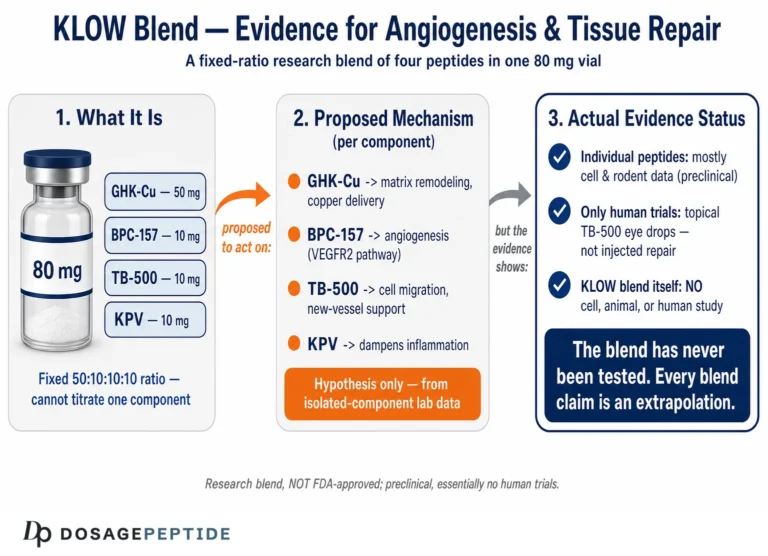
The research question behind this article is narrow and important: does clinical evidence actually support KLOW’s impact on skin elasticity? The honest answer, stated plainly at the outset, is that no human clinical trial has ever evaluated the KLOW blend as a formulation. KLOW is a vendor-assembled research combination, most commonly built from four separate peptides — GHK-Cu, BPC-157, TB-500 (thymosin β4 fragment), and KPV — and the elasticity-related evidence that exists sits entirely at the individual-component level, largely in vitro and in animal models.
That distinction matters for anyone evaluating this compound scientifically. This article separates what is genuinely known from what is extrapolated: it maps the component-level mechanisms that plausibly touch skin elasticity, weighs the strength of the underlying studies, and is explicit about where the evidence stops. KLOW and its components are research chemicals for laboratory and experimental use only — none are approved by the FDA or comparable regulators for human therapeutic use, and nothing here is medical advice.
Is There Any Clinical Research on KLOW Itself?
No. A literature search returns no peer-reviewed clinical trials, cohort studies, or even case reports on “KLOW” as a defined multi-peptide product. KLOW is not a pharmaceutical with an INN (International Nonproprietary Name), a registered trial history, or a pharmacopeial monograph. It is a blend name used by peptide suppliers, and its exact composition and ratios can vary between vendors. The most commonly cited formula pairs a copper tripeptide (GHK-Cu) with two regenerative peptides studied mainly in wound and musculoskeletal models (BPC-157 and TB-500) and an anti-inflammatory α-MSH fragment (KPV).
Because of that, any statement about “KLOW’s effect on skin elasticity” is necessarily a statement about its parts. When a supplier or blog claims KLOW improves skin elasticity, the underlying data — where any exists — comes from studies on one of these four peptides in isolation, usually GHK-Cu, and usually not in the combination, dose, ratio, or delivery route that KLOW is sold in. The combined pharmacology of the four together (synergy, interference, altered stability, copper interactions) has not been formally characterized in any published study.
The reader should therefore treat elasticity claims as mechanistically plausible for one component (GHK-Cu) and speculative for the blend. The sections below hold to that framing. For the practical research parameters researchers use when handling the blend, the dedicated KLOW 80 mg vial dosage protocol documents reconstitution and handling conventions; it is a research reference, not a treatment recommendation.
What Are the Four KLOW Components and Which One Drives the Elasticity Rationale?
Skin elasticity is a biomechanical property governed largely by two extracellular matrix (ECM) networks — collagen (mainly types I and III, providing tensile strength) and elastin (providing recoil) — plus the proteoglycans and glycosaminoglycans (GAGs) that hydrate and organize the matrix. Elasticity declines with age as elastin fragments, collagen cross-linking becomes disordered, and fibroblast synthetic capacity falls. Any peptide that plausibly affects elasticity must touch one of these processes. Here is how each KLOW component maps onto that biology.
| Component | Class / origin | Primary studied action | Relevance to skin elasticity | Strongest evidence level |
|---|---|---|---|---|
| GHK-Cu | Copper-binding tripeptide (Gly-His-Lys) native to human plasma | Modulates ECM gene expression; supplies copper to lysyl oxidase; balances MMP/TIMP activity | Direct — upregulates collagen, elastin, decorin, GAGs; cross-linking cofactor | In vitro + limited human topical trials |
| BPC-157 | Synthetic pentadecapeptide from a gastric protein fragment | Angiogenesis, fibroblast activity, growth-factor receptor upregulation | Indirect — supports granulation tissue, collagen deposition in wound repair | Rodent / in vitro preclinical only |
| TB-500 (Tβ4 fragment) | Synthetic fragment related to thymosin β4, an actin-sequestering peptide | Cell migration, angiogenesis, anti-inflammatory signaling | Indirect — promotes keratinocyte/fibroblast migration, matrix remodeling in wounds | Rodent / in vitro preclinical only |
| KPV | C-terminal tripeptide (Lys-Pro-Val) of α-MSH | Anti-inflammatory; suppresses NF-κB and pro-inflammatory cytokines | Indirect — reduces inflammatory ECM degradation environment | In vitro / preclinical |
The pattern is clear: GHK-Cu is the only component with a direct, mechanistically specific, and partially human-tested link to skin elasticity. The other three are regenerative or anti-inflammatory peptides whose connection to elasticity is inferential — they support the wound-healing and matrix-turnover milieu in which collagen and elastin are produced, but they are not elastin- or collagen-specific agents, and their skin data are preclinical. Researchers comparing the copper peptide alone to the blend often consult the GHK-Cu 50 mg vial dosage protocol to isolate that variable, and the BPC-157 / TB-500 blend protocol for the regenerative pair.
