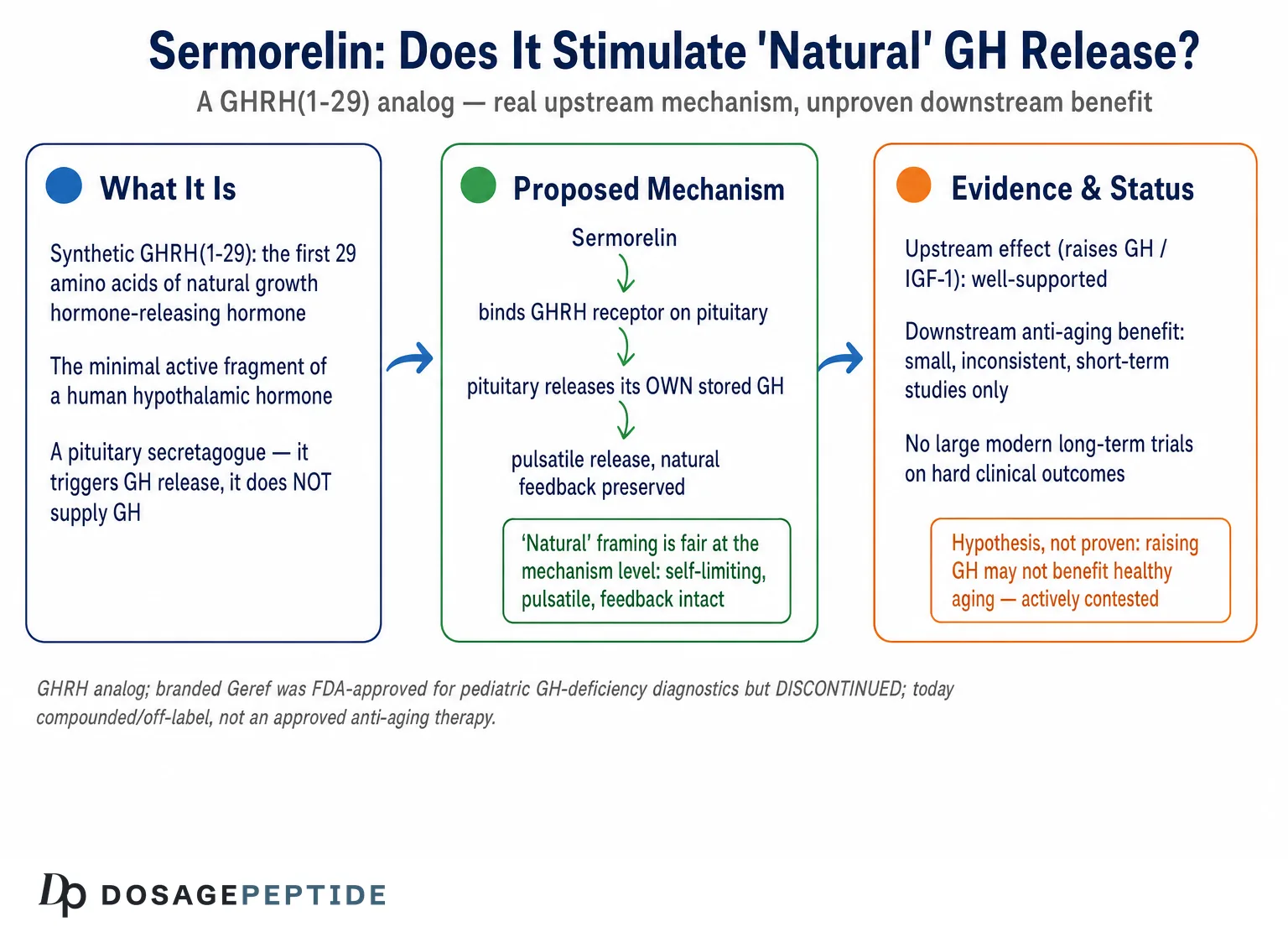
The question of whether sermorelin stimulates “natural” growth hormone deserves a more careful answer than the marketing around the compound usually gives it, because the honest answer is unusual: at the level of basic pharmacology, the premise is essentially correct, while at the level of clinical benefit it remains far softer and more contested than most sources admit. Sermorelin is a synthetic analog of growth hormone-releasing hormone (GHRH). It binds the same pituitary receptor that the body’s own GHRH activates, and in doing so it prompts the anterior pituitary to secrete growth hormone (GH) that the gland makes itself, in something close to the body’s own pulsatile rhythm.1 That is a genuine, well-characterized mechanism, not a vendor invention. So unlike many research peptides whose central claim collapses on inspection, sermorelin’s core claim — that it triggers endogenous GH release — is real.
Where honesty requires more discipline is everything downstream of that first fact. Stimulating a hormone is not the same as producing a clinical benefit, and the gap between “raises GH and IGF-1” and “improves health, body composition, or the trajectory of aging” is exactly where the sermorelin story becomes thin. The human trials that exist are small, short, decades old, and inconsistent in their functional outcomes. The one product ever approved — branded Geref — was cleared for a narrow purpose in children and for diagnostic testing, not for the anti-aging or body-optimization uses that dominate today’s conversation, and it was voluntarily discontinued in 2008.2 Everything prescribed now is compounded and off-label. This article treats the title’s question at both levels: affirming the mechanism where the data support it, and refusing to let a real pharmacodynamic effect be inflated into proven therapeutic value where the data do not.
The intended reader is a researcher or an educated layperson who wants a precise map: what sermorelin is, how it engages the pituitary, why the “natural release” framing is meaningful, what the clinical record actually shows, how it compares with recombinant GH and other secretagogues, how it has been studied and dosed, what is known about safety, and — crucially — its true regulatory status. Throughout, the guiding principle is that sermorelin’s honest position is neither “miracle” nor “fraud” but something more interesting: a real GHRH pharmacology attached to a modest and incompletely proven clinical case.
