NAD+ banner.
The third is intravenous NAD+, delivered by infusion in doses that can reach the hundreds of milligrams to grams over several hours in clinics that market “NAD+ therapy.” This bypasses the gut entirely but is expensive, time-consuming, frequently uncomfortable (rapid infusion causes chest tightness, nausea, and flushing), and supported by strikingly little controlled evidence for the anti-ageing claims attached to it.
The practical consequence is that “500 mg” is not a single, well-characterized intervention with a known effect. It is a number that could describe an orally near-useless dose of raw NAD+, a mid-range dose of a precursor with reproducible NAD+-raising pharmacology, or a fraction of an IV protocol. For the rest of this article, when we discuss the strongest human data, we are almost always discussing precursors — because that is where the randomized controlled trials live. Readers wanting to see how these compounds are catalogued and how reconstitution and dosing math are handled in a research context can consult the site’s central dosage index and reconstitution guide, both of which frame these materials as research references rather than health recommendations.
What NAD+ Is and Why It Falls With Age
NAD+ is a coenzyme present in every living cell. Its most familiar role is in energy metabolism: as the oxidized member of the NAD+/NADH redox couple, it shuttles electrons through glycolysis, the citric-acid cycle, and oxidative phosphorylation, making it indispensable to the conversion of food into ATP. If NAD+ did nothing else, it would still be essential to life. But over the past two decades a second identity has come into focus that is far more relevant to the “repair and longevity” question: NAD+ is also a consumed substrate for a family of signalling enzymes that spend it, cleaving the molecule as part of their catalytic cycle.1
Three enzyme families dominate this consumptive use. The sirtuins (SIRT1–7) are NAD+-dependent deacylases that regulate gene expression, mitochondrial biogenesis, inflammation, and stress resistance — they are the proteins most often invoked in longevity biology. The poly(ADP-ribose) polymerases (PARPs, especially PARP1) detect DNA breaks and consume large amounts of NAD+ to build the poly(ADP-ribose) chains that recruit repair machinery. And the NADases, chiefly CD38 (with the related CD157 and SARM1), hydrolyse NAD+ as part of immune and metabolic signalling.1 Because all three families consume NAD+ rather than merely borrowing it, the cell must continuously resynthesize the molecule through salvage pathways to keep the pool full.
This is the crux of the ageing story. Across model organisms and in humans, tissue and cellular NAD+ levels decline gradually with age.1 The decline appears to be driven less by a failure to make NAD+ and more by accelerated destruction and rising demand: chronic low-grade inflammation and cellular senescence raise CD38 expression, and CD38 has been shown to be a principal driver of age-related NAD+ decline and mitochondrial dysfunction, acting in part through effects on the sirtuin SIRT3.2 At the same time, accumulating DNA damage keeps PARP1 chronically activated, and an active PARP1 can consume NAD+ voraciously, drawing down the same pool the sirtuins need.1 The result is a vicious circle: less NAD+ means weaker sirtuin and repair function, which permits more damage and inflammation, which raises consumption and lowers NAD+ further.
It is this circle that makes NAD+ repletion such an attractive idea. If declining NAD+ is upstream of multiple hallmarks of ageing — genomic instability, mitochondrial dysfunction, chronic inflammation, cellular senescence — then restoring it might, in principle, blunt several of those hallmarks at once. That is a genuinely compelling hypothesis, and it is why so many capable laboratories work on it. But “compelling hypothesis” is a description of promise, not of proof, and the distance between the two is the subject of this article. For readers exploring the downstream biology, the site’s coverage of how NAD+ links to DNA repair traces these pathways in more detail.
The Bioavailability Problem: Why Researchers Rarely Give NAD+ Itself
A recurring source of confusion is the assumption that to raise NAD+ you should simply take NAD+. The biology makes this far less straightforward than it sounds, and understanding why clarifies the entire evidence base.
NAD+ is a dinucleotide — two nucleotides joined through their phosphate groups — carrying multiple charges at physiological pH. Large, polar, charged molecules do not cross the intestinal wall or the plasma membrane efficiently. The dominant view from tracer and metabolic studies is that orally administered NAD+ is substantially degraded before it reaches the systemic circulation intact, broken down into nicotinamide and nicotinamide-riboside-type fragments in the gut, which are then absorbed and used by tissues to synthesize NAD+ through the salvage pathway.1 In other words, even when you take NAD+ orally, much of whatever benefit accrues is likely delivered by its breakdown products behaving as precursors.
This is precisely why the human clinical literature is built around precursors rather than the parent molecule. Nicotinamide riboside (NR) and nicotinamide mononucleotide (NMN) are smaller, are handled by dedicated transport and salvage machinery, and have been shown repeatedly and reproducibly to raise blood NAD+ in humans.45 When a study wants to test whether “boosting NAD+” does anything, it almost always administers NR or NMN, measures the rise in NAD+ to confirm the intervention worked biochemically, and then looks for downstream effects. The intact-NAD+ oral route is scientifically the weakest of the options and, tellingly, the one with the least rigorous outcome data.
