Melanotan II is a synthetic, cyclic analog of alpha-melanocyte-stimulating hormone (α-MSH) that has become one of the most talked-about — and most misunderstood — peptides in the pigmentation literature. It was engineered specifically to switch on the same receptor that the body uses to darken skin, and in a small number of early human experiments it did exactly that: it produced visible tanning without ultraviolet light. That single observation is the reason the compound keeps resurfacing in scientific discussion, in online marketplaces, and in regulatory warnings alike. Yet the distance between “a peptide activated a receptor in a pilot study” and “a safe, proven product” is enormous, and this article is written to help researchers and educated readers understand exactly where that gap lies.1
The question “how does Melanotan II influence melanin production in scientific skin studies?” has a genuinely interesting mechanistic answer rooted in the melanocortin-1 receptor (MC1R) and the cyclic-AMP signaling cascade that governs pigment synthesis. But it also has a sobering scientific footnote: the human evidence base is thin, dated, and dominated by tiny early-phase trials and a growing catalogue of adverse-event case reports. Melanotan II is not an approved drug in the United States, the European Union, Australia, or the United Kingdom. It is a research chemical, and the version sold online is unregulated, frequently mislabeled, and legally prohibited as a consumer tanning agent in multiple jurisdictions.9,11
Below, we walk through the biology of melanin, the receptor pharmacology that lets Melanotan II drive melanogenesis, the actual studies that have been done, the compounds it is often confused with, the research models scientists use, and the substantial safety and regulatory concerns that surround it. Throughout, the aim is to describe the science honestly — neither dismissing the real receptor-level pharmacology nor inflating a handful of small experiments into evidence of safety or efficacy. This is educational material for a research audience, not medical guidance.
What Melanotan II Is and Where It Came From
Melanotan II (often abbreviated MT-II or MT-2) is a synthetic heptapeptide — a chain of seven amino acids arranged in a cyclic, lactam-bridged ring. Its structure is a deliberate redesign of endogenous α-MSH, the natural 13-amino-acid melanocortin peptide that the body releases to stimulate pigment-producing cells. The abbreviated cyclic sequence is commonly written as Ac-Nle-cyclo[Asp-His-D-Phe-Arg-Trp-Lys]-NH2. Every element of that design has a purpose: the ring constrains the molecule into a shape that fits the melanocortin receptor pocket, while the substituted and D-configured residues resist the enzymes that normally chew up native α-MSH within seconds.1,2
The compound originated in the 1980s and early 1990s at the University of Arizona, in the laboratories of researchers including Mac Hadley and Victor Hruby. The original scientific motivation was not cosmetic. Investigators reasoned that if they could induce the skin to build its own protective pigment on demand, they might reduce ultraviolet-driven DNA damage and, potentially, skin-cancer risk in vulnerable populations — a chemopreventive strategy. A related preformulation study by Lan, Ugwu, and colleagues explicitly framed Melanotan II as a “potential skin cancer chemopreventive peptide” and characterized its physicochemical stability with that goal in mind.5
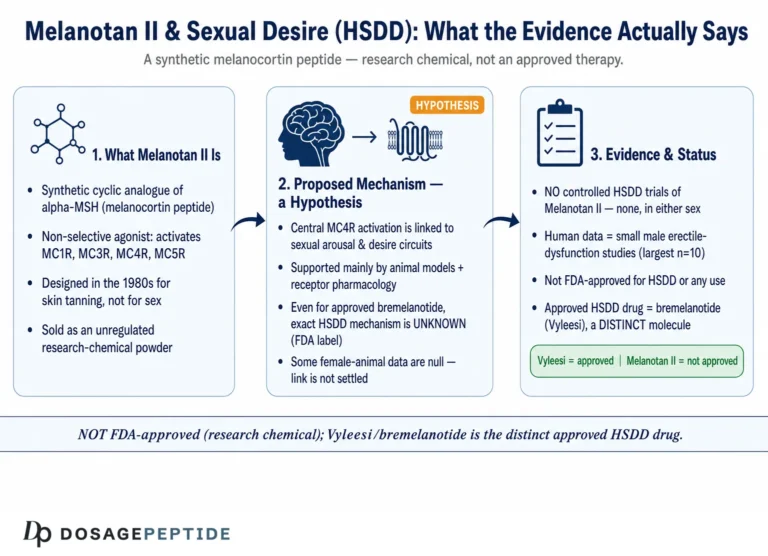
Two sibling molecules emerged from the same program and are frequently confused with MT-II. Melanotan I — the linear peptide afamelanotide — was developed as a more selective, controlled-release agent and eventually became an approved orphan drug (marketed as Scenesse) for a rare light-sensitivity disease. Melanotan II took a different path: it was found to be a “superpotent” but deliberately non-selective melanocortin agonist, meaning it activates not only the pigment receptor MC1R but also MC3R, MC4R, and MC5R. That broad receptor activity is central to both its unexpected effects (appetite suppression, spontaneous erections) and its side-effect profile.1,6
It is worth being precise about nomenclature, because the marketplace is not. “Melanotan,” “Melanotan II,” “MT-2,” and “the Barbie drug” are used loosely online, and injectable powders, nasal sprays, and troches are all sold under these names with little quality control. Analytical work by Breindahl and colleagues that examined tanning products sold illegally over the Internet found that labeled contents did not reliably match what was actually in the vial — a reminder that “Melanotan II” as a research reference standard and “Melanotan II” as a grey-market product are not the same thing.9 For dosing and reconstitution context in a research-education framework, DosagePeptide.com maintains a dedicated Melanotan II protocol reference, but the compound remains experimental throughout.