What Sermorelin Is and Where It Came From
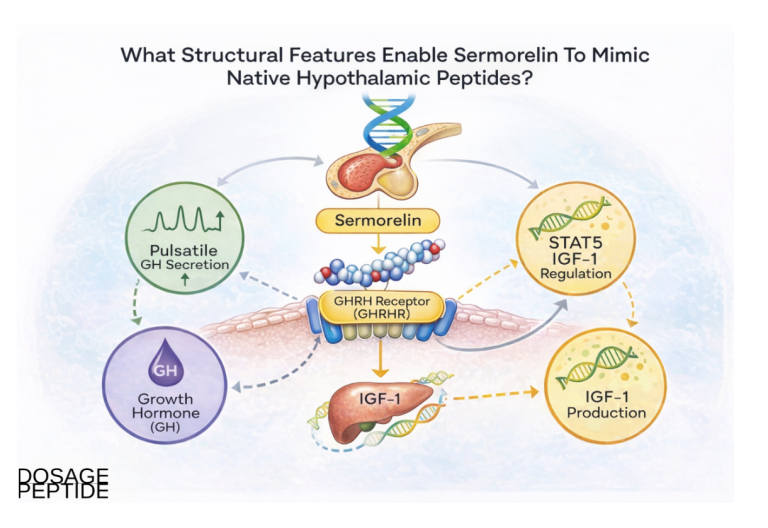
Sermorelin, also written as sermorelin acetate or GHRH(1–29), is a peptide of 29 amino acids. It corresponds to the first 29 residues of the N-terminal end of endogenous human growth hormone-releasing hormone, a 44-amino-acid hypothalamic hormone. That truncation is not arbitrary. Structure–activity work established that the biological activity of GHRH resides in its N-terminal region, and that the 1–29 fragment is the shortest sequence retaining full GH-releasing potency at the pituitary receptor.1 In other words, sermorelin is not a redesigned molecule or a foreign mimic; it is the minimal active core of a natural human hormone, reproduced synthetically.
This origin is the single most important fact for understanding why sermorelin behaves the way it does. Because it is the active fragment of GHRH itself, it does what GHRH does: it tells the somatotroph cells of the anterior pituitary to release stored growth hormone. It does not supply growth hormone from outside the body, and it does not act on peripheral tissues to build muscle or burn fat directly. Its entire action is upstream, at the level of the pituitary gland.
The compound has a formal pharmaceutical history that is often blurred in popular accounts. It was developed and studied through the 1980s and 1990s, first as a diagnostic agent to probe the pituitary’s capacity to secrete GH, and later as a treatment for children with idiopathic growth hormone deficiency whose deficiency was hypothalamic rather than pituitary in origin.1 Under the brand name Geref, it received U.S. Food and Drug Administration approval — the diagnostic indication first, and a treatment indication for pediatric growth failure in the late 1990s.2 That regulatory pedigree is real, and it is why sermorelin is sometimes described, accurately, as a “formerly FDA-approved” peptide. What matters is the fine print: the approval covered children with a specific deficiency and a diagnostic use, not healthy adults seeking anti-aging effects, and the branded product was withdrawn from the market in 2008 for commercial reasons as recombinant human growth hormone came to dominate pediatric practice.11
It helps to hold three distinct entities apart when thinking about sermorelin, because conflating them produces most of the confusion in circulation. First, there is endogenous GHRH, the natural 44-residue hypothalamic hormone that governs GH secretion. Second, there is sermorelin, the synthetic 1–29 fragment that reproduces GHRH’s activity and has a short circulating half-life measured in minutes. Third, there is recombinant human growth hormone (rhGH), the downstream hormone itself, administered directly and bypassing the pituitary entirely. Sermorelin sits one step upstream of GH: it is a secretagogue, an agent that causes secretion, rather than a replacement of the secreted product. Many claims made about sermorelin are really claims about GH that have been transplanted onto its upstream trigger, and keeping the three entities separate is the best defense against that slippage. For readers surveying the broader landscape of growth-hormone-axis research compounds, the site’s dosage index catalogs how these upstream secretagogues are distinguished from direct hormone replacement.
The Mechanism: How Sermorelin Reaches the Pituitary
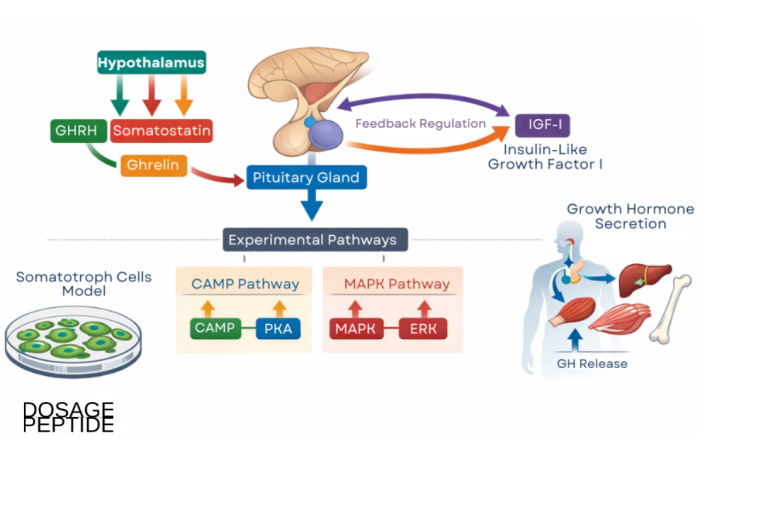
The mechanism of sermorelin is one of the better-defined stories in the peptide field, precisely because it borrows directly from the physiology of a natural hormone. Sermorelin binds the growth hormone-releasing hormone receptor (GHRH-R), a G-protein-coupled receptor expressed predominantly on the somatotroph cells of the anterior pituitary.3 The GHRH-R is a class B (secretin-family) GPCR, and its engagement sets off a well-mapped intracellular cascade.