Intravenous NAD+ occupies a different niche. Infusion delivers the intact molecule into the bloodstream, sidestepping the gut. But even here the pharmacology is not simple: infused NAD+ is rapidly metabolized, plasma dynamics are complex, and controlled trials measuring meaningful clinical outcomes from IV NAD+ — as opposed to anecdote and open-label observation — are scarce. The high cost, the infusion-related discomfort, and the thin evidence base together explain why IV NAD+, despite its popularity in wellness marketing, sits well outside mainstream evidence-based practice.
The takeaway for anyone parsing a “500 mg NAD+” claim is this: the route and the molecular form matter enormously, and the form with the best human pharmacology (an oral precursor) is not the same thing as the raw NAD+ implied by the name. Conflating them — treating a precursor’s reproducible NAD+-raising data as if it validated raw oral NAD+ powder, or vice versa — is one of the most common errors in this space.
Mechanisms of Cellular Damage Repair: The Theory Behind the Claim
To evaluate whether NAD+ repletion could plausibly repair cellular damage, it helps to lay out the mechanistic chain in full — and then to note, at each link, where the human evidence is strong and where it is absent.
DNA repair via PARPs. When DNA sustains breaks — from oxidative stress, radiation, or replication errors — PARP1 is among the first responders, and it uses NAD+ as its substrate to synthesize poly(ADP-ribose), a signal that recruits and coordinates repair proteins.1 The logic is intuitive: if NAD+ is the fuel PARP1 burns to repair DNA, then more NAD+ should support more or better repair. There is solid preclinical support for NAD+ availability influencing DNA-repair capacity, and this is the most direct mechanistic basis for the “cellular damage repair” framing. The caution is that PARP1 is a double-edged actor: excessive PARP1 activation can itself deplete NAD+ to lethal levels, so the relationship between NAD+, PARP activity, and repair is not a simple “more is better” dial. In humans, no trial has yet shown that supplementing a precursor measurably improves DNA-repair outcomes or reduces mutation burden in a way that translates to health benefit.
Sirtuins and stress resistance. The sirtuins depend on NAD+ to deacylate their targets, and through those targets they influence mitochondrial biogenesis (via PGC-1α), antioxidant defences, inflammatory signalling, and the activity of repair and longevity-associated transcription factors.3 Because sirtuin activity is limited by NAD+ availability, raising NAD+ is hypothesized to enhance sirtuin-mediated maintenance — the molecular basis for most longevity claims. Again, the preclinical support is substantial and the human confirmation is thin: showing that NAD+ rose in blood is not the same as showing that sirtuin-dependent programs meaningfully shifted in human tissue, let alone that lifespan changed.
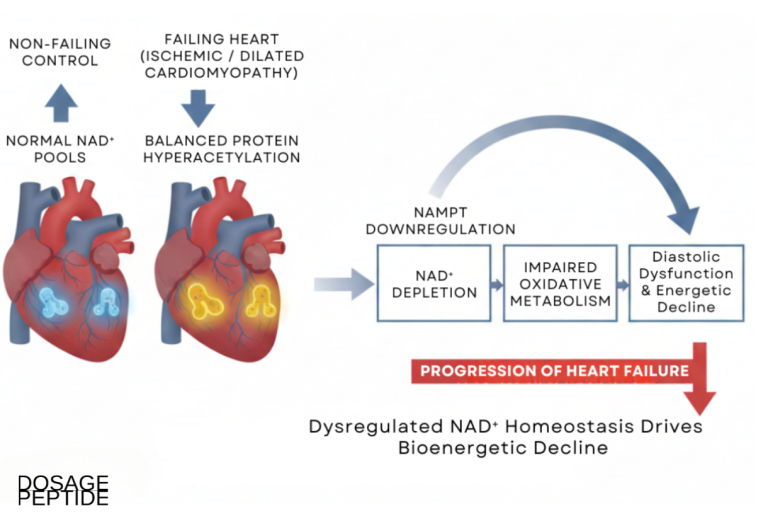
Mitochondrial function. As the redox workhorse, NAD+ is essential to mitochondrial energy production, and age-related NAD+ decline is linked to mitochondrial dysfunction.2 Restoring NAD+ improves mitochondrial measures in numerous rodent studies. Yet one of the more sobering human findings comes from a rigorous skeletal-muscle study in which three weeks of high-dose NR clearly raised the muscle NAD+ metabolome but did not increase mitochondrial bioenergetic capacity; instead it produced transcriptomic and anti-inflammatory signatures and even down-regulated some energy-metabolism pathways.6 That dissociation — NAD+ up, but the expected bioenergetic payoff absent — is a recurring theme and a warning against assuming the rodent mechanism transfers cleanly to people.