Understanding Melanin: The Pigment Behind the Effect
To understand how Melanotan II influences melanin, it helps to first understand what melanin is and how the skin normally makes it. Melanin is the family of pigments responsible for the color of skin, hair, and eyes, and it is manufactured inside specialized cells called melanocytes that sit in the basal layer of the epidermis. Within these cells, pigment is synthesized in dedicated organelles called melanosomes and then transferred to surrounding keratinocytes, where it forms protective “caps” over cell nuclei that absorb and scatter ultraviolet radiation.2,3
Crucially, melanin is not a single substance. There are two principal types, and the balance between them matters enormously. Eumelanin is the brown-black pigment that is relatively effective at absorbing UV and shielding DNA; it is the pigment associated with darker, more photoprotective tanning. Pheomelanin is the reddish-yellow pigment characteristic of fair, freckle-prone skin and red hair; it offers far less UV protection and, under UV exposure, can actually generate reactive oxygen species that contribute to oxidative DNA damage. The genetically determined ratio of these two pigments is a major reason some people tan and others burn.3
The switch that biases melanocytes toward eumelanin is MC1R. When MC1R is strongly activated — naturally by α-MSH, or pharmacologically by an agonist like Melanotan II — melanocytes shift their output toward eumelanin production. People carrying loss-of-function MC1R gene variants (common in red-haired, fair-skinned individuals) have receptors that signal poorly, produce more pheomelanin, tan weakly, and carry higher melanoma risk. This genetics of MC1R is the biological backdrop against which the entire Melanotan story plays out: the peptide is, in essence, a pharmacological attempt to force a strong “make eumelanin” signal regardless of a person’s UV exposure or their innate receptor tone.2,3
The following table summarizes the two pigment types and why the distinction is scientifically important.
| Feature | Eumelanin | Pheomelanin |
|---|---|---|
| Color | Brown to black | Red to yellow |
| UV protection | Relatively high; absorbs and scatters UV | Low; can generate reactive oxygen species under UV |
| Associated phenotype | Darker skin, dark hair, tans readily | Fair skin, red/blond hair, freckles, burns readily |
| MC1R signaling | Favored by strong MC1R activation | Predominates when MC1R signaling is weak |
| Relevance to MT-II | The pigment MC1R agonism is intended to increase | Not the target, but darkening of existing pigmented lesions is a documented concern |
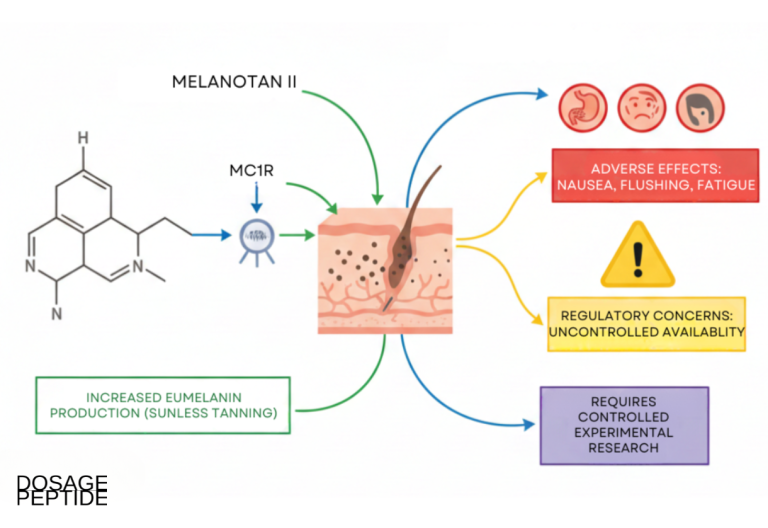
Understanding that Melanotan II is fundamentally an MC1R-directed tool clarifies both its intended action (raising eumelanin) and one of its central hazards: driving pigment machinery hard, and non-selectively, in a system where uncontrolled melanocyte stimulation raises legitimate questions about existing moles and atypical naevi.8,15
The Molecular Mechanism: How MC1R Activation Drives Melanogenesis
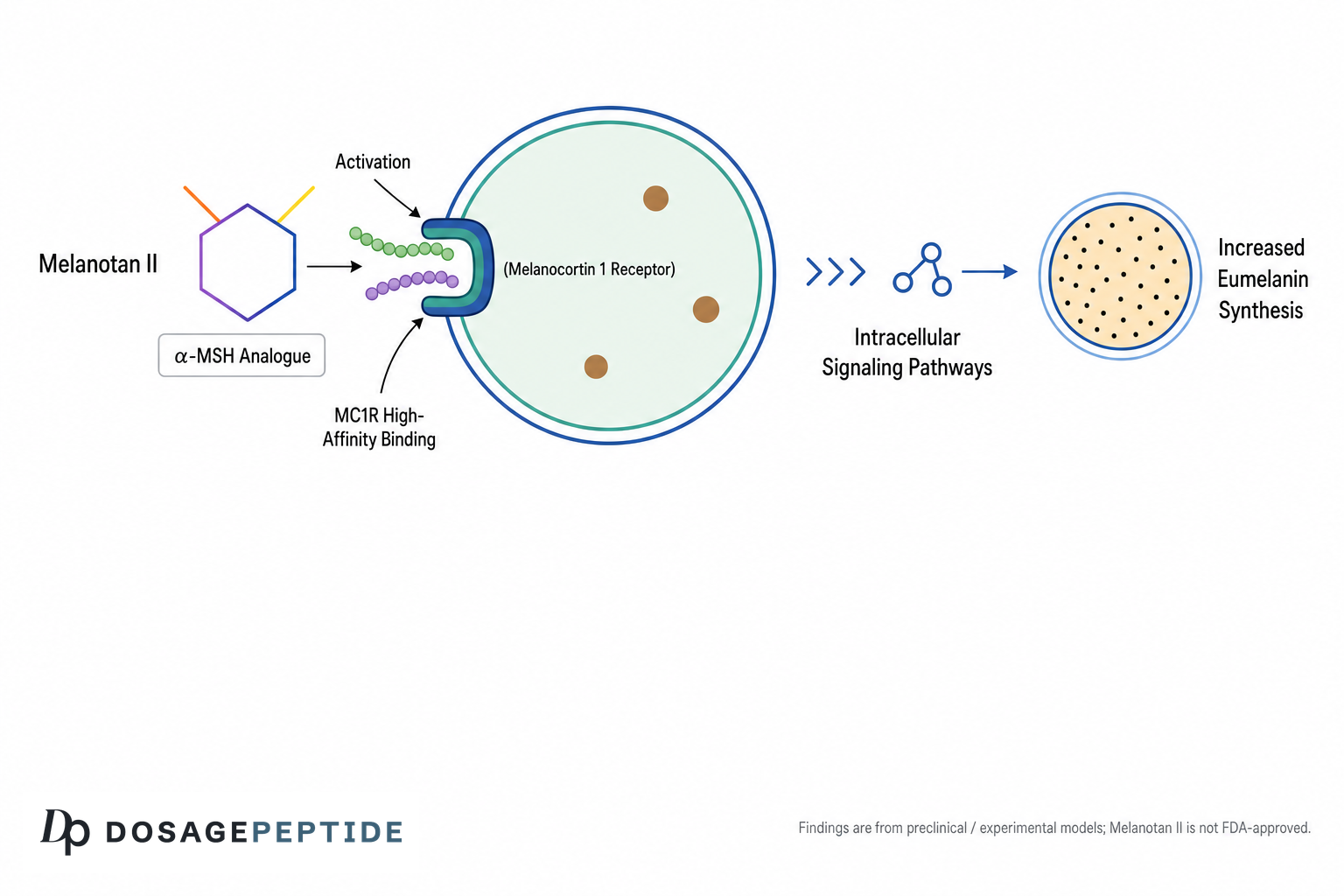
The mechanistic core of Melanotan II’s pigmentary effect is a well-characterized G-protein-coupled receptor cascade. MC1R is a Gs-coupled receptor on the melanocyte surface. When an agonist — α-MSH physiologically, or Melanotan II pharmacologically — binds MC1R, the receptor activates the stimulatory G-protein (Gsα), which in turn activates the enzyme adenylate cyclase. Adenylate cyclase converts ATP into cyclic AMP (cAMP), the second messenger that sits at the heart of pigment signaling.2,3
Rising intracellular cAMP activates protein kinase A (PKA). Active PKA catalytic subunits then phosphorylate the transcription factor CREB (cAMP-response-element-binding protein) at serine-133. Phosphorylated CREB, together with co-activators, drives transcription of the gene encoding MITF (microphthalmia-associated transcription factor), which is the master regulator of the melanocyte differentiation program. MITF, once expressed and activated, then switches on the structural and enzymatic genes that actually build pigment.3
The enzymes MITF turns on are the workhorses of melanogenesis: tyrosinase (the rate-limiting enzyme that oxidizes the amino acid tyrosine), along with tyrosinase-related protein 1 (TYRP1) and dopachrome tautomerase (DCT/TYRP2). Together these convert tyrosine through a series of intermediates into eumelanin. So the full chain, from peptide to pigment, reads: MT-II → MC1R → Gsα → adenylate cyclase → cAMP → PKA → CREB → MITF → tyrosinase/TYRP1/DCT → eumelanin. This is why an MC1R agonist can, in principle, darken skin independently of ultraviolet exposure — it injects the “tan” signal downstream of the sun.2,3