What Actually Determines Skin Elasticity at the Tissue Level?
To judge whether any peptide can influence elasticity, it helps to be precise about what elasticity is. In dermatology and biomechanics, skin elasticity refers to the tissue’s ability to deform under load and then return to its original shape — quantified by parameters such as the extensibility, the elastic-recovery ratio, and the viscoelastic creep measured by suction cutometry. These properties emerge from the interplay of three matrix systems, and a peptide can only affect elasticity if it touches one of them.
- The elastic-fiber network is the dedicated recoil system: elastin cores wrapped in fibrillin microfibrils, cross-linked by copper-dependent lysyl oxidase into desmosine and isodesmosine bonds. This network provides the spring that returns stretched skin to baseline. It is laid down mostly early in life and is poorly replaced in adults, which is why elastic-fiber damage is largely cumulative.
- The collagen network (predominantly types I and III) supplies tensile strength and limits over-extension. Collagen turns over more readily than elastin, and its organization — fiber diameter, alignment, cross-link maturity — strongly influences how skin resists and recovers from deformation.
- The ground substance — proteoglycans and glycosaminoglycans such as versican, decorin, hyaluronan, and chondroitin sulfate — hydrates the matrix, spaces the fibers, and contributes the viscous, time-dependent component of skin’s viscoelastic behavior.
Aging and photodamage degrade all three: elastic fibers fragment and clump (solar elastosis), collagen becomes sparse and disorganized, and proteoglycan content shifts. Loss of measurable recoil is the downstream result. This is why the GHK-Cu evidence is mechanistically interesting — it is one of very few molecules reported to act on collagen, elastin, and proteoglycan gene expression and the copper-dependent cross-linking enzyme simultaneously. It also explains why gene-expression data alone are insufficient: elasticity is ultimately a fiber-architecture and cross-link property, a point the measurement section below develops in full.
What Mechanisms Underlie GHK-Cu’s Effect on Collagen and Elastin?
GHK-Cu (glycyl-L-histidyl-L-lysine bound to copper(II)) is the mechanistic centerpiece of the KLOW elasticity story, and it is the best-characterized of the four peptides. Discovered by Loren Pickart in 1973 as a plasma factor that restored synthetic activity in aged tissue, GHK is present naturally in human plasma at roughly 200 ng/mL at age 20, declining to about 80 ng/mL by age 60 — a fall that parallels the age-related loss of regenerative capacity.[5]
Gene-level modulation of the extracellular matrix
The most striking data on GHK-Cu come from transcriptomic analysis. Pickart and Margolina’s 2018 review, drawing on Broad Institute Connectivity Map data, reported that GHK altered the expression of a very large fraction of assayed human genes — on the order of ~30% at a ≥50% change threshold — with enrichment in pathways governing collagen synthesis, antioxidant response, DNA repair, and matrix remodeling.[6] In fibroblast systems, GHK-Cu upregulates genes for type I and III collagen, elastin, and the proteoglycans decorin, dermatan sulfate, and chondroitin sulfate — the full structural toolkit of elastic dermis.[5]
Copper delivery to lysyl oxidase — the cross-linking connection
Elastin recoil depends on cross-linking, and the enzyme responsible, lysyl oxidase (LOX), is copper-dependent. GHK’s high affinity for copper(II) — comparable to the copper-transport site on albumin — lets it act as a physiological copper shuttle, supplying the cofactor that LOX needs to form the desmosine and isodesmosine cross-links that give elastic fibers their durability.[7] This is a mechanistically direct route from GHK-Cu to a physical property of skin, not merely a correlation.
Balanced remodeling, not simple accumulation
Critically, GHK-Cu does not just push collagen synthesis. Pickart’s tissue-remodeling model describes GHK-Cu as simultaneously upregulating matrix metalloproteinases (MMPs) — which clear damaged, disorganized collagen — and their tissue inhibitors (TIMPs), producing orderly turnover rather than uncontrolled deposition or scarring.[7] For elasticity specifically, this matters: young elastic skin is defined by well-organized fiber architecture, not merely by the total quantity of matrix protein. GHK-Cu is best understood as a pleiotropic modulator of ECM homeostasis rather than a single-target growth-factor mimic.
What Does the Direct GHK-Cu Human Evidence Actually Show?
Unlike the other three components, GHK-Cu has been tested topically in human skin. The most cited work is a series of controlled cosmetic studies. In a 12-week facial trial, a GHK-Cu cream applied twice daily to women with photoaged skin produced measurable improvements in skin density, thickness, laxity, clarity, and fine lines relative to vehicle control; a companion periorbital study reported similar firming and density gains in the eye area.[5] Comparative work indicated GHK-Cu increased collagen in a majority of treated subjects, at a rate reported to exceed both vitamin C and retinoic acid comparators in the same analyses.[5]
Two caveats keep this honest. First, these are topical cosmetic studies of GHK-Cu alone, not of KLOW, and not the injectable research context in which the blend is typically discussed. Second, endpoints such as “skin density” and “laxity” are measured by cutometer and ultrasound-style instruments — legitimate but surrogate — rather than by direct histological quantification of elastin cross-link density. The evidence supports GHK-Cu as a genuine ECM-active agent in human skin; it does not validate KLOW, an injectable four-peptide blend, at any dose.