Neuroprotection and beyond. NAD+ metabolism is also implicated in axonal integrity (through the SARM1 pathway) and in neuronal resilience, which is why NAD+ precursors are studied in neurodegeneration and stroke models. The site’s discussions of NAD+ deficiency and Parkinson’s progression and of NAD+ and neuronal preservation during stroke survey those preclinical and early-clinical threads. The honest summary across all these mechanisms is the same: the biology is coherent and the animal data are frequently impressive, but each mechanistic link that looks robust in a mouse becomes a question mark when you ask for the human randomized-trial evidence.
What Human Trials Actually Show, Part 1: NAD+ Elevation Is Real
If there is one thing the human literature has established beyond reasonable doubt, it is that oral NAD+ precursors raise blood NAD+ in a dose-dependent, reproducible way. This is the strongest, cleanest result in the entire field, and it deserves to be stated plainly before we turn to the weaker claims.
In a well-conducted 8-week randomized, double-blind, placebo-controlled trial in overweight but otherwise healthy adults, nicotinamide riboside chloride at 100, 300, and 1000 mg per day raised whole-blood NAD+ by roughly 22%, 51%, and 142% respectively within two weeks, with the increases sustained across the study — a textbook dose-response relationship.4 An independent randomized crossover trial in healthy middle-aged and older adults found that 1000 mg per day of NR was well tolerated and raised NAD+ by about 60%.5 In aged skeletal muscle, 1 g per day of NR for 21 days measurably augmented the muscle NAD+ metabolome.6 On the NMN side, a randomized multicentre trial testing 300, 600, and 900 mg per day for 60 days found statistically significant increases in blood NAD+ across all NMN groups, with the largest elevations at the 600 and 900 mg doses.7 A combination product pairing NR with pterostilbene likewise raised NAD+ dose-dependently — roughly 40% at a standard dose and 90% at a double dose — in a placebo-controlled study of older adults.10
The consistency here is genuinely reassuring on one narrow point: these compounds do what they say on the biochemical tin. If your only question is “will an oral NR or NMN dose raise my measurable NAD+?” the answer, across multiple independent trials, is yes. The following table summarizes the core NAD+-elevation findings.
| Trial (precursor) | Population & design | Dose | NAD+ change |
|---|---|---|---|
| Conze 2019 (NR)4 | Overweight healthy adults; RCT, 8 wk | 100 / 300 / 1000 mg/d | +22% / +51% / +142% (whole blood) |
| Martens 2018 (NR)5 | Healthy middle-aged/older; RCT crossover | 1000 mg/d | ~+60% |
| Elhassan 2019 (NR)6 | Aged men; RCT crossover, 21 d | 1000 mg/d | Muscle NAD+ metabolome elevated |
| Yi 2023 (NMN)7 | Healthy middle-aged; RCT, 60 d | 300 / 600 / 900 mg/d | Significant rise, all doses |
| Dellinger 2017 (NRPT)10 | Older adults; RCT, 8 wk | Standard / double | ~+40% / ~+90% |
Two honest caveats attach even to this strong result. First, blood NAD+ is a proxy; it is not obvious that a percentage rise in whole-blood or peripheral-blood-mononuclear-cell NAD+ mirrors the change in the tissues that matter most for ageing (brain, heart, liver, muscle), and tissue responses can differ. Second, and more importantly, raising a biomarker is not the same as improving health. The entire weight of the “repair and longevity” claim rests not on whether NAD+ goes up — it does — but on whether that rise produces meaningful functional or clinical benefit. That is where the evidence thins dramatically.
What Human Trials Actually Show, Part 2: Function and “Longevity” Endpoints
Here the picture becomes far more sobering, and intellectual honesty requires stating it directly: despite reproducible NAD+ elevation, human trials have not established that NAD+ precursors repair cellular damage in a clinically meaningful way, improve physical function robustly, slow ageing, or extend lifespan. The results on hard and soft outcomes are best described as mixed, mostly null, or preliminary.3
Consider the outcome data area by area. On cardiovascular measures, the Martens crossover trial reported that NR was well tolerated and, in a small exploratory subgroup with elevated blood pressure, was associated with a reduction in systolic blood pressure and a suggestion of reduced aortic stiffness — but these were secondary, hypothesis-generating findings in a modest sample, not confirmed endpoints.5 On skeletal muscle and mitochondria, the Elhassan study’s central lesson was a dissociation: NAD+ rose, inflammatory signatures improved, but mitochondrial bioenergetic capacity did not increase.6 On metabolic health, results are genuinely split. A carefully done randomized trial in postmenopausal women with prediabetes found that 250 mg per day of NMN improved insulin-stimulated glucose disposal and muscle insulin signalling — a real, positive functional signal.9 Yet several other NR trials in overweight or obese people found little or no improvement in insulin sensitivity, body composition, or broad metabolic markers, and systematic reviews of NMN on glucose and lipid metabolism describe modest and inconsistent effects.