Two features make Melanotan II pharmacologically distinctive within this cascade. First, potency and duration: native α-MSH is degraded almost instantly, whereas the cyclic, enzyme-resistant structure of MT-II gives it a far longer functional half-life — in the pilot human study, plasma concentrations were consistent with a half-life on the order of tens of minutes rather than seconds, so a single dose sustains receptor activation long enough to matter biologically.1 Second, non-selectivity: because MT-II activates MC3R, MC4R, and MC5R in addition to MC1R, the same molecule that drives melanogenesis at MC1R simultaneously engages central melanocortin receptors that influence appetite, sexual arousal, and autonomic tone — which is why “a tanning peptide” also reliably produces nausea and spontaneous erections.1,6
A further layer of mechanistic nuance concerns individual variability and receptor regulation. Because MC1R is highly polymorphic, the same dose of an agonist can produce very different downstream signaling depending on a person’s receptor variants: individuals with loss-of-function MC1R alleles have receptors that couple less efficiently to Gsα and generate weaker cAMP responses, which is precisely why fair, red-haired individuals tan poorly even under strong stimulation. In principle, a supraphysiological agonist like MT-II could partially override weak endogenous signaling, but the degree to which it does so in people with different MC1R genotypes has never been systematically studied. Like most G-protein-coupled receptors, MC1R is also subject to desensitization and internalization after sustained agonist exposure, so continuous high-level stimulation does not translate linearly into ever-increasing pigment. These regulatory realities are one reason mechanistic elegance on paper does not guarantee predictable results at the level of a whole organism.2,3
It is important to note a mechanistic subtlety that is often glossed over: the tan produced by MC1R agonism is a genuine increase in epidermal eumelanin, but its magnitude and durability in humans have only been measured in very small samples. The signaling pathway is not in doubt — it is textbook cell biology — but “the pathway exists and MT-II engages it” is a claim about mechanism, not a claim about clinically meaningful, safe, or reproducible results in people. The reconstitution and handling context needed to work with such peptides in vitro is discussed further below and in the DosagePeptide peptide reconstitution guide.
Key Evidence From Scientific Skin Studies (and Its Real Level)
Here the honesty has to be front and center: the direct human pigmentation evidence for Melanotan II rests on a very small number of early studies, most of them decades old and conducted in single-digit numbers of volunteers. The anchor citation is the pilot phase-I study by Dorr and colleagues, published in Life Sciences in 1996. It was a single-blind, placebo-controlled trial in just three healthy male volunteers, who received subcutaneous MT-II or saline daily on weekdays for two weeks, starting at 0.01 mg/kg and escalating in small increments to roughly 0.025–0.03 mg/kg.1
The pigmentary result was real but modest in scope: two of the three subjects showed increased pigmentation in the face, upper body, and other sites, measured both by quantitative reflectance and by visual assessment about a week after dosing ended. That is genuinely notable — it is direct human evidence that an MC1R agonist can darken skin without UV — but three subjects is not a foundation for any claim about efficacy, dose-response, or safety at the population level. The same study documented dose-limiting side effects (nausea, flushing, spontaneous erections) at these low doses, which is itself an important part of the evidentiary picture.1
Complementary human pharmacokinetic and pigmentation data come from work on the sibling peptide Melanotan I (afamelanotide). Ugwu, Blanchard, and colleagues characterized melanotan-I in humans and reported essentially complete subcutaneous bioavailability with pigmentation persisting for weeks after dosing — useful comparative context, but data about the linear analog, not MT-II itself.4 Meanwhile, most of the additional “human MT-II” literature concerns sexual function rather than tanning: Wessells and colleagues studied MT-II for erectile response in men, reporting that it initiated erections in a majority of subjects but with frequent nausea and yawning.6,7 These are the studies that gave rise to the drug bremelanotide (PT-141), an MT-II metabolite developed separately for sexual dysfunction.