Upon binding, the receptor couples to the stimulatory G protein (Gs), which activates adenylyl cyclase, raising intracellular cyclic AMP (cAMP). The rise in cAMP activates protein kinase A and, through downstream signaling that includes mitogen-activated protein kinase (MAPK) pathways, produces two effects: an acute release of stored growth hormone from secretory granules, and a slower, trophic stimulation of GH gene transcription and somatotroph proliferation.3 The acute effect is what produces the pulse of GH seen within minutes of administration; the trophic effect is part of why chronic GHRH exposure can, in principle, maintain or expand the pituitary’s secretory capacity rather than exhaust it.
Two features of this cascade deserve emphasis because they distinguish sermorelin from simply injecting growth hormone. The first is pulsatility. Endogenous GH is not secreted as a steady stream; it is released in discrete bursts, predominantly at night during slow-wave sleep, with near-undetectable levels between pulses. This pulsatile pattern is thought to be physiologically important — different tissues respond differently to pulsatile versus continuous GH exposure. Because sermorelin works by prompting the pituitary to fire its own pulses, the resulting GH release tends to follow the body’s natural rhythmic pattern rather than the flat, sustained elevation produced by exogenous rhGH injection.3 The second feature is preserved negative feedback. GH secretion is restrained by somatostatin (the hypothalamic “off” signal) and by the negative feedback of GH and IGF-1 on the hypothalamus and pituitary. Sermorelin acts within this intact regulatory loop: if GH and IGF-1 rise too high, the body’s own somatostatin tone and feedback braking limit further release. This ceiling is a genuine mechanistic safeguard that direct rhGH administration lacks, and it is the strongest pharmacological argument for the “natural” framing in the article’s title.4
A further mechanistic subtlety is worth naming, because it bears on why the “natural” description holds up under scrutiny rather than being mere branding. The GHRH signal and the opposing somatostatin signal together sculpt the shape of each GH pulse: GHRH sets the amplitude, while withdrawal of somatostatin tone permits the pulse to fire. Sermorelin adds to the GHRH arm of that balance without touching the somatostatin arm, so the pituitary still cannot release GH during periods of high somatostatin tone no matter how much sermorelin is present. This is why the compound produces discrete, well-formed pulses rather than a continuous leak of hormone, and why its effect is naturally entrained to the times — chiefly deep sleep — when somatostatin tone falls. The trophic, longer-term arm of the cascade matters too: sustained GHRH-receptor signaling supports somatotroph health and gene transcription, which is the mechanistic reason a secretagogue approach is sometimes argued to be more sustainable than repeatedly overriding the system with exogenous hormone.3 These are elegant properties, but they should be read as reasons the mechanism is plausible and physiological, not as independent proof of clinical benefit.
There is, however, a corollary that honesty demands: because sermorelin depends on a functioning pituitary and an intact feedback system, it can only work if the somatotrophs are capable of responding. In a person whose pituitary cannot make GH — for example, after surgical removal or radiation damage to the gland — sermorelin has nothing to stimulate and will fail. This is not a defect but a defining limitation: sermorelin amplifies an existing capacity; it does not create one. That same dependence is what made sermorelin useful as a diagnostic agent (it tests whether the pituitary can respond to GHRH), and it explains why its effects in aging are inherently bounded by whatever secretory reserve remains. Readers exploring how upstream stimulation is thought to influence downstream physiology may find the discussion in the site’s coverage of whether sermorelin supports cognitive function in age-related neurodegeneration a useful companion, as it examines the same GH/IGF-1 axis from a different endpoint.
Why “Natural” Growth Hormone Release Is the Central Claim
The word “natural” in the title is doing real work, and it is worth unpacking rather than dismissing, because it is the axis on which sermorelin’s legitimate appeal turns. The contrast is with exogenous recombinant growth hormone, and the differences are not cosmetic.
When rhGH is injected, it delivers a bolus of hormone that circulates and acts on tissues regardless of what the body would have chosen to do at that moment. Serum GH rises, IGF-1 rises, and the pituitary’s own secretion is suppressed by feedback. The pattern is non-physiological: a sustained elevation rather than a pulse, imposed from outside the regulatory system. Over time and at supraphysiological doses, this pattern is associated with the recognizable adverse effects of GH excess — fluid retention, joint pain, carpal tunnel syndrome, insulin resistance, and, at the extreme, the features of acromegaly.4
Sermorelin works differently. It asks the pituitary to release its own GH in its own rhythm, subject to the body’s own brakes. In practical terms this predicts a lower ceiling on GH exposure, a preserved circadian and pulsatile pattern, and a reduced likelihood of driving IGF-1 into supraphysiological territory. This is the mechanistic basis for the frequently repeated claim that sermorelin offers a “more physiological” approach than direct GH replacement.4 The claim is reasonable as a description of mechanism.
But two honest caveats must travel alongside it. First, “more physiological” is a statement about the shape of the hormonal signal, not a demonstration of superior clinical outcomes; the two do not automatically follow from each other, and no large head-to-head trial has shown that sermorelin produces better long-term results than any comparator in adults. Second, the very feature that makes sermorelin gentler — its dependence on the pituitary and on intact feedback — also caps its potential magnitude of effect. It cannot push GH and IGF-1 as high as rhGH can, which is desirable from a safety standpoint but limiting from an efficacy standpoint. The “natural” framing, then, is best understood as a trade: a smoother, self-limiting, more physiological signal in exchange for a smaller and more variable effect that depends on the individual’s own secretory reserve. That trade is genuinely attractive in principle. Whether it delivers meaningful benefit in practice is the empirical question the rest of this article examines.