On physical performance in ageing, the NMN dose-response trial reported greater six-minute-walk distance in treated groups versus placebo,7 and a 12-week study of 250 mg NMN in older Japanese adults found improvements in some lower-limb function and drowsiness measures, though with small samples and effect-size-based rather than definitive endpoints.8 But a systematic review pooling randomized trials of NMN concluded that improvements in physical-performance parameters such as grip strength were, overall, non-significant — a useful corrective to individual trials that looked encouraging in isolation.12 On cognition and post-viral recovery, a recent randomized placebo-controlled trial of high-dose NR (up to 2000 mg/d) in people with long-COVID raised NAD+ roughly 2.6- to 3.1-fold but did not significantly outperform placebo on its primary cognitive endpoint; only exploratory within-group analyses hinted at fatigue and cognitive benefit, and the authors explicitly framed those signals as preliminary and hypothesis-generating rather than practice-changing.11
Perhaps the most important single source for a realistic view is the body of critical appraisal that has emerged as the field matured. Independent reviews now emphasize that oral NR supplementation has displayed few clinically relevant effects in humans, that there is a tendency in the literature to exaggerate the importance and robustness of reported findings, and that the putative clinical potential of these compounds in people remains to be established.3 A rigorously controlled twin study of NR, for instance, improved certain muscle and microbiome measures but did not improve adiposity or overall metabolic health.13 The pattern across the literature is unmistakable: robust biomarker change, unreliable outcome change.
Crucially, on the specific claims embedded in this article’s title — measurable repair of cellular damage and extension of longevity — there is no human randomized controlled trial demonstrating either. No trial has shown that an NAD+-boosting regimen extends human lifespan; the follow-up periods are far too short and the endpoints are surrogates. No trial has shown a clinically meaningful reduction in cellular-damage burden that translates to disease prevention. The longevity claim, in humans, is at present entirely extrapolated from mechanism and from animal studies — and animal lifespan results themselves have been inconsistent.
Dose in Research Context: The “500 mg” Question
With that evidence base in view, we can address the title’s specific figure directly. Where does 500 mg sit, and does it correspond to anything meaningful?
For oral precursors, the doses studied in humans span roughly 100 to 2000 mg per day, with the most common being 250–300 mg, 500 mg, and 1000 mg.457 A 500 mg dose is therefore squarely within the studied range and, based on the dose-response data, would be expected to raise blood NAD+ appreciably — somewhere between the ~51% seen at 300 mg NR and the ~142% seen at 1000 mg NR in the Conze trial, though the exact figure depends on the precursor, the individual, and the tissue measured.4 In that narrow biochemical sense, “500 mg” is a reasonable, evidence-adjacent number. What it is not is a validated therapeutic dose for repair or longevity, because no such validated therapeutic dose exists for those outcomes at any level.
Several honest qualifications follow. First, the optimal dose for raising NAD+ is not necessarily the optimal dose for any downstream benefit — and since the downstream benefits are largely unproven, “optimal” is undefined for them. Some trials have found that higher NAD+ elevation did not translate into greater functional effect, so pushing the dose up is not obviously advantageous. Second, the form matters: 500 mg of NR, 500 mg of NMN, and 500 mg of raw NAD+ powder are not interchangeable, because they differ in absorption, transport, and conversion efficiency, with raw NAD+ the least favourable orally.1 Third, individual variability is large; baseline NAD+ status, age, body composition, and inflammatory state all influence the response. The following table places 500 mg in the context of the human dose range and its documented effects.
| Daily dose (oral precursor) | What human data suggest | Evidence status |
|---|---|---|
| 100–250 mg | Modest but real NAD+ rise; some NMN function signals at 250 mg49 | Biomarker robust; outcomes preliminary |
| 300 mg | ~50% blood NAD+ rise (NR); significant NAD+ rise (NMN)47 | Biomarker robust; outcomes mixed |
| 500 mg | Within studied range; expected substantial NAD+ rise (interpolated)4 | Biomarker plausible; no validated outcome benefit |
| 600–900 mg | Largest NMN NAD+ elevations; 6-min-walk signal7 | Biomarker robust; function uncertain |
| 1000–2000 mg | ~60–142% NAD+ rise (NR); well tolerated4511 | Biomarker robust; outcomes largely null |
The candid conclusion is that 500 mg is a defensible number for the goal of raising measurable NAD+, and an unvalidated number for the goals stated in the title. Anyone presenting “500 mg” as an established dose for cellular repair or life extension is asserting something the human evidence does not support. Researchers modelling reconstitution and dosing arithmetic for study purposes can reference the site’s dosage calculator, keeping in mind that these tools describe how to prepare a solution, not evidence that any dose achieves the outcomes marketed for it.