Beyond these small trials, the largest body of “evidence” is unfortunately a catalogue of adverse-event case reports and one influential review. A widely cited review of melanotan use and associated clinical outcomes gathered roughly eighteen clinical studies and more than twenty case presentations, and its overall message was cautionary: alongside tanning, the literature is dominated by reports of nausea, darkening and change of moles, new naevi, and more serious systemic toxicity.8 The table below places the evidence in an honest hierarchy.
| Evidence type | What exists for MT-II | Strength |
|---|---|---|
| In vitro / mechanistic | Well-established MC1R–cAMP–MITF–tyrosinase pathway | Strong for mechanism, not for outcomes |
| Animal models | Pigmentation and receptor pharmacology in frog/rodent systems | Supportive of mechanism |
| Human pigmentation trials | Pilot phase-I, n=3 (Dorr 1996) | Very limited; hypothesis-generating only |
| Human sexual-function trials | Small crossover studies (Wessells) | Limited; different endpoint |
| Phase 2/3 efficacy or safety trials | None completed for MT-II tanning | Absent |
| Post-market/real-world | Numerous adverse-event case reports | Signals harm, not efficacy |
It is worth dwelling on why the evidence base stalled where it did. The University of Arizona program that generated MT-II was scientifically productive, but the compound’s non-selectivity meant that dose-limiting side effects appeared at or near the doses needed for tanning — a poor therapeutic window for a cosmetic application. Rather than pushing MT-II itself through large tanning trials, developers pivoted: the more selective linear analog (afamelanotide) was carried forward for medical photoprotection, and the sexual-function branch became bremelanotide. Melanotan II, in effect, was left behind by legitimate drug development and picked up instead by the unregulated grey market. This history matters because it explains a counterintuitive fact — the peptide is widely used yet barely studied in controlled human trials. Its popularity is a marketplace phenomenon, not a reflection of accumulating clinical evidence.1,8,12
The bottom line on evidence: the mechanism is solid and the tanning effect is real at the level of tiny pilot data, but there has never been a completed large-scale efficacy or safety trial of Melanotan II as a tanning agent. Any statement stronger than “it engages a known pigment pathway and darkened skin in a handful of early subjects” overreaches the data. For a research-education audience, the appropriate framing is that MT-II is a mechanistically validated but clinically unproven tool — interesting to study, but not demonstrated to be safe or effective for human pigmentation.1,8
Comparisons With Related Compounds
Melanotan II is best understood alongside its relatives, because the differences are often the source of public confusion — and of misplaced safety assumptions. The most consequential comparison is with afamelanotide (Melanotan I / Scenesse). Afamelanotide is a linear 13-amino-acid α-MSH analog that is relatively selective for MC1R, and it is a genuinely approved medicine: the U.S. Food and Drug Administration approved it in October 2019 (the European Medicines Agency in 2014) as a controlled-release subcutaneous implant to increase pain-free light exposure in adults with erythropoietic protoporphyria (EPP), a rare inherited photosensitivity disorder.12 The temptation to reason “afamelanotide is approved, so Melanotan II must be roughly the same” is exactly the error to avoid: they are different molecules, with different receptor selectivity, different delivery, a different (narrow) indication, and vastly different regulatory status.
The table below contrasts the key melanocortin compounds discussed in this article.
| Compound | Structure | Receptor profile | Regulatory status |
|---|---|---|---|
| α-MSH (endogenous) | Linear 13-aa peptide | Broad melanocortin, very short-lived | Natural hormone |
| Afamelanotide (Melanotan I) | Linear 13-aa analog | Relatively MC1R-selective | FDA/EMA approved for EPP only |
| Melanotan II | Cyclic 7-aa analog | Non-selective (MC1R/3R/4R/5R) | Not approved; research chemical |
| Bremelanotide (PT-141) | MT-II metabolite, cyclic | MC3R/MC4R-oriented | FDA approved for HSDD in women |
A second key comparison is with bremelanotide (PT-141), which is chemically a metabolite of Melanotan II. When the pigmentation program observed that MT-II caused erections through central MC4R activity, developers pursued that effect separately, yielding bremelanotide — now an FDA-approved injectable for hypoactive sexual desire disorder in premenopausal women. This shared lineage explains why MT-II reliably produces sexual side effects and why some educational resources discuss the two together, such as the DosagePeptide references for PT-141 and the Melanotan II and PT-141 combination. The pharmacological point for a researcher is that MT-II’s non-selectivity is not incidental — it is why one “tanning” molecule spins off both an approved sexual-function drug and a cascade of off-target effects.6,7