The Diagnostic Legacy and the Pediatric Evidence
The strongest and most rigorous evidence for sermorelin’s core action does not come from anti-aging clinics; it comes from its original clinical roles, and it is worth taking seriously because it is where the compound was studied under regulatory scrutiny.
As a diagnostic agent, sermorelin was used to test pituitary responsiveness. Administered intravenously or subcutaneously, it provokes a measurable GH rise in people with an intact, responsive pituitary; a blunted response points toward pituitary (rather than hypothalamic) disease. This diagnostic use rests directly on the mechanism described above, and its reliability in provoking GH release is the clearest possible demonstration that sermorelin does what it claims: it stimulates endogenous GH secretion.1
As a therapeutic agent, sermorelin was approved for children with idiopathic growth hormone deficiency — specifically the subset whose deficiency arose from inadequate hypothalamic GHRH signaling rather than from an intrinsically failed pituitary. In these children, supplying the missing GHRH signal with daily subcutaneous sermorelin increased GH secretion and improved growth velocity.1 The review literature of the era characterized sermorelin as producing meaningful height-velocity gains in appropriately selected responders, with effect sizes generally smaller than those achieved by direct rhGH therapy but with a favorable tolerability profile.1 This is an important and honest nuance: even in its approved pediatric indication, sermorelin was understood to be somewhat less potent than direct hormone replacement, precisely because it depends on the child’s own pituitary capacity.
The pediatric and diagnostic evidence establishes two things cleanly. First, sermorelin genuinely and reproducibly stimulates natural GH release — this is not in serious scientific dispute. Second, the magnitude of downstream benefit is bounded by the responsiveness of the individual’s pituitary and tends to be more modest than direct GH. Both facts carry directly into the adult and aging context, where the pituitary’s secretory reserve is diminished and where, as we will see, the clinical evidence becomes much thinner. For a grounding in the vocabulary of this axis — somatotroph, secretagogue, IGF-1, pulsatility — the site’s peptide glossary defines the terms used throughout this discussion.
What the Human Trials Show in Aging Adults
This is the section where restraint matters most, because the adult anti-aging use of sermorelin is both the most popular and the least well-evidenced. The honest summary is that a handful of small, short studies from the 1990s consistently show that sermorelin (and closely related GHRH(1–29) analogs) raises GH and IGF-1 in older adults, but that the translation of those hormonal changes into body-composition and functional benefits is inconsistent, modest, and sex-dependent. There are no large, modern, long-term randomized trials establishing meaningful clinical outcomes.
The foundational study is Corpas and colleagues at the National Institute on Aging, who showed in 1992 that GHRH(1–29) given twice daily for two weeks reversed the age-related decline in GH and IGF-1 in older men, restoring hormone levels toward those seen in younger men.5 This established the pharmacodynamic point in the aging population: the older pituitary retains enough reserve to respond. Crucially, however, this short study was about hormone levels, not clinical endpoints, and later analyses in the same research program noted that raising GH and IGF-1 did not automatically translate into changes in body weight, lean mass, or fat mass over the intervals studied.5
Vittone and colleagues, in 1997, gave single nightly subcutaneous injections of GHRH(1–29) to healthy elderly men for six weeks. Nocturnal GH output roughly doubled — a clear demonstration of the compound’s effect on the pattern of secretion — but over the short treatment period IGF-1 did not rise significantly, and functional endpoints were not the focus.6 The lesson is that a robust effect on GH pulses does not guarantee a proportional change in the integrated IGF-1 signal that mediates many of GH’s peripheral effects.
The most cited body-composition study is Khorram, Laughlin, and Yen’s 1997 trial of a GHRH(1–29) analog given nightly for 16 weeks (following a 4-week placebo run-in) to men and women aged 55 to 71.7 Nocturnal GH rose by roughly 100 percent and IGF-1 by roughly a quarter within the first weeks. In terms of clinical measures, men gained a modest amount of lean body mass (on the order of 1.26 kg on average) and reported improvements in well-being and libido, insulin sensitivity improved, and skin thickness increased in both sexes. But — and this is the caveat routinely omitted from marketing — women did not gain lean body mass, illustrating a sex-dependent and inconsistent functional response even in the single most favorable trial.7 A gain of roughly one kilogram of lean mass in men over four months, with no lean-mass benefit in women, is a real but small signal, and it is a slender foundation for the sweeping claims often made.
| Study | Population & duration | Hormonal effect | Functional / body-composition effect |
|---|---|---|---|
| Corpas et al. 19925 | Older men; GHRH(1–29) twice daily, ~2 weeks | GH and IGF-1 restored toward younger-adult levels | Short duration; no established change in body composition |
| Vittone et al. 19976 | Healthy elderly men; single nightly injection, 6 weeks | Nocturnal GH roughly doubled; IGF-1 not significantly increased | Not a primary focus; no clear functional benefit shown |
| Khorram et al. 19977 | Men & women 55–71; nightly analog, 16 weeks | Nocturnal GH ~+100%; IGF-1 ~+28% | Men +~1.26 kg lean mass; women no lean-mass gain; skin thickness up in both; improved insulin sensitivity, well-being |
Read together, these studies support a careful two-part conclusion. The upstream claim is well-supported: sermorelin-type GHRH analogs reliably raise GH secretion and usually IGF-1 in older adults, confirming that the “stimulates natural growth hormone” premise is biologically real even in aging. The downstream claim is weak: the resulting changes in body composition and function are small, inconsistent, sex-dependent, measured over weeks to a few months, and never confirmed in large modern trials with hard clinical endpoints such as fracture reduction, cardiovascular outcomes, or longevity. Anyone extrapolating from “raises IGF-1 by a quarter over 16 weeks” to “reverses aging” is leaping across an evidentiary chasm. The site’s research blog tracks how this literature evolves as newer work appears, but as of this writing the modern evidence base for adult anti-aging use remains thin.