Why Does the Age-Related Decline in GHK Matter for Elasticity?
One of the more compelling threads in the copper-peptide literature is that GHK is not a foreign molecule imposed on skin — it is an endogenous human peptide whose concentration falls sharply with age, from the roughly 200 ng/mL of a 20-year-old to about a third of that by age 60. This framing reframes the elasticity rationale: rather than forcing an unnatural response, supplementing GHK-Cu is hypothesized to restore a signaling molecule that youthful skin already possesses in abundance.
The biology of elastic-fiber aging makes this relevant. Elastin is essentially a lifetime-durable protein — the body lays down most of its elastic-fiber network early in life and has very limited capacity to synthesize functional new elastin in adulthood. Aged, sun-damaged skin shows fragmented elastic fibers (solar elastosis), disorganized collagen, and reduced fibroblast output. A peptide that simultaneously (a) upregulates elastin and collagen transcription, (b) supplies copper to the cross-linking enzyme, and (c) promotes orderly clearance of damaged matrix via balanced MMP/TIMP activity is, in principle, addressing several of these failure modes at once.[7] Whether that translates into measurable recoil improvement in intact human skin — as opposed to gene-expression shifts in culture — is exactly the question that remains only partially answered, and only for topical GHK-Cu monotherapy.
Copper as a double-edged variable
Copper is essential for lysyl oxidase, superoxide dismutase, and other ECM-relevant enzymes, which is why GHK’s copper-shuttling behavior is mechanistically attractive. But copper is also redox-active and can, in excess or in the wrong chemical context, drive oxidative damage. The physiological appeal of GHK-Cu is that it delivers copper in a chaperoned, tightly bound form rather than as free ionic copper — buffering availability to enzymes while limiting uncontrolled redox activity.[6] In a multi-peptide blend like KLOW, this copper chemistry is one more reason the whole cannot be assumed equal to the sum of the parts: the presence of other peptides and the reconstitution environment could, in theory, affect copper coordination, and this has not been studied.
What Does the Evidence Show for Each Ingredient’s Role in Skin — Component by Component?
The sections above establish that GHK-Cu is the elasticity anchor and the other three peptides are regenerative or anti-inflammatory adjuncts. This section goes deeper on each ingredient in turn, grading the evidence honestly at every step. The recurring point is that the quality of data falls off sharply as you move from GHK-Cu (in vitro plus some human topical work) to BPC-157, TB-500, and KPV (preclinical, and mostly not in skin-elasticity contexts at all).
GHK-Cu — the best-evidenced component, and why
GHK-Cu earns its place at the center of the elasticity rationale because its actions on skin have been probed at three distinct levels: transcriptomic, biochemical, and functional. Beyond the collagen/elastin/proteoglycan upregulation and the lysyl-oxidase copper-shuttle mechanism already described, two additional GHK-Cu properties are directly relevant to elastic-tissue quality.
Antioxidant and copper-regulatory activity. A dedicated analysis by Pickart and colleagues reported that GHK-Cu modifies the expression of numerous antioxidant genes and helps regulate cellular copper handling, and that in animal injury models GHK-Cu treatment raised superoxide dismutase (SOD) activity and lowered reactive-oxygen-species levels alongside reductions in pro-inflammatory cytokines.[12] This matters for elasticity because oxidative stress is one of the principal drivers of elastic-fiber fragmentation and disordered collagen cross-linking in photoaged skin; a molecule that both supplies copper to cross-linking enzymes and bolsters the antioxidant defenses that protect those fibers is acting on two sides of the same problem.
Decorin and proteoglycan synthesis. GHK-Cu has been reported to stimulate synthesis of the small proteoglycan decorin in addition to collagen and glycosaminoglycans.[12] Decorin is not incidental to elasticity: it binds collagen fibrils and regulates their diameter and spacing, contributing to the orderly fiber architecture on which functional recoil depends. This reinforces the theme that GHK-Cu is a broad ECM-homeostasis modulator rather than a single-gene inducer. The overall GHK-Cu evidence ladder therefore reads: strong in vitro and transcriptomic support, plausible biochemical mechanism, and limited but real human topical-cosmetic data — the highest tier available for any KLOW component, though still short of controlled injectable-elasticity trials.
BPC-157 — angiogenesis and fibroblast support, entirely preclinical for skin
BPC-157’s skin-relevant evidence is regenerative and preclinical. It is reported to promote angiogenesis, fibroblast activity, and collagen deposition, and to accelerate healing across skin, tendon, ligament, muscle, and gastrointestinal tissue in rodent and in vitro studies.[8] A frequently cited mechanistic detail is that in tendon fibroblasts, BPC-157 upregulated the growth-hormone receptor in a dose- and time-dependent manner, a route proposed to potentiate proliferation and repair.[9] For skin specifically, topical BPC-157 has reduced inflammation and edema and improved collagen deposition and angiogenesis in animal wounds.[8] The honest reading: BPC-157 plausibly enriches the vascular and fibroblast environment in which matrix is rebuilt, but there is no controlled human evidence that it increases skin elasticity, and none of its skin data use elasticity as an endpoint.
TB-500 / thymosin β4 — cell migration and remodeling, preclinical
TB-500 is a synthetic fragment associated with thymosin β4, an actin-sequestering peptide whose defining action is driving cell migration. By sequestering monomeric G-actin and remodeling the cytoskeleton, thymosin β4 promotes keratinocyte and fibroblast movement — the migratory step of re-epithelialization and matrix repopulation — and additionally supports angiogenesis (partly via VEGF), modulates inflammatory cytokines, and influences scar quality through TGF-β isoform balance. In preclinical wound models, thymosin β4 has increased collagen deposition and vascular density versus controls. As with BPC-157, these are wound-repair endpoints in animals; extrapolation to intrinsic dermal elasticity in intact human skin is a rationale, not a demonstrated outcome, and no controlled human elasticity trial exists.