Finally, MT-II is sometimes compared to endogenous α-MSH itself. The comparison highlights why the synthetic peptide behaves so differently: α-MSH is exquisitely regulated and degraded within seconds, so its pigmentary signaling is tightly controlled, whereas MT-II is engineered to resist degradation and to hit the receptor family hard and for a long time. In other words, MT-II is not “natural α-MSH in a vial” — it is a deliberately supraphysiological agonist. That distinction is the difference between a fine-tuned physiological signal and a blunt pharmacological override, and it underlies much of the safety discussion that follows.1,2
Research Models and Methodology
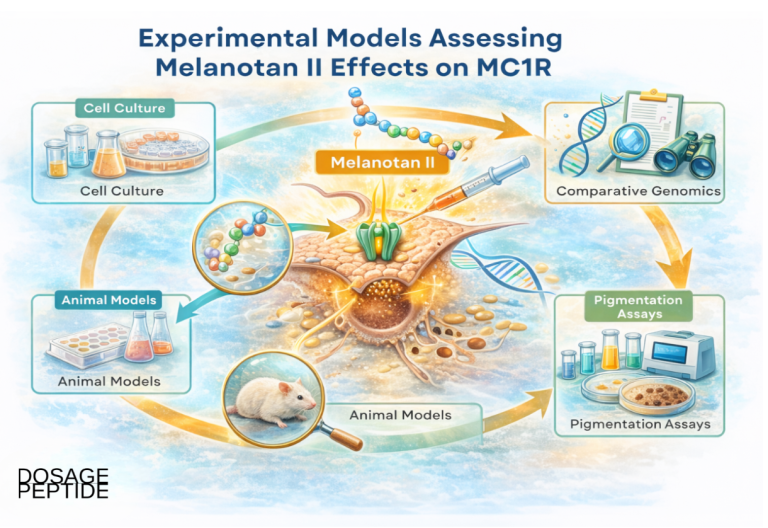
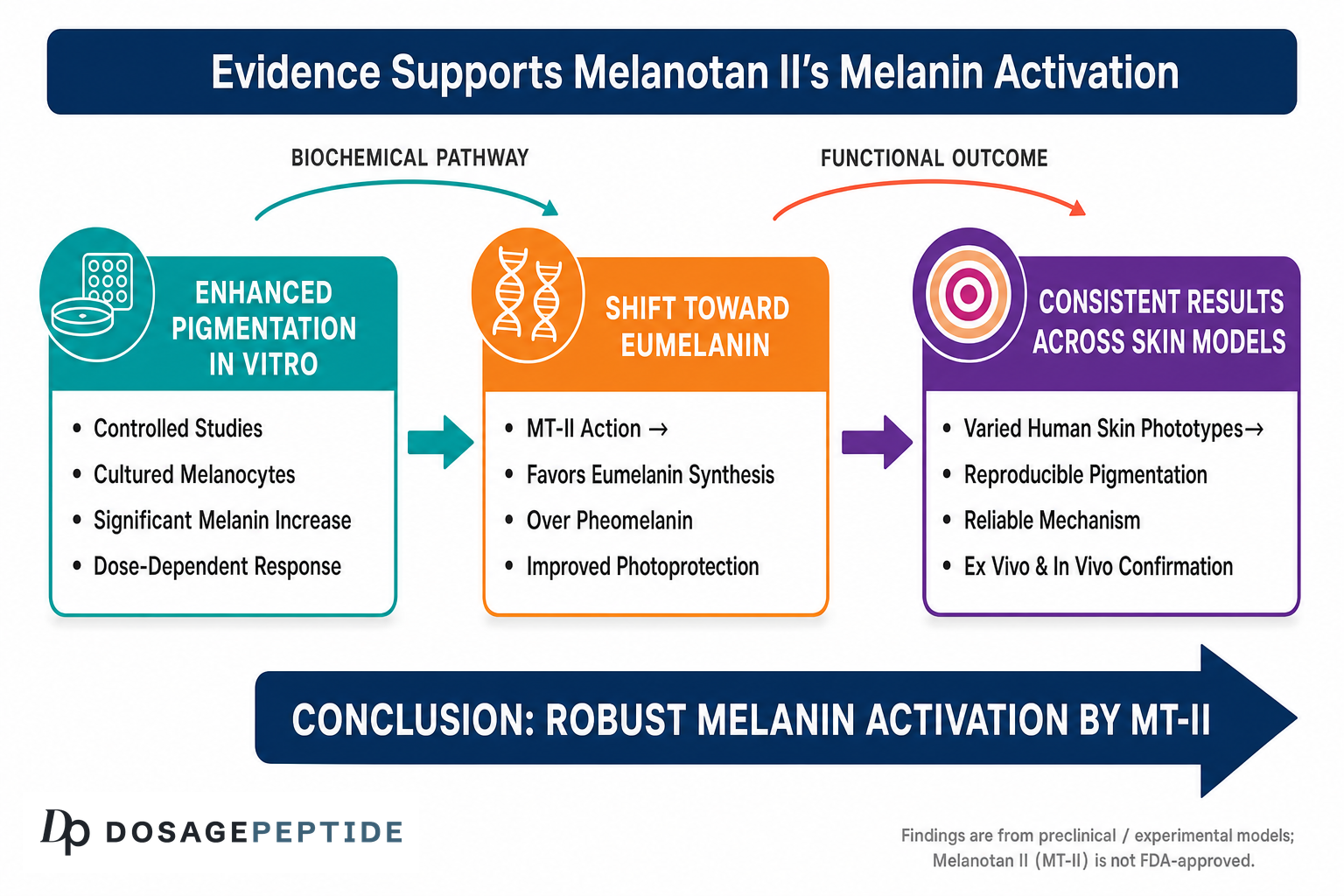
Scientists studying how Melanotan II influences melanin rely on a layered set of models, each answering a different question. At the most fundamental level are in vitro cell models: cultured melanocytes (human or murine, including classic B16 mouse melanoma lines) and melanocyte–keratinocyte co-cultures. In these systems, researchers can add an MC1R agonist and directly measure the mechanistic readouts described earlier — intracellular cAMP accumulation, PKA and CREB phosphorylation, MITF expression, tyrosinase enzyme activity, and total melanin content (typically quantified spectrophotometrically). These assays are what establish, unambiguously, that MC1R agonism raises tyrosinase activity and eumelanin output.3
Historically, melanotropic peptide bioactivity was also assayed in amphibian and reptile skin models — the frog and lizard skin darkening bioassays were classic tools in the Hadley/Hruby program for ranking the potency of α-MSH analogs, and MT-II was identified as “superpotent” partly through such comparative pharmacology. Rodent models add the ability to study systemic pharmacokinetics, tissue distribution, and, in some lines, tumor biology. Notably, one line of laboratory work has examined topical MT-II in melanoma models, reporting suppression of tumor growth via PTEN upregulation and cyclooxygenase-2 inhibition — a reminder that melanocortin signaling in cancer is complex and context-dependent rather than uniformly pro- or anti-tumor.17
In humans, the central methodological tool for measuring pigmentation is reflectance spectrophotometry (and related colorimetry), which quantifies skin darkening objectively rather than relying on subjective visual grading. The Dorr pilot study used exactly this approach, combining quantitative reflectance with visual assessment to document increased pigmentation at defined body sites after subcutaneous dosing.1 Human studies also incorporate pharmacokinetic sampling (plasma peptide concentrations over time) and structured adverse-event monitoring — the latter being how the characteristic nausea, flushing, and erection signals were captured. The table below maps model types to the questions they answer.
| Model | Primary question answered | Typical readouts |
|---|---|---|
| Cultured melanocytes | Does MC1R agonism drive the pigment pathway? | cAMP, MITF, tyrosinase activity, melanin content |
| Frog/lizard skin bioassay | How potent is the analog vs α-MSH? | Darkening / melanosome dispersion |
| Rodent models | Pharmacokinetics, distribution, tumor biology | Plasma levels, tissue pigment, tumor endpoints |
| Human pilot trials | Does it darken human skin, and how is it tolerated? | Reflectance spectrophotometry, PK, adverse events |
An important methodological point for anyone reading the pigmentation literature is the distinction between constitutive and facultative pigmentation, and how studies attempt to control for it. Constitutive pigmentation is a person’s baseline, genetically determined skin color in the absence of sun; facultative pigmentation is the additional tanning induced by a stimulus such as UV — or, in these experiments, an MC1R agonist. Rigorous studies measure sun-protected body sites (such as the buttock or inner upper arm) precisely because unintended ambient UV exposure would otherwise confound the readout, making it impossible to attribute darkening to the peptide rather than to incidental sunlight. The Dorr pilot’s use of protected sites and quantitative reflectance reflects this care. Real-world, uncontrolled use offers no such controls: users are simultaneously exposed to sun, so any darkening they observe cannot cleanly be credited to the peptide alone. This is one more reason anecdotal “it worked for me” reports sit far below controlled measurement in the evidence hierarchy.1,4
A methodological caveat runs through all of this: the human work is small, old, and heterogeneous, and much of what circulates as “evidence” today is instead real-world case reporting from unregulated use — a fundamentally different and lower tier of evidence than a controlled trial. Analytical-chemistry methodology matters here too, because grey-market products are frequently impure or mislabeled; Breindahl and colleagues used LC-UV-MS/MS specifically to characterize what illegal internet tanning products actually contained, and the answer was often “not what the label claimed.”9 Any researcher interpreting the MT-II literature must therefore separate rigorous laboratory mechanism from anecdotal human outcomes.