Sermorelin Compared With rhGH and Other Secretagogues
Sermorelin is one member of a broader family of ways to raise growth-hormone signaling, and placing it in that family clarifies both its appeal and its limits. The relevant comparators are direct recombinant GH, other GHRH analogs (notably tesamorelin and the long-acting CJC-1295), and the ghrelin-mimetic GH secretagogues (such as ipamorelin, GHRP-2, GHRP-6, and the orally active ibutamoren/MK-677), which act on a different receptor to release GH.4
| Approach | How it raises GH signaling | Pattern of GH exposure | Regulatory / evidence status |
|---|---|---|---|
| Recombinant human GH (rhGH) | Supplies GH directly; bypasses the pituitary | Sustained, non-pulsatile; feedback bypassed | FDA-approved for defined GH-deficiency and other specific indications; potent but with dose-related GH-excess effects4 |
| Sermorelin (GHRH 1–29) | Stimulates the pituitary via GHRH-R | Pulsatile, physiological; feedback preserved; short half-life | Branded Geref formerly FDA-approved (pediatric GHD, diagnostic), discontinued 2008; now compounded/off-label2 |
| Tesamorelin (GHRH analog) | Stabilized GHRH analog at the same receptor | Pulsatile, physiological | FDA-approved specifically for HIV-associated lipodystrophy; not an anti-aging approval4 |
| CJC-1295 (long-acting GHRH analog) | GHRH-R agonist engineered for a longer half-life | More sustained elevation of GH/IGF-1 | Not approved for any therapeutic use; research compound4 |
| Ghrelin-mimetic secretagogues (ipamorelin, GHRP-2/6, MK-677) | Act on the ghrelin/GHS receptor, a separate pathway | Pulsatile GH release; some also raise appetite | Investigational for most uses; not approved anti-aging therapies4 |
Several honest observations emerge from this comparison. First, sermorelin’s distinctive selling point — a physiological, self-limiting, pulsatile GH signal — is shared to varying degrees by the other GHRH analogs and even by the ghrelin-mimetic secretagogues; it is not unique to sermorelin. Second, within the GHRH class, sermorelin is the shortest-acting: its half-life is only minutes, which is why nightly dosing timed to sleep is the studied pattern, and why longer-acting analogs like CJC-1295 were engineered in the first place.4 Third, and most important for calibrating expectations, only two members of this landscape carry current FDA approval for any indication — rhGH (for defined deficiency states) and tesamorelin (for HIV-associated lipodystrophy specifically) — and neither approval is for anti-aging or healthy-adult optimization. Sermorelin’s own former approval was narrow and has lapsed. The comparison thus reframes the popular question: the interesting distinctions among these agents are real at the level of pharmacokinetics and receptor target, but none of them has an approved anti-aging indication, and sermorelin’s evidence for adult benefit is not stronger than, and in some respects thinner than, that of its better-studied cousins.
It is also worth noting why sermorelin is frequently paired in research framings with a ghrelin-mimetic such as ipamorelin. The two act on different receptors — GHRH-R and the GHS receptor — and in principle their signals can be additive or synergistic at the somatotroph, producing a larger GH pulse than either alone. This combination logic is mechanistically coherent, but it is important to be clear that the existence of a plausible synergy is not the same as controlled evidence of superior clinical outcomes in humans, which does not exist for the pairing in an anti-aging context.4
Dosing and Administration in a Research Context
Any discussion of sermorelin dosing must begin with an unambiguous framing: there is no current FDA-approved sermorelin product, no approved adult indication, and therefore no officially sanctioned adult dosing regimen. What follows is a strictly educational description of how the compound has been administered in the published literature and how research protocols are typically structured — not a recommendation for use.
In the pediatric approval era, sermorelin was given by daily subcutaneous injection, and diagnostic testing used weight-based intravenous or subcutaneous dosing to provoke a measurable GH response.1 In the adult aging studies, the pattern that recurs is a single subcutaneous injection given at night, timed to coincide with and amplify the natural nocturnal GH pulse associated with slow-wave sleep. The Khorram trial, for instance, used a weight-based nightly dose (on the order of 10 µg/kg) administered before sleep.7 This timing is not incidental: because sermorelin works by amplifying the pituitary’s own rhythm, aligning administration with the body’s largest natural GH pulse is the logical way to maximize a physiological signal.
Two features of sermorelin’s pharmacology shape how it is studied. First, the very short half-life means the compound produces a discrete pulse rather than a sustained elevation, which is consistent with the “natural release” rationale but also means timing and consistency matter more than with a long-acting agent. Second, food — particularly a high-fat or high-carbohydrate meal near the time of injection — can blunt GH release, so research protocols generally separate administration from meals. The endpoints used to gauge response in a research setting are hormonal (nocturnal GH output, integrated 24-hour GH, and serum IGF-1) and, in the more ambitious studies, body composition by DXA and measures of physical function.
Because sermorelin is supplied as a lyophilized (freeze-dried) powder that must be reconstituted, the arithmetic of reconstitution is part of any rigorous research handling. The general principle is that a fixed mass of peptide dissolved in a chosen volume of diluent sets the concentration, and the injected volume then determines the delivered dose. Educational walkthroughs of that arithmetic — how vial size, diluent volume, and syringe graduations interact — are laid out on the site’s peptide reconstitution guide, and the underlying calculations can be worked through with the dosage calculator. These are presented as research-context references, not as instructions for human use.