NAD+ Versus Its Precursors: A Practical Comparison
Because the terms are used loosely and interchangeably, it is worth setting NAD+ and its main precursors side by side, so that a “NAD+ 500 mg” product can be interpreted correctly depending on what it actually contains.
| Form | Oral bioavailability | Human NAD+-raising evidence | Best-studied outcome context |
|---|---|---|---|
| NAD+ (raw, oral) | Poor; largely degraded to precursors in gut1 | Weak/indirect (acts via breakdown products) | Little rigorous outcome data |
| NAD+ (intravenous) | Bypasses gut; rapidly metabolized | Raises NAD+ but pharmacology complex | Mostly anecdote/open-label; few RCTs |
| Nicotinamide riboside (NR) | Good; dedicated transport/salvage4 | Strong, dose-dependent456 | Cardio-metabolic, muscle, long-COVID (mixed) |
| Nicotinamide mononucleotide (NMN) | Good; salvage substrate7 | Strong, dose-dependent7 | Insulin sensitivity, physical function (mixed) |
| Niacin / nicotinamide (vitamin B3) | Excellent; classic precursors | Raise NAD+; niacin causes flushing | Dyslipidemia (niacin); pellagra prevention |
Two points from this comparison deserve emphasis. First, the compounds with the best oral pharmacology and the richest trial data are the precursors NR and NMN — not raw oral NAD+ and not, in evidentiary terms, IV NAD+. Second, even the well-studied precursors converge on the same verdict: reliable NAD+ elevation, inconsistent downstream benefit.3 The differences among the forms are real and matter for absorption, but they do not rescue the longevity claim, because that claim fails at the outcome stage regardless of which form delivers the NAD+.
It is also worth noting that the humble, inexpensive B3 vitamins (niacin and nicotinamide) are themselves NAD+ precursors that have been used medically for decades. Their existence is a useful sanity check: if simply raising NAD+ with a cheap vitamin reversed ageing, we would likely have noticed over the many decades of niacin use. That we did not is consistent with the modern trial data showing that raising NAD+ is necessary-but-not-sufficient for the grand claims attached to it.
Research Models and Why Rodents Oversell the Story
Much of the excitement around NAD+ and longevity traces to animal work, and understanding the gap between those models and humans is essential to reading the field honestly.
In rodents, NAD+ decline with age is well documented, and repletion with NR or NMN has produced a striking catalogue of benefits across studies: improved insulin sensitivity, enhanced mitochondrial function, better exercise capacity, neuroprotection in models of neurodegeneration, improved vascular function, and, in some experiments, extended healthspan.3 The CD38 work in mice was particularly influential, showing that the enzyme drives age-related NAD+ decline and that inhibiting it can restore tissue NAD+ and reverse aspects of metabolic dysfunction.2 This body of preclinical evidence is genuinely substantial and is why the hypothesis is taken seriously.
But several features of the rodent literature caution against straightforward extrapolation. Mice are short-lived, inbred, and studied under controlled conditions that magnify effect sizes; interventions frequently work better in mice than in humans across many fields, not just this one. Rodent lifespan results for NAD+ precursors have themselves been inconsistent — not every study extends life, and effects often depend on strain, sex, age at initiation, and disease model. And the mechanistic endpoints measured in mice (tissue NAD+, mitochondrial markers, gene-expression signatures) are exactly the surrogates that, in the human muscle study, rose without delivering the expected bioenergetic payoff.6 The methodological lesson is that impressive mouse data establish plausibility and justify human trials; they do not establish human efficacy, and treating them as if they do is the central error behind the longevity hype.
Human studies, by contrast, are constrained in exactly the ways that make the strong claims hard to test. Lifespan endpoints are practically impossible to run — you would need decades and enormous samples — so trials rely on short-term surrogates. Sample sizes are typically small (often a few dozen participants), follow-up is measured in weeks to months, and outcome measures vary between studies, making meta-analysis difficult. The result is a literature that is strong on the narrow biochemical question and weak, by necessity and by result, on the questions people actually care about.
Safety and Tolerability
On safety, the NAD+ precursor literature is relatively reassuring for short-to-medium-term use in the populations studied — a point that must be stated with the same care applied throughout this article, because “well tolerated for a few months in a trial” is not the same as “proven safe for years of daily use across all populations.”
Across the randomized trials, oral NR and NMN have generally been well tolerated, with adverse-event rates not significantly different from placebo and no serious safety signals attributable to the compounds at the doses tested.457 Notably, unlike high-dose niacin, NR and NMN do not typically cause the flushing reaction, which improves tolerability.4 Long-term safety studies out to a year in overweight adults did not surface major concerns at the studied doses.4 The following considerations temper this generally favourable picture:
- Duration. Most trials ran weeks to months; a small number extended to a year. Lifelong or multi-year daily supplementation — the way many people actually use these products for “longevity” — has not been characterized for safety.
- Population. Participants were largely healthy or metabolically at-risk adults. Safety in people with cancer, serious illness, pregnancy, or on complex medication regimens is not established, and there is theoretical debate about whether boosting NAD+ could, in some contexts, support the metabolism of existing malignant cells — an unresolved question that argues for caution rather than alarm.
- IV NAD+ specifically. Rapid intravenous infusion commonly causes uncomfortable acute reactions (chest pressure, nausea, cramping, flushing) that are infusion-rate dependent, and the longer-term safety of repeated infusions is not well studied.