Safety and Tolerability
Safety is the area where Melanotan II most clearly departs from any reassuring narrative, and it deserves the most careful treatment. Even in the controlled pilot setting, tolerability was poor: the Dorr phase-I study reported dose-dependent nausea, facial flushing, and spontaneous penile erections at doses as low as 0.01–0.03 mg/kg, and the Wessells sexual-function studies likewise reported frequent nausea and yawning, with severe nausea in a meaningful minority of subjects at 0.025 mg/kg.1,6 Nausea, appetite suppression, flushing, and yawning are essentially expected consequences of non-selective central melanocortin activation, not rare idiosyncrasies.
The more serious concerns come from real-world case reports and small case series accumulated as unregulated use spread. Documented and reviewed events include:
- Change in moles and new naevi. Multiple case reports describe darkening and enlargement of existing melanocytic naevi and eruption of new atypical naevi after melanotan use — a plausible consequence of strongly stimulating melanocytes. A widely discussed case involved a patient developing crops of new atypical naevi within about a week of injection, with lesions regressing after discontinuation.8,15
- Melanoma. Several case reports describe melanoma diagnosed during or shortly after melanotan use. Causation cannot be established from case reports, but the biological concern — driving proliferation of melanocytic cells in predisposed individuals — is taken seriously in the dermatology literature.8,16
- Systemic toxicity and rhabdomyolysis. A case report documented systemic toxicity with rhabdomyolysis and acute kidney injury following injection.14
- Renal infarction and cardiovascular effects. A case report/review describes renal infarction associated with melanotan II use in a previously normotensive man, and hypertension and other cardiovascular signals have been reported.13
- Priapism. As a direct extension of its central MC4R activity, MT-II can cause prolonged, painful erections requiring medical intervention.6,8
Layered on top of these pharmacological risks is a product-quality risk that is specific to the unregulated marketplace. Because MT-II is sold as an unlicensed powder for self-reconstitution and injection, users face non-sterile preparation, inaccurate labeling, dosing errors, and unknown impurities — the analytical work by Breindahl and colleagues confirmed that internet tanning products frequently did not match their labels.9 Injecting an unverified peptide compounds every biological hazard with a manufacturing and sterility hazard.
The dermatologic concern around naevi and melanoma deserves particular emphasis because it directly involves the same cells the peptide is designed to stimulate. Melanocytes are, biologically, the precursor cells of melanoma, and MT-II is a potent, sustained stimulus to melanocyte activity. A published case describing a patient with a history of melanoma and multiple dysplastic nevi is illustrative: after self-administering synthetic α-MSH, the patient developed crops of new pigmented nevi with atypical features and darkening of pre-existing nevi, which then progressively lightened and lost growth features after the peptide was discontinued. Case reports cannot establish that MT-II causes melanoma — the temporal association and small numbers do not permit that conclusion — but they raise a mechanistically coherent concern that clinicians take seriously, especially in individuals who already carry atypical moles or a personal or family history of skin cancer. At minimum, MT-II can obscure the early visual warning signs of melanoma by darkening and changing existing lesions, complicating the very surveillance that catches skin cancer early.8,15,16
The honest summary is that Melanotan II has no established safety profile in the sense that regulators require. There has never been a completed large-scale safety trial for tanning, the true incidence of serious events is unknown, and the documented signals span dermatologic, renal, cardiovascular, and urologic systems. Health authorities have responded accordingly — the Australian TGA and others explicitly warn consumers not to use melanotan tanning products, and dermatology resources such as DermNet describe the compound as unlicensed and potentially hazardous.10,11,18 Nothing in the pigment mechanism offsets these concerns.
Handling and Reconstitution in a Research Context
Because Melanotan II is supplied to laboratories as a lyophilized (freeze-dried) powder, handling and reconstitution are practical questions in any bench setting — but they must be framed strictly as laboratory technique, not as instructions for human use. In a research context, the peptide is typically reconstituted with sterile or bacteriostatic water to a defined stock concentration, aliquoted, and stored cold. General peptide-handling principles that apply include gentle reconstitution (directing the diluent against the vial wall rather than forcefully onto the powder), avoiding vigorous shaking that can shear the peptide, and minimizing freeze–thaw cycles that degrade stock solutions.5
The stability characterization by Lan, Ugwu, and colleagues is directly relevant here: their preformulation work examined MT-II’s physicochemical stability precisely because a candidate peptide’s utility depends on how it behaves in solution, at various pH values and temperatures, over time. Lyophilized peptide is generally stored frozen and protected from light; once reconstituted, aqueous stock is kept refrigerated and used within a limited window, as peptides in solution are more prone to hydrolysis and oxidation than the dry powder.5 The table below gives illustrative laboratory-handling parameters (values are typical ranges reported for peptide stocks generally and should be verified against a specific reference standard’s certificate of analysis).