The honest bottom line on dosing is that the regimens appearing in the literature were designed to answer hormonal questions in small studies, not to establish a validated therapeutic dose for healthy adults. Extrapolating a precise “optimal” anti-aging dose from these sources overstates what the data can support; the studies were not powered or designed for that purpose.
Safety and Tolerability
Sermorelin’s safety profile is, within the limits of the available data, one of its more reassuring features — a point that must nonetheless be stated with the same caveats that qualify its efficacy. Because sermorelin works within the body’s intact feedback system, it is inherently less able to drive growth-hormone signaling into the pathological excess that direct rhGH can produce, and the clinical record reflects a generally favorable tolerability profile at studied doses.1
The most common adverse effects reported across studies are local: transient redness, swelling, or discomfort at the subcutaneous injection site. Systemic effects that have been reported less frequently include flushing, headache, dizziness, a sensation of warmth, and occasional nausea or an altered taste. Because the intended effect is a rise in GH and IGF-1, the theoretical adverse effects of GH excess — fluid retention, joint aches, carpal-tunnel-type symptoms, and reduced insulin sensitivity — are relevant, but the feedback-limited mechanism makes them less likely at physiological dosing than with supraphysiological rhGH.4 A theoretical concern common to all GH-axis interventions is that sustained elevation of GH/IGF-1 signaling could, in principle, be undesirable in the context of active or latent malignancy, since IGF-1 is a growth factor; this is a reason for caution rather than a demonstrated harm from sermorelin specifically, and it has not been characterized in long-term human trials of the compound.
Several honest limitations bound this reassuring picture:
- Short duration of evidence. The adult studies ran for weeks to a few months. The long-term safety of chronic sermorelin administration in healthy adults over years has not been established in controlled trials.
- Small and selected populations. The trials enrolled modest numbers of relatively healthy participants; safety in people with comorbidities, on multiple medications, or at the extremes of age is far less characterized.
- Contraindication by mechanism. Sermorelin is not appropriate where GH stimulation is undesirable — for example, in active malignancy — and is ineffective where the pituitary cannot respond.
- Product quality outside regulated channels. Because there is no approved finished product, material obtained outside of legitimate compounding pharmacies varies in purity and sterility. Impurities, endotoxin, and mislabeling are real risks that are independent of the molecule’s intrinsic safety and entirely a function of sourcing.
- Prohibited in sport. Sermorelin, as a GHRH analog, is on the World Anti-Doping Agency Prohibited List under the peptide-hormone category; for tested athletes its use is an anti-doping rule violation regardless of pharmacology.8
The reasonable reading is that sermorelin has not generated major short-term safety signals in the limited populations studied, and that its feedback-preserving mechanism is a genuine safety advantage over direct GH. But an encouraging short-term profile in small studies is not evidence of long-term safety in chronic anti-aging use, and the absence of demonstrated harm should not be mistaken for a demonstration that indefinite use is safe.
The Somatopause Question: Does Raising GH Help Aging?
Behind the popularity of sermorelin lies a larger and genuinely unsettled scientific question, and engaging it honestly is essential to answering the title. Growth hormone secretion declines with age — a phenomenon often called the “somatopause” — and this decline is real and well-documented: integrated GH output and IGF-1 levels fall progressively from young adulthood onward, on the order of roughly 15 percent per decade after the third decade of life.9 The intuitive therapeutic logic is straightforward: if GH falls with age and GH does desirable things (supports lean mass, bone, skin), then restoring youthful GH levels should reverse or slow aspects of aging. Sermorelin, by stimulating the aging pituitary, is positioned as a physiological way to do exactly that.
The problem is that the intuitive logic runs ahead of the evidence, and in some respects the evidence points in a more complicated direction. Decades of research into GH and aging have failed to establish that raising GH/IGF-1 in older adults produces durable, clinically meaningful benefit on the outcomes that matter — strength, function, independence, morbidity, and mortality — and there is a competing body of biology suggesting that lower GH/IGF-1 signaling is associated with longevity in numerous model systems and in some human populations.9 In other words, the decline in GH with age may not be simply a deficiency to be corrected; it may in part be an adaptive or even protective change. This is an active, unresolved debate, not a settled matter, and it is the single most important piece of context that the marketing around sermorelin omits.
Reviews of growth hormone in aging repeatedly reach a cautious conclusion: GH-axis interventions can change body composition modestly (a small increase in lean mass, a small decrease in fat mass) but frequently fail to improve the functional endpoints — muscle strength, physical performance — that would make those compositional changes clinically worthwhile, and they carry a real burden of side effects when pushed toward supraphysiological exposure.910 Sermorelin’s gentler, feedback-limited mechanism plausibly mitigates the side-effect burden, but by the same token it produces smaller compositional changes, and it has not been shown to escape the central disappointment of the field: that moving the biomarker does not reliably move the outcome.
It is also worth being explicit about why the aging-adult evidence is so much weaker than one might expect for a compound this old. The influential trials were run in the 1990s, before the field standardized on the functional and patient-centered endpoints that regulators now require, and they enrolled small numbers over short intervals. No sponsor has since mounted a large, adequately powered, long-duration randomized trial of sermorelin in healthy older adults — in part because, once the branded product was discontinued in 2008 and the compound moved into the compounding and off-label space, the commercial incentive to fund expensive pivotal trials largely evaporated.2 The result is a peculiar situation in which a genuinely well-understood mechanism is attached to a clinical literature that is thin not because the compound failed rigorous testing, but because that testing was never done at scale. That absence of evidence is not evidence of absence of benefit — but neither can it be read as evidence of benefit, and the burden of proof for an anti-aging claim has simply not been met.