- Product quality. Because these are sold as supplements, purity and actual content vary between brands; independent testing has repeatedly found products whose NMN or NR content differs from the label. Impurities and mislabelling are real-world risks independent of the molecule’s intrinsic safety.
The reasonable reading is that NR and NMN appear to have a benign short-term safety profile in the studied populations and doses, that they avoid the flushing problem of niacin, and that this favourable tolerability is, ironically, part of why they are easy to over-promote — a well-tolerated compound invites open-ended use even in the absence of demonstrated benefit. Absence of demonstrated harm and absence of demonstrated efficacy can coexist, and here, for the longevity and repair claims, they do.
Regulatory Status
The regulatory picture for NAD+ and its precursors is genuinely tangled and has shifted recently, so precision matters.
Not FDA-approved drugs for repair or longevity. Neither NAD+ itself nor NR nor NMN is approved by the U.S. Food and Drug Administration, the European Medicines Agency, or any comparable regulator as a drug to repair cellular damage, slow ageing, or extend lifespan. There is no approved indication of that kind for any NAD+-boosting product. These are marketed and regulated as dietary supplements (or, for IV NAD+, often as clinic-administered wellness services), not as medicines with proven efficacy for the claims attached to them.
Dietary-supplement status — and the NMN saga. Nicotinamide riboside has been marketed as a dietary supplement in the United States for years and has received self-affirmed “generally recognized as safe” (GRAS) treatment as an ingredient — a food-safety concept that speaks to ingredient safety at defined exposure, not to therapeutic efficacy or drug approval. NMN’s path has been far bumpier. In November 2022 the FDA took the position that NMN could not be marketed as a dietary supplement because it had earlier been authorized for investigation as a new drug, invoking the “drug preclusion” provision of U.S. supplement law.14 That determination was controversial, was contested by industry, and was subsequently revisited: by 2025 the agency had reversed course and indicated that NMN could lawfully be used in dietary supplements after all.14 The whiplash is itself instructive — it reflects a substance caught between supplement and drug frameworks, not one whose therapeutic value regulators have endorsed.
What GRAS and supplement status do and do not mean. A recurring public misunderstanding deserves explicit correction: the fact that NR or NMN is sold legally as a supplement, or that an ingredient carries a GRAS designation, says nothing about whether it repairs cells or extends life. GRAS is a safety-and-food-law concept; supplement marketing in the United States does not require proof of efficacy before sale, only that claims avoid asserting the treatment of disease. So a legal, GRAS-affirmed, widely sold NAD+ precursor can be simultaneously safe to consume and unproven for the very benefits its marketing evokes. Conflating “legal to sell as a supplement” with “shown to work” is one of the most common errors in this space, and it is worth carrying that distinction into every product claim you encounter.
The regulatory synthesis is straightforward: NAD+ and its precursors occupy the dietary-supplement and wellness-service space, not the approved-drug space, for any repair or longevity use. There is no regulatory recognition anywhere that these products achieve the outcomes in this article’s title. For readers tracking how the evidence and rules evolve, the site’s peptide and compound glossary defines the surrounding terminology, and its treatment of the NAD+–DNA-repair link traces the underlying mechanisms.
Limitations and the Longevity-Hype Gap
Pulling the threads together, the limitations bearing on the title’s question are severe and, importantly, they compound one another.
Surrogate, not outcome. The strongest human finding — reproducible NAD+ elevation — is a biomarker, and blood NAD+ may not reflect the tissues that matter, nor does its rise reliably predict functional benefit.6 The whole edifice of “repair and longevity” rests on outcomes that trials have mostly failed to move.
No lifespan data in humans. There is not, and realistically cannot soon be, a randomized trial showing that an NAD+ regimen extends human lifespan. Every longevity claim is extrapolated from mechanism and from inconsistent animal data.3
Mixed and often null functional results. Across cardiovascular, metabolic, muscular, cognitive, and physical-performance endpoints, human trials are a patchwork of small positive signals, non-significant trends, and outright nulls, with independent reviews warning of a tendency to overstate the robustness of the positives.31213
Form and route confusion. “NAD+ 500 mg” may denote a near-useless oral raw dose, a well-absorbed precursor, or a fraction of an IV protocol — and these are not equivalent.1 Much popular writing blurs them, importing the precursor pharmacology data onto raw NAD+ or the reverse.
Small, short, heterogeneous trials. Sample sizes of dozens, follow-up of weeks to months, and inconsistent endpoints make firm conclusions impossible and meta-analysis fragile.
Commercial pressure. This is a large and lucrative market, and the incentive to translate “raises a biomarker” into “repairs your cells and extends your life” is enormous. The critical-appraisal literature exists precisely because that translation has repeatedly outrun the data.3
The longevity-hype gap, then, is not a minor caveat to be waved away with mechanism talk. It is the central fact. NAD+ biology is real, its age-related decline is real, and the hypothesis that repletion could help is legitimate and worth researching. But the claim implied by this article’s title — that a 500 mg dose of NAD+ repairs cellular damage and extends longevity, as shown in human studies — is not supported. Human studies show that precursors raise NAD+ reliably and that this rise has, so far, produced disappointingly little proven benefit. Responsible communication means holding both halves of that sentence at once.