KPV — an anti-inflammatory brake on matrix degradation
KPV is the C-terminal Lys-Pro-Val tripeptide of α-melanocyte-stimulating hormone (α-MSH). It retains the parent hormone’s anti-inflammatory activity while shedding its pigmentary effects. A central part of that activity is inhibition of NF-κB signaling — the α-MSH C-terminal sequence GKPV has been shown to inhibit TNF-α-stimulated NF-κB activity, quieting a master inflammatory switch.[13] Its precise mechanism is not fully resolved: some work supports a cell-surface, receptor-mediated route, while other reports describe a more direct intracellular action, and the balance between the two remains debated. In human keratinocytes, KPV suppresses NF-κB-driven pro-inflammatory output at low concentrations without inducing pigmentation.[11]
The elasticity connection is protective rather than generative. Chronic inflammation upregulates matrix metalloproteinases that degrade collagen and elastin, and it perpetuates the oxidative environment that fragments elastic fibers. A tripeptide that quiets NF-κB signaling could, in principle, lower that degradative pressure and preserve existing matrix. This is a defensible contribution to a regenerative blend — but it is a matrix-protective hypothesis several inferential steps removed from any measured elasticity endpoint, and it has been demonstrated for KPV alone, never within KLOW.
What Do the Regenerative Components (BPC-157, TB-500, KPV) Contribute — and How Strong Is That Evidence?
The three non-copper peptides in KLOW are included on a regenerative rationale rather than a direct elasticity rationale, and — as detailed component-by-component above — their relevance to skin elasticity is indirect and preclinical. What the phased view adds is a way to see how they are meant to fit together. A blend of this kind maps onto the classic phases of tissue repair — inflammation, proliferation, and remodeling. KPV addresses the inflammatory phase by lowering cytokine-driven signaling; BPC-157 and TB-500 act in the proliferative and migratory phase, mobilizing fibroblasts, endothelial cells, and new vasculature (BPC-157 via angiogenesis, fibroblast activity, and growth-hormone-receptor upregulation;[8] TB-500 via actin-sequestering cell migration and VEGF-linked angiogenesis[10]); and GHK-Cu operates in the remodeling phase, tuning matrix synthesis and organized turnover. That phased logic is intellectually tidy, but it describes wound repair, not the intrinsic elasticity of uninjured, aging skin — and the mapping has never been validated for the KLOW blend. Human data for the regenerative trio remain limited to small musculoskeletal pilot investigations, with no controlled evidence that any of them raises skin elasticity as a defined endpoint.
What Biomarkers Quantify Skin Elasticity Changes in These Models?
Because “elasticity” is a composite property, research on these peptides relies on a defined set of molecular and biomechanical readouts, spanning gene expression, matrix chemistry, and instrumental biomechanics. One point deserves emphasis up front, because it governs how every downstream claim should be read: gene expression and staining are reported far more often than direct biomechanical elasticity. When a study reports higher ELN transcription, that is upstream evidence — it does not by itself prove increased functional recoil, which depends on translation, secretion, fiber assembly, and cross-linking. A minimally invasive biomarker platform has also been developed to apply standardized qRT-PCR panels to small skin samples, improving comparability of ECM and elasticity-related markers across experiments.[2] The specific instruments and assays behind each tier — cutometry parameters, collagen and elastin histology, hydroxyproline and desmosine chemistry, and the COL1A1/ELN/VCAN qRT-PCR readout — are detailed in the measurement section further below; the interpretive rule is what matters here: reading these biomarkers correctly is what separates a mechanistic hypothesis from a validated outcome.
How Does the KLOW Rationale Compare With Single-Peptide and Collagen-Peptide Approaches?
It is worth situating KLOW’s multi-peptide logic against the alternatives a researcher might otherwise study, because the comparison clarifies both its appeal and its unproven status.
Multi-peptide blend vs. single peptide
The theoretical case for a blend is broader mechanistic coverage: GHK-Cu handles ECM gene expression and cross-linking, BPC-157 and TB-500 address angiogenesis and cell migration, and KPV dampens the inflammatory degradation environment. In principle these act on different phases of tissue remodeling and could produce layered effects that a single peptide cannot. This is a reasonable hypothesis — but it remains a hypothesis. No head-to-head study has shown that the four-peptide blend outperforms GHK-Cu alone on any elasticity endpoint, and combination pharmacology can just as easily produce interference or reduced stability as synergy. Researchers isolating this question typically compare the full blend against the copper peptide by itself, using the GHK-Cu single-peptide protocol as the control arm.
Peptide signaling vs. exogenous collagen peptides
A different and better-studied approach uses ingested or applied collagen-derived peptides, which are thought to act partly as signaling fragments that stimulate fibroblasts. In cultured human dermal fibroblasts, such collagen peptides significantly increased COL1A1, ELN, and VCAN expression and raised collagen protein,[3] and in D-galactose/UV skin-aging models, collagen and elastin peptides improved structural markers of aging.[4] The mechanistic difference is important: collagen peptides supply substrate-like signaling fragments, whereas GHK-Cu acts as a copper-delivering transcriptional modulator and enzyme cofactor. Both routes converge on the same output — more organized collagen and elastin — but through distinct upstream logic. KLOW belongs to the second, signaling-modulator category, with GHK-Cu as its active elasticity element.