So the honest answer to “does stimulating natural GH help aging?” is: stimulating GH is achievable and real, but whether doing so benefits an aging person is not established and is genuinely contested. Sermorelin sits squarely inside this uncertainty. It is a well-mechanized way to nudge a declining system back toward its younger set-point, wrapped around a therapeutic premise — that the nudge is beneficial — that the broader science has not confirmed and in some respects questions. A researcher should hold both halves of that sentence at once.
Regulatory Status: Precise and Frequently Misrepresented
Sermorelin’s regulatory status is the area where marketing most often blurs the truth, so precision is worth the space.
Formerly approved, now discontinued. Sermorelin acetate, as the branded product Geref, did receive FDA approval — a diagnostic indication and, subsequently, a treatment indication for pediatric idiopathic growth hormone deficiency.2 This is genuine regulatory history and distinguishes sermorelin from research peptides that were never approved for anything. However, the sole manufacturer voluntarily ceased production, and the branded product was withdrawn from the U.S. market in 2008 — for commercial reasons, as recombinant human growth hormone came to dominate the pediatric growth-hormone-deficiency market, rather than for safety reasons. The FDA later formally determined that Geref was not withdrawn for reasons of safety or effectiveness, confirming the commercial nature of the decision.11 The practical consequence is that, as of today, there is no FDA-approved finished sermorelin drug product on the market.
Everything current is compounded and off-label. Sermorelin prescribed in 2026 is supplied by compounding pharmacies operating under Sections 503A and 503B of the Federal Food, Drug, and Cosmetic Act. Compounded sermorelin does not carry FDA approval as a finished drug product; it is prepared for individual patients on the basis of a prescription. Its use in adults for anti-aging, body-composition, sleep, or wellness purposes is off-label and is not supported by an FDA-approved indication.2 It is essential to understand that “available through compounding pharmacies” is not equivalent to “FDA-approved,” and that the former FDA approval of Geref for children does not extend to, or validate, current adult uses.
Prohibited in sport. Sermorelin is included on the WADA Prohibited List within the category covering peptide hormones and growth factors — specifically as a growth-hormone-releasing factor, the same class that encompasses tesamorelin, CJC-1295, and related GHRH analogs.8 Athletes subject to anti-doping testing should treat sermorelin as prohibited at all times.
A recurring source of public confusion deserves explicit correction: the phrase “FDA-approved” is applied to sermorelin in ways that are technically defensible but practically misleading. Yes, a sermorelin product was once FDA-approved — for a narrow pediatric indication and diagnostics, and that product no longer exists on the market. No, sermorelin is not FDA-approved today for the adult anti-aging and optimization uses for which it is overwhelmingly prescribed. Conflating “was approved for children’s growth disorders in the 1990s” with “is an approved anti-aging therapy now” is one of the most common errors in the popular literature, and it is precisely the kind of overstatement this article exists to resist. The accurate one-sentence summary is that sermorelin is a formerly approved GHRH analog whose branded product was discontinued in 2008, now available only as a compounded, off-label preparation with no current FDA-approved indication for adults.
Frequently Asked Questions
Does sermorelin actually stimulate natural growth hormone?
Yes — this part of the claim is genuinely well-supported. Sermorelin is the active 1–29 fragment of GHRH and binds the pituitary GHRH receptor, prompting the somatotroph cells to release the body’s own stored growth hormone in a pulsatile pattern, subject to normal feedback.13 Its reliability in provoking GH release is well established, which is why it was historically used as a diagnostic agent to test pituitary function. What is far less certain is whether that GH stimulation produces meaningful clinical benefit in healthy adults, which is a separate question with much weaker evidence.
Is sermorelin FDA-approved?
Not currently, in any practical sense. The branded product Geref was FDA-approved for diagnostic use and for treating growth hormone deficiency in children, but the manufacturer discontinued it in 2008 for commercial reasons.2 There is no FDA-approved sermorelin product on the market today, and the adult anti-aging uses for which it is now prescribed are off-label preparations from compounding pharmacies, not FDA-approved therapies.
How is sermorelin different from injecting growth hormone?
Sermorelin acts one step upstream. Recombinant human GH supplies the hormone directly, producing a sustained, non-pulsatile elevation that bypasses the body’s regulatory system. Sermorelin instead prompts the pituitary to release its own GH in its natural pulsatile rhythm, with somatostatin feedback still able to limit excess.4 This makes sermorelin more physiological and, in theory, safer from GH-excess effects, but also inherently less potent, since its effect is capped by the individual’s own pituitary reserve.
What does the research show about sermorelin for anti-aging?
The evidence is thin and modest. Small studies from the 1990s show that GHRH(1–29) analogs raise GH and IGF-1 in older adults, and one 16-week trial found men gained about 1.26 kg of lean mass with improved skin thickness — but women in the same trial gained no lean mass, and the effects overall were small and short-term.567 There are no large, modern, long-term trials showing benefit on hard clinical outcomes, and the broader question of whether raising GH helps aging remains scientifically contested.
Will sermorelin work in everyone?
No. Because sermorelin works by stimulating the pituitary, it requires a functioning, responsive pituitary gland. In people whose pituitary cannot make GH — after surgery, radiation, or certain diseases — sermorelin has nothing to stimulate and will not work. Its magnitude of effect is also bounded by the individual’s remaining secretory reserve, which declines with age.1
Is sermorelin safe?
In the short-term studies available, sermorelin was generally well tolerated, with mostly local injection-site reactions and occasional flushing, headache, or nausea, and its feedback-limited mechanism reduces the risk of the growth-hormone-excess effects seen with direct rhGH.14 However, long-term safety in healthy adults using it chronically has not been established, it is inappropriate where GH stimulation is undesirable (such as active malignancy), and material from unregulated sources carries purity and sterility risks. It is also prohibited in competitive sport.8
Why is sermorelin banned in sports?