Frequently Asked Questions
Does taking 500 mg of NAD+ repair cellular damage in humans?
There is no human randomized controlled trial demonstrating that any NAD+ dose, including 500 mg, measurably repairs cellular damage in a way that translates to health benefit. The mechanistic rationale — NAD+ fuels PARP-mediated DNA repair and sirtuin-mediated maintenance — is real and well studied in cells and animals, but in humans the proven effect of NAD+ precursors is that they raise blood NAD+ levels, not that they demonstrably repair cells or reverse damage.13 The repair claim remains a plausible hypothesis, not a demonstrated human outcome.
Will NAD+ or its precursors extend my lifespan?
No human study has shown that NAD+, NR, or NMN extends lifespan, and such a trial is practically very difficult to run because it would require decades and huge samples. Longevity claims are extrapolated from mechanism and from animal studies, and even the animal lifespan data are inconsistent.3 Anyone stating that these compounds are proven to extend human life is overstating the evidence.
Is it better to take NAD+ directly or a precursor like NR or NMN?
Oral NAD+ is a large, charged molecule that is poorly absorbed intact and is largely broken down into precursors in the gut, so much of any effect is delivered by those breakdown products anyway.1 This is why the strongest human data are on the precursors NR and NMN, which are well absorbed and reproducibly raise blood NAD+.47 If the goal is simply to raise measurable NAD+, an oral precursor has far better evidence than raw oral NAD+ powder.
Do NR and NMN actually raise NAD+ levels in people?
Yes — this is the best-established finding in the field. Multiple randomized controlled trials show dose-dependent increases in blood NAD+: for example, NR at 100/300/1000 mg raised whole-blood NAD+ by roughly 22%/51%/142%, and NMN at 300–900 mg significantly raised NAD+ across all doses.47 The reliability of this biomarker effect is not in dispute; what is disputed is whether the rise produces meaningful health benefits.
Why do some human trials show benefits and others show nothing?
Because the outcome literature is genuinely mixed. A few trials report positive signals — improved insulin sensitivity with NMN in prediabetic women, a blood-pressure signal with NR, some physical-function measures — while many others find little or no effect, and a landmark muscle study found NAD+ rose without improving mitochondrial bioenergetics.69 Small samples, short durations, different populations, and different endpoints all contribute, and independent reviews caution that positive findings are often overstated.3
Is NAD+ supplementation safe?
In the randomized trials conducted so far, oral NR and NMN have generally been well tolerated over weeks to months, with adverse events similar to placebo and no flushing of the kind high-dose niacin causes.45 However, long-term (multi-year) safety is not established, safety in serious illness or pregnancy is not characterized, IV NAD+ can cause uncomfortable infusion reactions, and supplement product quality varies. A benign short-term profile is not the same as proven long-term safety, and it is not evidence of benefit.
What does “NAD+ IV therapy” do, and is it proven?
Intravenous NAD+ delivers the intact molecule into the bloodstream, bypassing the gut, and it does raise NAD+ — but the pharmacology is complex, infusions are costly and often uncomfortable, and controlled trials measuring meaningful clinical outcomes are scarce. Most support for IV NAD+ anti-ageing claims is anecdotal or open-label, not from rigorous randomized trials, so it sits outside evidence-based practice for the benefits typically marketed.
Is NAD+ or NMN approved by the FDA?
Not as a drug for repair or longevity. NR and NMN are handled as dietary-supplement ingredients (NR with self-affirmed GRAS status), and NMN’s supplement status was contested by the FDA in 2022 under the drug-preclusion rule before being reversed by 2025.14 Legal supplement status and GRAS designations speak to safety and marketing, not to proven efficacy for cellular repair or life extension.
If the evidence is thin, why is NAD+ so popular?
Because the underlying biology is genuinely compelling, the age-related decline is real, the animal data are impressive, the compounds are well tolerated, and the market is large and heavily promoted. All of that creates strong momentum to translate “raises a biomarker” into “repairs cells and extends life” — a translation the human data do not yet justify.3 Popularity reflects plausibility and marketing more than proof.