What Research Models and Methodologies Are Used?
The evidence base for these peptides spans a hierarchy of models, and the level of a finding is inseparable from the model that produced it.
In vitro fibroblast and keratinocyte cultures
Monolayer cultures of human dermal fibroblasts are the workhorse for ECM-gene and collagen-synthesis studies. They are reproducible and mechanistically informative — the COL1A1/ELN/VCAN upregulation data and much of the GHK-Cu transcriptomic work come from such systems[3] — but a 2D culture cannot reproduce the layered architecture, mechanical loading, or vascular context of real dermis, and it cannot measure functional elasticity.
3D skin equivalents and organotypic models
Reconstructed skin equivalents (fibroblasts in a collagen matrix under a keratinocyte layer) bridge some of that gap, allowing measurement of matrix organization and, in some designs, mechanical properties. They remain simplified relative to living skin but are the most physiologically relevant in vitro option.
Rodent wound and photoaging models
BPC-157 and TB-500 skin data come almost entirely from rodent wound-healing models — excisional wounds, tendon and muscle injury, and diabetic-impaired healing — with endpoints of closure rate, granulation-tissue histology, angiogenesis, and tensile strength.[8] Photoaging is frequently modeled by combining UV exposure with D-galactose-induced oxidative aging; in such models, collagen and elastin peptides improved skin structural markers and reduced signs of aging.[4] Interspecies differences in skin thickness, healing kinetics, and hair-follicle density limit direct translation to humans.
Bioavailability and delivery — an under-appreciated variable
How a peptide reaches fibroblasts fundamentally shapes any elasticity result. Work on collagen-derived peptides has highlighted that their biological effects are constrained by low bioavailability, motivating research into improving delivery to human dermal fibroblasts.[1] KPV skin-permeation research similarly required iontophoresis across microporated skin to achieve meaningful transdermal delivery.[11] This is a central reason KLOW’s blend-level effect cannot be assumed from component data: the route, formulation, and copper chemistry all change what actually reaches the target cells.
How Should Researchers Handle Reconstitution and Dosing Context?
The following is research-handling context only. KLOW and its components are not approved for human use, and nothing here is a dosing recommendation, a protocol for administration to people, or medical advice. It describes the parameters investigators use to prepare and standardize material for laboratory work.
Multi-peptide blends introduce handling considerations that single peptides do not. Because GHK-Cu carries a copper(II) ion, reconstitution and storage conditions that are fine for a plain peptide can matter more here — copper chemistry is sensitive to pH and oxidation, and blends combine peptides with differing solubility and stability profiles. General best practice in peptide research is to reconstitute with an appropriate diluent (commonly bacteriostatic or sterile water), to avoid vigorous agitation that can shear or denature peptides, to protect solutions from light and heat, and to keep reconstituted material refrigerated and used within a defined window. The step-by-step conventions are covered in the peptide reconstitution guide.
For concentration math — converting a target amount per unit volume into a reconstitution volume for a given vial size — researchers typically use a peptide dosage calculator rather than estimating by eye, since blend vials (such as an 80 mg KLOW vial) contain multiple peptides whose combined mass must be accounted for. The blend-specific parameters are documented in the KLOW dosage protocol. Unfamiliar terms used throughout this literature — ECM, lysyl oxidase, versican, MMP/TIMP — are defined in the site peptide glossary.
Why Are There No Blend-Level Clinical Trials, and What Would Rigorous Evidence Require?
It is worth being explicit about why the KLOW blend has no trials, because the reasons are structural rather than accidental, and they define what a genuinely convincing body of evidence would have to look like.
Formulation science: a blend is not its ingredient list
A multi-peptide product is a formulation, and formulation behavior cannot be read off from a list of ingredients. Combining four peptides — one of them a copper-coordinated tripeptide — introduces variables that do not exist for any component alone: competing solubilities, differential stability and degradation kinetics, potential peptide–peptide interactions, and the real possibility that GHK’s copper(II) coordination is perturbed by the other species or by the reconstitution environment. Because GHK’s utility depends on copper being chaperoned in a tightly bound, redox-buffered form rather than present as free ionic copper, any shift in that coordination chemistry is mechanistically consequential and has not been characterized in KLOW. None of these blend-specific properties can be inferred from single-peptide studies; they have to be measured in the actual formulation.
Additive is the null hypothesis — synergy must be proven, not assumed
Marketing language around blends often implies synergy, but in combination pharmacology additivity is the default expectation and synergy is a claim that requires a specific kind of proof. The established framework is isobolographic analysis: from the dose–response curve of each agent alone, one constructs the isobole — the line of all combination doses expected to produce a given effect under simple additivity. A combination that lands below that line is synergistic; on it, additive; above it, antagonistic (sub-additive).[14] Regulators evaluating fixed-dose combinations generally require a demonstration that the combination outperforms its constituents, precisely because “more ingredients” does not entail “better outcome.” For KLOW, no such analysis exists on any endpoint: it is unknown whether the four peptides together are synergistic, merely additive, or in fact antagonistic or destabilizing for elasticity-relevant outputs.
What a rigorous evidence base would require
A credible demonstration that KLOW improves skin elasticity — as opposed to a demonstration that GHK-Cu does — would need, at minimum:
- Characterization of the actual formulation: identity, purity, and stability of each peptide in the blend, and confirmation that GHK’s copper coordination is intact after reconstitution and storage.
- A defined, fixed composition and route, since vendor blends vary in peptides and ratios and results cannot generalize across undefined formulations.
- Comparison against the right controls, chiefly GHK-Cu monotherapy, to establish whether the additional three peptides add anything to an elasticity endpoint — ideally analyzed isobolographically rather than as a single-arm before/after.