| Parameter | Typical laboratory practice |
|---|---|
| Supplied form | Lyophilized powder (research reference material) |
| Reconstitution diluent | Sterile or bacteriostatic water, added gently to vial wall |
| Lyophilized storage | Frozen, typically around −20 °C or below, protected from light |
| Reconstituted storage | Refrigerated (about 2–8 °C); used within a short window |
| Key degradation risks | Repeated freeze–thaw, heat, light, vigorous agitation |
For readers who work with peptide stocks and need to calculate concentrations for in vitro dosing, DosagePeptide provides general reconstitution and concentration tools, including a reconstitution and dosage calculator and the broader library of dosage references. These are useful for the arithmetic of preparing a defined-concentration solution in a laboratory, but it must be stated plainly: none of this constitutes endorsement of administering Melanotan II to humans. The reconstitution details exist because researchers legitimately need to prepare and store reference material; they do not transform an unapproved research chemical into a safe product. The line between “here is how a peptide stock is handled at the bench” and “here is how to use it” is a bright one, and this article stays firmly on the laboratory side of it.9,11
Limitations and the Human-Evidence Gap
Stepping back, the single most important thing to understand about Melanotan II is the size of the gap between its mechanistic plausibility and its actual human evidence. Mechanistically, the story is elegant and well supported: MC1R agonism drives the cAMP–PKA–CREB–MITF–tyrosinase cascade and increases eumelanin. But mechanistic plausibility has never been a substitute for clinical evidence, and here the clinical evidence is strikingly thin. The foundational tanning data come from a three-person pilot study; there is no completed phase 2 or phase 3 trial establishing efficacy, optimal dosing, or safety for pigmentation.1,8
Several specific limitations compound this gap. First, sample sizes are tiny, so estimates of both effect size and adverse-event frequency are unstable — a side effect that appears in one of three people tells you almost nothing precise about its true rate. Second, the studies are old and short, meaning long-term consequences (especially the melanoma question, which unfolds over years) are entirely unaddressed by controlled data. Third, much of the “human experience” that exists is uncontrolled real-world use of unregulated products, which cannot distinguish drug effects from impurity effects, dosing errors, or coincidence. Fourth, publication and reporting are skewed toward adverse events in case reports rather than systematic outcome measurement, so the literature is better at flagging harms than at quantifying benefit.8,9
There is also a conceptual limitation worth naming for a research audience: even if MT-II reliably produced a tan, a UV-independent tan is not the same as UV protection in any proven sense. The assumption that pharmacologically induced pigment confers meaningful photoprotection — and therefore reduces skin-cancer risk — was the original chemopreventive hypothesis, but it was never demonstrated in outcome trials for MT-II, and the concurrent signals around naevi and melanoma cut in the opposite direction. Some users also reduce sun-avoidance behavior because they feel “protected,” a behavioral risk that no pigment mechanism addresses.8
Finally, it is worth being explicit that “research chemical” status is itself a limitation, not a loophole. When a compound has not passed through regulated clinical development, there is no manufacturer accountability, no standardized formulation, no pharmacovigilance system collecting adverse events, and no approved labeling to define contraindications or drug interactions. Everything that a prescription drug’s label would normally tell a clinician — who should avoid it, what it interacts with, what monitoring is required — simply does not exist for Melanotan II. That informational vacuum is why case reports, rather than trial data, dominate the human record: harms surface anecdotally in emergency departments and dermatology clinics because no structured system was ever built to capture them. For a compound that is injected and acts on melanocytes and multiple central receptors, that absence of oversight is a substantive risk in its own right.8,9,11
For obscure or lightly studied peptides generally, and for Melanotan II specifically, the responsible scientific posture is candor: the receptor pharmacology is real and interesting, but rigorous, independent, adequately powered human evidence is scarce to nonexistent for the tanning application. Claims that MT-II is a proven, safe, or effective way to tan are not supported by the primary literature. It remains an experimental compound whose most robust “human data” are, paradoxically, its documented harms rather than its benefits.1,8,13,14
Regulatory Status
The regulatory picture is unambiguous and important. In the United States, Melanotan II is not approved by the FDA for any indication, and it has never been. It is not a dietary supplement and not a cosmetic; it is an unapproved new drug when marketed for human use. The FDA has taken enforcement action against sellers — notably a 2007 warning letter to Melanocorp for marketing injectable Melanotan II as an unapproved new drug over the Internet — and the agency has advised people using it to stop and consult a physician about any adverse events.10
Internationally the message is consistent. Australia’s Therapeutic Goods Administration (TGA) states plainly that melanotan is not approved for sale or use as a tanning agent, that supplying tanning products containing melanotan without a prescription is illegal regardless of formulation (spray, tablet, injection, or cream), and that these products have not been assessed for quality or safety; the TGA has run large enforcement campaigns against unlawful online promotions.11 In the United Kingdom, the Medicines and Healthcare products Regulatory Agency (MHRA) has repeatedly acted against vendors, treating unlicensed Melanotan II as an illegal, unlicensed medicine. Across these jurisdictions the common thread is that grey-market MT-II is not a lawful consumer product.11,18
The one place where a related molecule is approved deserves careful restatement to prevent confusion: afamelanotide (Scenesse), the linear MC1R-selective Melanotan I analog, is approved by the FDA (2019) and EMA (2014) — but only as a physician-implanted controlled-release device for the rare disease erythropoietic protoporphyria, and only to increase pain-free light exposure. That narrow, disease-specific approval of a different molecule says nothing about the legality or safety of Melanotan II, and it must not be read as an implicit endorsement of MT-II. Likewise, bremelanotide (an MT-II metabolite) is approved for a sexual-desire disorder in women — again a distinct molecule with a distinct indication.12
In short: Melanotan II sits entirely outside the approved-drug framework. It is legitimately used only as a research chemical / reference material in appropriately controlled laboratory settings, and its sale as a tanning product to consumers is prohibited and actively enforced against in major regulatory jurisdictions. Any educational discussion of the compound — including this one — should treat it as experimental, not therapeutic.10,11,12
Frequently Asked Questions
How does Melanotan II actually make skin darker?
It activates the melanocortin-1 receptor (MC1R) on pigment-producing melanocytes. That triggers a cAMP–PKA–CREB signaling cascade, raises the master pigment transcription factor MITF, and increases the enzyme tyrosinase — which converts tyrosine into eumelanin, the brown-black pigment. Because it drives this pathway downstream of ultraviolet light, MC1R agonism can, in principle, darken skin without sun exposure. This mechanism is well established in cell biology, but demonstrating it in a pathway is different from proving safe, reproducible results in people.2,3
Is Melanotan II approved or legal?
No. Melanotan II is not approved by the FDA (or the EMA) for any use, and selling it as a tanning agent is illegal in Australia, the UK, and elsewhere. Regulators including the FDA and TGA have issued warnings and taken enforcement action. It is legitimately handled only as a research chemical in controlled laboratory settings, not as a consumer product.10,11
Is it the same thing as afamelanotide or Scenesse?
No, and this is a common and consequential confusion. Afamelanotide (Melanotan I / Scenesse) is a different, linear, more MC1R-selective peptide that IS FDA/EMA approved — but only as a physician-administered implant for the rare disease erythropoietic protoporphyria. Melanotan II is a distinct cyclic, non-selective peptide with no approval. The approval of one does not extend to the other.12
How strong is the scientific evidence that it tans skin in humans?