References
- Covarrubias AJ, Perrone R, Grozio A, Verdin E. NAD+ metabolism and its roles in cellular processes during ageing. Nat Rev Mol Cell Biol. 2021;22(2):119-141. PMID: 33353981. https://pubmed.ncbi.nlm.nih.gov/33353981/
- Camacho-Pereira J, Tarragó MG, Chini CCS, et al. CD38 Dictates Age-Related NAD Decline and Mitochondrial Dysfunction through an SIRT3-Dependent Mechanism. Cell Metab. 2016;23(6):1127-1139. PMID: 27304511. https://pubmed.ncbi.nlm.nih.gov/27304511/
- Rajman L, Chwalek K, Sinclair DA. Therapeutic Potential of NAD-Boosting Molecules: The In Vivo Evidence. Cell Metab. 2018;27(3):529-547. PMID: 29514064. https://pubmed.ncbi.nlm.nih.gov/29514064/
- Conze D, Brenner C, Kruger CL. Safety and Metabolism of Long-term Administration of NIAGEN (Nicotinamide Riboside Chloride) in a Randomized, Double-Blind, Placebo-controlled Clinical Trial of Healthy Overweight Adults. Sci Rep. 2019;9(1):9772. PMID: 31278280. https://pubmed.ncbi.nlm.nih.gov/31278280/
- Martens CR, Denman BA, Mazzo MR, et al. Chronic nicotinamide riboside supplementation is well-tolerated and elevates NAD+ in healthy middle-aged and older adults. Nat Commun. 2018;9(1):1286. PMID: 29599478. https://pubmed.ncbi.nlm.nih.gov/29599478/
- Elhassan YS, Kluckova K, Fletcher RS, et al. Nicotinamide Riboside Augments the Aged Human Skeletal Muscle NAD+ Metabolome and Induces Transcriptomic and Anti-inflammatory Signatures. Cell Rep. 2019;28(7):1717-1728.e6. PMID: 31412242. https://pubmed.ncbi.nlm.nih.gov/31412242/
- Yi L, Maier AB, Tao R, et al. The efficacy and safety of β-nicotinamide mononucleotide (NMN) supplementation in healthy middle-aged adults: a randomized, multicenter, double-blind, placebo-controlled, parallel-group, dose-dependent clinical trial. Geroscience. 2023;45(1):29-43. PMID: 36482258. https://pubmed.ncbi.nlm.nih.gov/36482258/
- Kim M, Seol J, Sato T, Fukamizu Y, Sakurai T, Okura T. Effect of 12-Week Intake of Nicotinamide Mononucleotide on Sleep Quality, Fatigue, and Physical Performance in Older Japanese Adults: A Randomized, Double-Blind Placebo-Controlled Study. Nutrients. 2022;14(4):755. PMID: 35215405. https://pubmed.ncbi.nlm.nih.gov/35215405/
- Yoshino M, Yoshino J, Kayser BD, et al. Nicotinamide mononucleotide increases muscle insulin sensitivity in prediabetic women. Science. 2021;372(6547):1224-1229. PMID: 33888596. https://pubmed.ncbi.nlm.nih.gov/33888596/
- Dellinger RW, Santos SR, Morris M, et al. Repeat dose NRPT (nicotinamide riboside and pterostilbene) increases NAD+ levels in humans safely and sustainably: a randomized, double-blind, placebo-controlled study. NPJ Aging Mech Dis. 2017;3:17. PMID: 29184669. https://pubmed.ncbi.nlm.nih.gov/29184669/
- Wu CY, Guzmán-Vélez E, McManus AJ, et al. Effects of nicotinamide riboside on NAD+ levels, cognition, and symptom recovery in long-COVID: a randomized controlled trial. eClinicalMedicine. 2025. PMID: 41357333. https://pubmed.ncbi.nlm.nih.gov/41357333/
- Improved Physical Performance Parameters in Patients Taking Nicotinamide Mononucleotide (NMN): A Systematic Review of Randomized Control Trials. Cureus. 2024. PMID: 39221308. https://pubmed.ncbi.nlm.nih.gov/39221308/
- Lapatto HAK, Kuusela M, Heikkinen A, et al. Nicotinamide riboside improves muscle mitochondrial biogenesis, satellite cell differentiation, and gut microbiota in a twin study. Sci Adv. 2023;9(2):eadd5163. PMID: 36638183. https://pubmed.ncbi.nlm.nih.gov/36638183/
- U.S. Food and Drug Administration; regulatory reporting on the dietary-supplement status of nicotinamide mononucleotide (NMN) — 2022 drug-preclusion determination and subsequent 2025 reversal. Venable LLP analysis, 2025. https://www.venable.com/insights/publications/2025/10/fda-declares-nicotinamide-mononucleotide-is
Educational and research-use disclaimer: This article is provided solely for scientific and educational purposes. NAD+ and its precursors nicotinamide riboside (NR) and nicotinamide mononucleotide (NMN) are marketed as dietary supplements and are not approved by the FDA, EMA, or any comparable regulator to repair cellular damage, slow ageing, extend lifespan, or treat, cure, or prevent any disease. No human randomized controlled trial has demonstrated that any NAD+ dose, including 500 mg, extends human longevity or measurably repairs cellular damage in a clinically meaningful way; the strongest human evidence shows only that oral precursors reproducibly raise blood NAD+ levels. Nothing here is medical advice or a recommendation for human use. Readers should consult qualified healthcare professionals and applicable regulations before making any decisions.