- Direct biomechanical elasticity endpoints (suction cutometry parameters, ex vivo tensile testing, desmosine cross-link chemistry) rather than transcriptional or staining surrogates alone.
- Adequate design: randomization, vehicle or comparator control, blinding, pre-registered endpoints, and a sample size powered for the effect claimed.
Until studies of that shape exist, the correct scientific position is not “KLOW works” or “KLOW fails” but “KLOW is untested as a blend,” with the component evidence — strong for GHK-Cu, preclinical for the rest — standing in for it only as a hypothesis.
How Is Skin Elasticity Actually Measured in Research?
Claims about elasticity are only as trustworthy as the methods behind them, so it is worth understanding exactly how the property is quantified. Researchers work across three tiers — non-invasive instrument measurement on living skin, tissue-level histology and chemistry from biopsies, and in vitro cellular assays — each answering a different question.
Non-invasive biomechanics: suction cutometry
The most widely used instrument for in vivo skin elasticity is the suction cutometer, which applies a controlled negative pressure to draw skin into a probe aperture and optically tracks how far and how quickly it deforms and recovers. From the deformation-versus-time curve it derives a family of viscoelastic parameters. Several are directly interpretable as “elasticity”:
| Parameter | What it captures | Interpretation |
|---|---|---|
| R0 (Uf) | Maximum deformation at end of suction (firmness/pliability) | Lower R0 indicates firmer, tighter skin |
| R2 (Ua/Uf) | Gross elasticity, including viscous deformation | Closer to 1 (100%) = more elastic |
| R5 (Ur/Ue) | Net elasticity: elastic recoil vs. immediate elastic distension | Higher R5 indicates better elasticity |
| R7 (Ur/Uf) | Biological elasticity: immediate recovery vs. total deformation | Declines with age; strong inverse age correlation |
In a correlation study of skin-elasticity parameters against age, R2, R5, and R7 all declined with age, with biological elasticity (R7) showing the strongest negative correlation.[15] These are the same instrumental endpoints used in the GHK-Cu topical cosmetic studies, which is why “skin density” and “laxity” outcomes in that literature are legitimate but instrumental surrogates rather than direct histological measures of elastin cross-link density. A practical caveat: cutometer values depend on probe aperture, applied pressure, anatomical site, hydration, and operator technique, so cross-study comparison requires standardized settings — an active methodological concern in the field.
Tissue-level quantification: biopsy histology and matrix chemistry
To connect a biomechanical change to its structural cause, researchers examine skin tissue directly. Collagen content and organization are assessed by picrosirius red, Masson’s trichrome, and immunofluorescence for type I and III collagen, and quantified biochemically by hydroxyproline assay. Elastic fibers are visualized with elastin-specific stains (e.g., Verhoeff–Van Gieson) to grade fragmentation and solar elastosis. Most specifically, the elastin cross-links desmosine and isodesmosine can be quantified as a chemical index of functional elastic-fiber maturity, and lysyl oxidase activity can be assayed to gauge cross-linking capacity. This tier is the gold standard for elasticity biology because it measures the fibers and cross-links themselves, but it is invasive and therefore used sparingly in human work and predominantly in animal models.
In vitro fibroblast and matrix assays
Upstream of tissue, cellular assays measure whether a compound switches on the machinery of elastic-matrix production. The standard readouts are qRT-PCR of elasticity-linked transcripts — COL1A1 (collagen I), ELN (elastin), and VCAN (versican) — together with secreted-protein quantification and confocal imaging of deposited collagen. In cultured human dermal fibroblasts, for example, collagen peptides significantly increased COL1A1, ELN, and VCAN expression and raised detectable collagen protein.[3] The essential interpretive rule ties the three tiers together: a rise in ELN transcription (in vitro) is upstream of, and does not by itself prove, an increase in desmosine cross-links (tissue) or a measurable gain in R5/R7 recoil (in vivo). Genuine elasticity evidence requires the chain to be demonstrated, not assumed — which is exactly why component gene-expression data cannot be read as blend-level functional proof.
What Are the Limitations and Open Questions?
A scientifically literate reader should weight the following limitations heavily when evaluating any KLOW elasticity claim.
- No blend-level data. Every elasticity-relevant finding is for a single component in isolation. Synergy, antagonism, altered stability, and copper-interaction effects among GHK-Cu, BPC-157, TB-500, and KPV are entirely uncharacterized in published research.
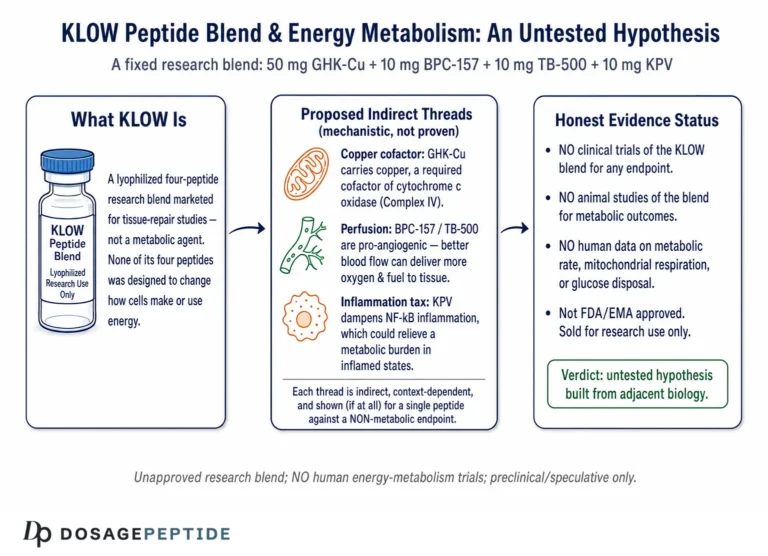
- No KLOW human trials. There are no clinical trials of KLOW at any dose, route, or endpoint. “Clinical research on KLOW” does not exist; the phrase in the title is answered by describing component evidence and stating the gap.