Weak in terms of trial quality. The core human tanning data come from a 1996 pilot study in just three volunteers, which did show measurable pigmentation by reflectance but also dose-limiting side effects. No large phase 2 or phase 3 trial of Melanotan II for tanning has ever been completed. Most additional human data concern sexual function, and much of the remaining “evidence” is adverse-event case reports.1,8
What are the main safety concerns?
Even in controlled studies, nausea, flushing, and spontaneous erections were common. Real-world case reports describe darkening and change of moles, new atypical naevi, melanoma diagnosed during use, rhabdomyolysis with kidney injury, renal infarction, hypertension, and priapism. Added to these biological risks is product risk: unregulated MT-II is often impure or mislabeled and is self-injected non-sterilely. There is no established safety profile.8,13,14,9
Why does a “tanning” peptide cause nausea and erections?
Because Melanotan II is non-selective. In addition to the pigment receptor MC1R, it activates central melanocortin receptors MC3R, MC4R, and MC5R. MC4R activity in particular drives sexual arousal and erections, while central melanocortin activation also produces nausea, yawning, and appetite suppression. The same non-selectivity that makes it “superpotent” is why it produces effects far beyond the skin — and it is why the MT-II metabolite bremelanotide became a separate sexual-function drug.1,6
Does a Melanotan II tan protect against UV damage or skin cancer?
This has not been proven, and it should not be assumed. The original chemopreventive hypothesis — that induced eumelanin would reduce UV harm — was never confirmed in outcome trials for MT-II, and the concurrent signals around naevi and melanoma point the other way. A pharmacologically induced tan is not demonstrated to confer meaningful photoprotection, and some users may increase risk by reducing sun-avoidance behavior.8
How is Melanotan II handled in a laboratory setting?
As a lyophilized powder reconstituted with sterile or bacteriostatic water to a defined stock concentration, stored frozen when dry and refrigerated once in solution, with freeze–thaw cycles minimized to preserve stability. These are bench-handling practices for reference material only. General concentration math can be worked out with tools like the DosagePeptide dosage calculator, but handling instructions are not an endorsement of human use.5
References
- Dorr RT, Lines R, Levine N, et al. Evaluation of melanotan-II, a superpotent cyclic melanotropic peptide in a pilot phase-I clinical study. Life Sciences. 1996;58(20):1777–1784. PubMed: https://pubmed.ncbi.nlm.nih.gov/8637402/
- Herraiz C, et al. The α-melanocyte-stimulating hormone/melanocortin-1 receptor interaction: a driver of pleiotropic effects beyond pigmentation. Pigment Cell & Melanoma Research. 2021. https://onlinelibrary.wiley.com/doi/10.1111/pcmr.12980
- García-Borrón JC, et al. MC1R signaling: intracellular partners and pathophysiological implications. Biochimica et Biophysica Acta. 2017. https://www.sciencedirect.com/science/article/pii/S0925443917300765
- Ugwu SO, Blanchard J, et al. Skin pigmentation and pharmacokinetics of melanotan-I in humans. Biopharmaceutics & Drug Disposition. 1997;18(3):259–269. PubMed: https://pubmed.ncbi.nlm.nih.gov/9113347/
- Lan EL, Ugwu SO, Blanchard J, et al. Preformulation studies with melanotan-II: a potential skin cancer chemopreventive peptide. Journal of Pharmaceutical Sciences. 1994. https://www.sciencedirect.com/science/article/abs/pii/S0022354915495474
- Wessells H, Levine N, Hadley ME, Dorr R, Hruby V. Melanocortin receptor agonists, penile erection, and sexual motivation: human studies with Melanotan II. International Journal of Impotence Research. 2000. PubMed: https://pubmed.ncbi.nlm.nih.gov/11035391/
- Wessells H, et al. Effect of an alpha-melanocyte stimulating hormone analog on penile erection and sexual desire in men with organic erectile dysfunction. Urology. 2000. PubMed: https://pubmed.ncbi.nlm.nih.gov/11018622/
- An unhealthy glow? A review of melanotan use and associated clinical outcomes. 2015. https://www.sciencedirect.com/science/article/abs/pii/S2211266915000055
- Breindahl T, et al. Identification and characterization by LC-UV-MS/MS of melanotan II skin-tanning products sold illegally on the Internet. Drug Testing and Analysis. 2015. https://analyticalsciencejournals.onlinelibrary.wiley.com/doi/10.1002/dta.1655
- U.S. Food and Drug Administration. Warning Letter: Melanocorp, Inc. (injectable Melanotan II marketed as an unapproved new drug). 2007. https://www.fda.gov/
- Therapeutic Goods Administration (Australia). Don’t risk using tanning products containing melanotan. https://www.tga.gov.au/news/blog/dont-risk-using-tanning-products-containing-melanotan
- Scenesse (afamelanotide) FDA approval history (October 2019); EMA approval 2014. Drugs.com. https://www.drugs.com/history/scenesse.html
- Melanotan II: a possible cause of renal infarction — review of the literature and case report. 2020. https://www.researchgate.net/publication/338672018
- Melanotan II injection resulting in systemic toxicity and rhabdomyolysis (case report/response). https://www.researchgate.net/publication/232809914
- Change in moles linked to use of unlicensed “sun tan jab” / eruptive melanocytic naevi following melanotan (case reports). BMJ and related. https://www.researchgate.net/publication/23953808
- Melanoma associated with the use of Melanotan-II (case report). https://www.researchgate.net/publication/259394012
- Topical MTII therapy suppresses melanoma through PTEN upregulation and cyclooxygenase-II inhibition. PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7013727/
- DermNet NZ. Melanotan II. https://dermnetnz.org/topics/melanotan-ii
Educational and research-use disclaimer: This article is provided strictly for scientific education and research reference. It is not medical advice, and nothing here should be interpreted as a recommendation to obtain, prepare, or use Melanotan II in humans. Melanotan II is an unapproved, unregulated research chemical; it is not approved by the FDA or comparable authorities as a tanning agent or for any other indication, and its sale for human use is prohibited in multiple jurisdictions. It carries documented and potentially serious risks, and products sold online are frequently impure or mislabeled. Any laboratory handling described above pertains only to work with reference material by qualified researchers in appropriately controlled settings. Individuals with questions about skin health, pigmentation disorders, moles, or photoprotection should consult a licensed physician or dermatologist.