Because it raises endogenous growth hormone, sermorelin falls under the World Anti-Doping Agency’s prohibited category of peptide hormones and growth factors, specifically as a growth-hormone-releasing factor alongside tesamorelin and CJC-1295.8 For any athlete subject to anti-doping testing, its use constitutes a rule violation at all times.
Does sermorelin build muscle or burn fat directly?
No. Sermorelin has no direct action on muscle or fat tissue. Any effect on body composition is indirect, mediated through the GH and IGF-1 it stimulates the pituitary to release, and the observed effects in trials are modest and inconsistent — a small lean-mass gain in men in one study, none in women.7 It is a pituitary secretagogue, not a peripheral anabolic or lipolytic agent.
How does sermorelin compare with other GHRH peptides like tesamorelin or CJC-1295?
All three are GHRH-receptor agonists that produce a physiological, pulsatile GH signal, but they differ in pharmacokinetics and regulatory standing. Sermorelin is the shortest-acting (half-life of minutes), tesamorelin is a stabilized analog that is FDA-approved specifically for HIV-associated lipodystrophy (not anti-aging), and CJC-1295 is engineered for a longer half-life but is not approved for any therapeutic use.4 None carries an approved anti-aging indication.
References
- Prakash A, Goa KL. Sermorelin: a review of its use in the diagnosis and treatment of children with idiopathic growth hormone deficiency. BioDrugs. 1999;12(2):139-157. PMID 18031173. https://pubmed.ncbi.nlm.nih.gov/18031173/
- Walker RF. Sermorelin: a better approach to management of adult-onset growth hormone insufficiency? Clin Interv Aging. 2006;1(4):307-308. PMID 18046908. PMCID PMC2699646. https://pmc.ncbi.nlm.nih.gov/articles/PMC2699646/
- Halmos G, Szabo Z, Dobos N, Juhasz E, Schally AV. Growth hormone-releasing hormone receptor (GHRH-R) and its signaling. Rev Endocr Metab Disord. 2025;26(3):343-352. doi:10.1007/s11154-025-09952-x. PMCID PMC12137518. https://pmc.ncbi.nlm.nih.gov/articles/PMC12137518/
- Ishida J, Saitoh M, Ebner N, et al. Growth hormone secretagogues: history, mechanism of action, and clinical development. JCSM Rapid Communications. 2020;3(1):25-37. doi:10.1002/rco2.9. https://onlinelibrary.wiley.com/doi/full/10.1002/rco2.9
- Corpas E, Harman SM, Piñeyro MA, Roberson R, Blackman MR. Growth hormone (GH)-releasing hormone-(1-29) twice daily reverses the decreased GH and insulin-like growth factor-I levels in old men. J Clin Endocrinol Metab. 1992;75(2):530-535. PMID 1379256. https://pubmed.ncbi.nlm.nih.gov/1379256/
- Vittone J, Blackman MR, Busby-Whitehead J, et al. Effects of single nightly injections of growth hormone-releasing hormone (GHRH 1-29) in healthy elderly men. Metabolism. 1997;46(1):89-96. PMID 9005976. https://pubmed.ncbi.nlm.nih.gov/9005976/
- Khorram O, Laughlin GA, Yen SS. Endocrine and metabolic effects of long-term administration of [Nle27]growth hormone-releasing hormone-(1-29)-NH2 in age-advanced men and women. J Clin Endocrinol Metab. 1997;82(5):1472-1479. PMID 9141536. https://pubmed.ncbi.nlm.nih.gov/9141536/
- World Anti-Doping Agency. S2. Peptide Hormones, Growth Factors, Related Substances and Mimetics — The Prohibited List (growth hormone-releasing factors, including GHRH analogs). https://www.wada-ama.org/en/prohibited-list
- Fredrick JR, Blackman MR, Corpas E, Merriam GR, Kargi AY, Garcia JM. Growth Hormone and Aging. In: Endotext. MDText.com; NCBI Bookshelf NBK279163. https://www.ncbi.nlm.nih.gov/books/NBK279163/
- Fernández-Garza LE, Guillen-Silva F, Sotelo-Ibarra MA, Domínguez-Mendoza AE, Barrera-Barrera SA, Barrera-Saldaña HA. Growth hormone and aging: a clinical review. Frontiers in Aging. 2025;6:1549453. doi:10.3389/fragi.2025.1549453. https://www.frontiersin.org/journals/aging/articles/10.3389/fragi.2025.1549453/full
- Food and Drug Administration. Determination That GEREF (Sermorelin Acetate) Injection… Were Not Withdrawn From Sale for Reasons of Safety or Effectiveness. Federal Register. March 4, 2013 (documenting EMD Serono’s December 2008 discontinuation of GEREF). https://www.federalregister.gov/documents/2013/03/04/2013-04827/
Educational and research-use disclaimer: This article is provided solely for scientific and educational purposes. Sermorelin genuinely stimulates endogenous growth hormone secretion, but it is not currently approved by the FDA as a finished drug product; the branded product (Geref) was approved only for pediatric growth hormone deficiency and diagnostic use and was discontinued in 2008. Sermorelin is not FDA-approved for anti-aging, body-composition, or wellness use in adults, and it is available today only as a compounded, off-label preparation. No large, long-term human trials have established clinical anti-aging benefit, and sermorelin is prohibited in sport by WADA. Nothing here is medical advice or a recommendation for human use. Any legitimate investigation of this compound should occur under appropriate medical or research oversight. Readers should consult qualified professionals and applicable regulations before making any decisions.