- Elasticity is often inferred, not measured. Much component evidence reports gene expression or collagen staining, which are upstream of functional recoil. Direct biomechanical elasticity endpoints (cutometry, desmosine content) are less commonly reported for these peptides.
- Model-to-human translation gaps. Rodent wound models and 2D fibroblast cultures do not reproduce human dermal architecture, aging biology, or delivery constraints.
- Route and bioavailability unknowns. GHK-Cu’s human elasticity evidence is topical cosmetic; the regenerative components’ evidence is largely injectable in animals. KLOW is discussed in a different context again, and route changes outcome.
- Composition variability. Vendor blends differ in exact peptides and ratios, so even component-level extrapolation is imprecise for any given KLOW vial.
The most valuable open questions are therefore obvious: controlled studies of the actual blend, direct biomechanical elasticity endpoints rather than transcriptional surrogates, and characterization of how the four peptides interact when combined.
What Are the Safety and Handling Considerations in Research?
Safety data track the same component-level, mostly-preclinical pattern as the efficacy data. GHK-Cu is generally reported as well tolerated in topical cosmetic use, though copper-containing preparations warrant attention to formulation and to any copper-sensitivity context. BPC-157 and TB-500 show favorable safety and pharmacokinetic profiles in animal studies, but human safety data are limited to small pilot investigations and are not sufficient to establish a human safety profile.[8] KPV’s anti-inflammatory action, which spares α-MSH’s pigmentary effects, is favorable in principle, but again its evidence is preclinical.
For the laboratory itself, standard research-chemical handling applies: treat these as investigational materials, use appropriate PPE, avoid contamination, maintain a documented chain of custody and lot records, verify identity and purity (e.g., by supplier certificate of analysis and, where possible, independent analysis), and store per stability requirements. The overriding safety statement is regulatory: KLOW and its component peptides are not approved by the FDA or comparable authorities for human therapeutic use, and this article does not endorse or instruct any such use.
Frequently Asked Questions
Is there any clinical trial proving KLOW improves skin elasticity?
No. There are no published clinical trials, cohort studies, or case reports evaluating the KLOW blend for skin elasticity or any other endpoint. All elasticity-relevant evidence comes from studies of individual components in isolation — chiefly GHK-Cu — and mostly from in vitro and animal models. Any claim of “clinical proof” for KLOW itself is unsupported by the peer-reviewed literature.
Which KLOW ingredient actually affects skin elasticity?
GHK-Cu is the only component with a direct, partly human-tested link to elasticity. It upregulates collagen, elastin, and proteoglycan genes and supplies copper to lysyl oxidase, the enzyme that cross-links elastic fibers. BPC-157, TB-500, and KPV contribute regenerative and anti-inflammatory actions that indirectly support matrix health, but they are not elasticity-specific and their skin data are preclinical.
What does GHK-Cu do to collagen and elastin at the molecular level?
In fibroblasts, GHK-Cu upregulates genes for type I and III collagen, elastin, decorin, and glycosaminoglycans, and it balances MMP and TIMP activity to remodel the matrix in an orderly way rather than simply accumulating protein. By delivering copper to lysyl oxidase, it also supports the cross-linking that gives elastic fibers their recoil — a direct route from peptide to a physical skin property.
Are BPC-157 and TB-500 tested for skin elasticity specifically?
Not for elasticity as a defined endpoint. Both are studied mainly in rodent wound- and tissue-repair models, where they promote angiogenesis, fibroblast activity, cell migration, and collagen deposition. These support the healing environment in which matrix is built, but no controlled study demonstrates that either peptide increases functional skin elasticity in humans. Their inclusion in KLOW rests on a regenerative rationale, not elasticity data.
What biomarkers do researchers use to measure elasticity changes?
Common readouts include collagen type I/III staining and hydroxyproline assays, qRT-PCR of COL1A1, ELN, and VCAN genes, elastin cross-link chemistry (desmosine/isodesmosine), lysyl oxidase activity, and biomechanical testing by ex vivo tensile measurement or non-invasive cutometry. Gene expression and staining are reported more often than direct biomechanics, so upstream markers should not be read as proof of functional recoil.
Why can’t KLOW’s effect be assumed from its individual components?
Because combining four peptides — one of them copper-bound — can change stability, solubility, and pharmacology in ways no study has characterized. Route and delivery also differ: GHK-Cu’s human elasticity evidence is topical cosmetic, while the regenerative components are studied by injection in animals. Synergy, interference, and copper interactions in the actual blend are unknown, so component data are suggestive, not confirmatory.
Is KLOW approved for human use?
No. KLOW and each of its component peptides (GHK-Cu, BPC-157, TB-500, KPV) are research chemicals intended for laboratory and experimental use only. None are approved by the FDA or equivalent regulators as drugs for treating skin aging or any condition. Nothing in this article is medical advice or a recommendation for human administration.
Why are there no clinical trials on the KLOW blend specifically?
The gap is structural, not accidental. KLOW is a vendor-assembled combination with no fixed, standardized composition, no INN, and no registered trial program — and a multi-peptide formulation cannot be validated from its ingredient list because combining peptides (one of them copper-bound) changes stability, solubility, and pharmacology in ways that must be measured directly. There is also no commercial or regulatory pathway pushing anyone to run such trials on an unapproved research blend, so the data simply do not exist.
Does combining four peptides make KLOW more effective than GHK-Cu alone?
That is an untested assumption. In combination pharmacology, additivity is the default and synergy has to be demonstrated — typically by isobolographic analysis comparing the blend against each component. No such study has been done for KLOW, so it is unknown whether the four peptides together are synergistic, merely additive, or even antagonistic or destabilizing for elasticity. “More ingredients” does not automatically mean “better outcome.”
How is skin elasticity measured in research?
Across three tiers. Non-invasively, a suction cutometer draws skin into a probe and derives viscoelastic parameters such as R2 (gross elasticity), R5 (net elasticity), and R7 (biological elasticity), which decline with age. At the tissue level, biopsies are analyzed by collagen and elastin staining, hydroxyproline assay, and desmosine/isodesmosine cross-link chemistry. In vitro, fibroblast cultures are profiled by qRT-PCR of COL1A1, ELN, and VCAN plus collagen protein imaging. A gene-expression rise is upstream of, and does not by itself prove, a measurable gain in functional recoil.
Does KPV do anything for skin elasticity directly?
Not directly. KPV, the C-terminal tripeptide of α-MSH, is anti-inflammatory: it inhibits NF-κB signaling and suppresses pro-inflammatory output in keratinocytes without causing pigmentation. Its elasticity relevance is protective — by lowering inflammatory and oxidative pressure it may reduce MMP-driven degradation of existing collagen and elastin — rather than generative. This is a plausible matrix-protective rationale, demonstrated for KPV alone and never within the KLOW blend.
How is a KLOW research vial typically prepared?
In research settings, blend vials are reconstituted with an appropriate sterile diluent, handled gently to avoid denaturation, protected from light and heat, and refrigerated. Because a blend vial contains several peptides, the combined mass must be accounted for when calculating concentration — researchers use a dosage calculator and the vial-specific protocol rather than estimating. See the reconstitution guide and KLOW protocol linked above for the documented conventions.
References
- Feng, M. (2018). Improving the bioavailability of collagen-derived peptides (Master’s thesis). University of Alberta. Improving the bioavailability of collagen-derived peptides
- Kim, S. H., et al. (2024). Development of a biomarker-based platform for comprehensive skin characterization using minimally invasive skin sampling and quantitative real-time PCR. Skin Research and Technology, 30(8), e13908. Biomarker-based platform for skin characterization (qRT-PCR)
- Collagen peptides affect collagen synthesis and the expression of collagen, elastin, and versican genes in cultured human dermal fibroblasts (2024). Frontiers in Medicine. Collagen peptides and COL1A1/ELN/VCAN expression in human dermal fibroblasts
- Zhang, Z., et al. (2020). The effects and mechanism of collagen peptide and elastin peptide on skin aging induced by D-galactose combined with ultraviolet radiation. Journal of Photochemistry and Photobiology B: Biology, 210, 111964. Collagen and elastin peptide on D-galactose/UV skin aging
- Pickart, L., Vasquez-Soltero, J. M., & Margolina, A. (2015). GHK peptide as a natural modulator of multiple cellular pathways in skin regeneration. BioMed Research International, 2015, 648108. GHK peptide as a natural modulator of multiple cellular pathways in skin regeneration
- Pickart, L., & Margolina, A. (2018). Regenerative and protective actions of the GHK-Cu peptide in the light of the new gene data. International Journal of Molecular Sciences, 19(7), 1987. Regenerative and protective actions of the GHK-Cu peptide in light of new gene data
- Pickart, L. (2008). The human tri-peptide GHK and tissue remodeling. Journal of Biomaterials Science, Polymer Edition, 19(8), 969–988. The human tri-peptide GHK and tissue remodeling
- From regeneration to analgesia: the role of BPC-157 in tissue repair and pain management (2026). International Journal of Molecular Sciences. The role of BPC-157 in tissue repair
- Chang, C. H., et al. Pentadecapeptide BPC 157 enhances the growth hormone receptor expression in tendon fibroblasts. Molecules. BPC 157 enhances growth hormone receptor expression in tendon fibroblasts
- Malinda KM, Sidhu GS, Mani H, et al. Thymosin β4 accelerates wound healing. Journal of Investigative Dermatology. 1999;113(3):364–368.
- Pawar, K., Kolli, C. S. R., Rangari, V. K., & Babu, R. J. (2017). Transdermal iontophoretic delivery of lysine-proline-valine (KPV) peptide across microporated human skin. Journal of Pharmaceutical Sciences, 106(7), 1814–1820. Transdermal iontophoretic delivery of KPV peptide across microporated human skin
- Pickart, L., Vasquez-Soltero, J. M., & Margolina, A. (2015). GHK-Cu may prevent oxidative stress in skin by regulating copper and modifying expression of numerous antioxidant genes. Cosmetics, 2(3), 236–247. GHK-Cu, copper regulation, and antioxidant gene expression in skin
- Immobilized α-melanocyte-stimulating hormone 10–13 (GKPV) inhibits tumor necrosis factor-α-stimulated NF-κB activity. Peptides (ScienceDirect). GKPV inhibits TNF-α-stimulated NF-κB activity
- Tallarida, R. J. (2011). Quantitative methods for assessing drug synergism (the isobole and related methods). Genes & Cancer, 2(11), 1003–1008. Revisiting the isobole and related quantitative methods for assessing drug synergism
- Correlation between skin elasticity evaluation parameters and age (2024). Cosmetics, 11(6), 205. Correlation between skin elasticity evaluation parameters (R2/R5/R7) and age