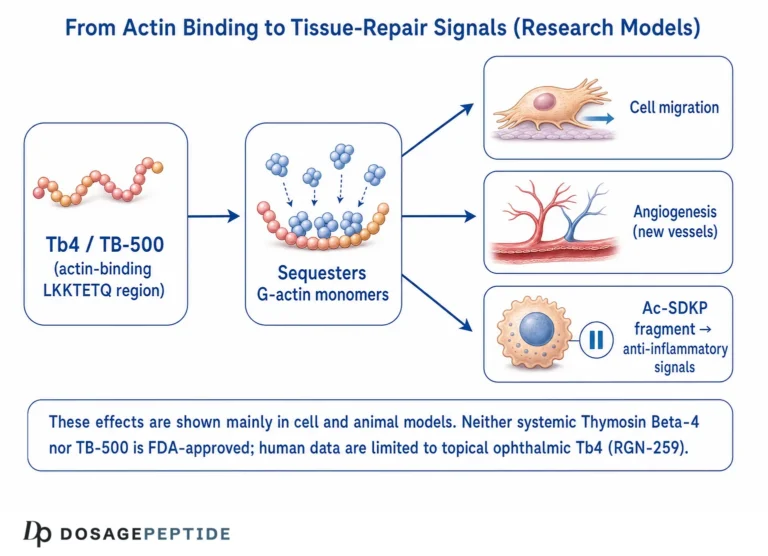
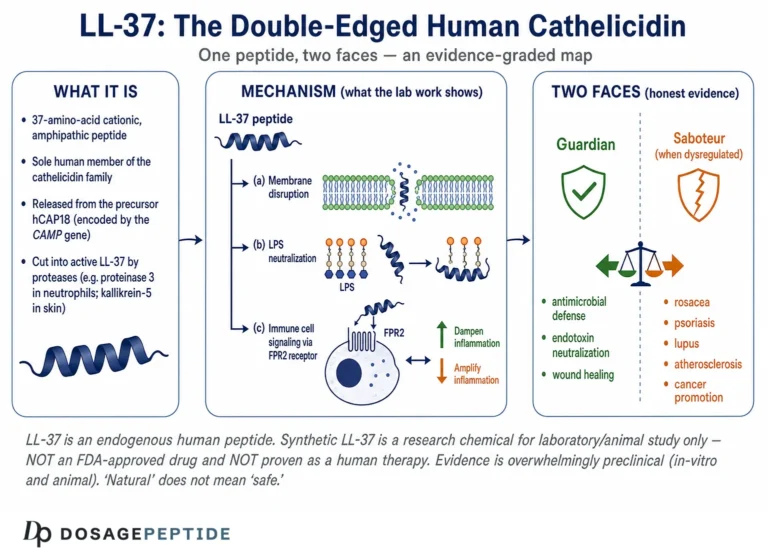
KPV is a naturally occurring tripeptide — lysine–proline–valine (Lys-Pro-Val) — that corresponds to the last three amino acids of alpha-melanocyte-stimulating hormone (α-MSH). This article is a research-focused reference on what KPV is, how its anti-inflammatory mechanism is thought to work at the molecular level, and exactly what the preclinical evidence in gut, skin, and antimicrobial models does and does not show. For another host-defense peptide studied in innate immunity, see our reference on LL-37, the human cathelicidin. Throughout, the goal is an honest account: KPV is an investigational research compound with a real, reproducible preclinical literature but essentially no completed human clinical trials and no FDA approval for any therapeutic use.
What is KPV, and where does it come from?
KPV is a synthetic and endogenously derived tripeptide composed of the amino acids lysine (K), proline (P), and valine (V). Its structural significance comes from its parentage: it is the C-terminal fragment of α-MSH, specifically the residues at positions 11–13 of the 13-amino-acid melanocortin hormone (α-MSH 11–13).[1] Decades of melanocortin research established that much of the anti-inflammatory activity of the full α-MSH molecule is retained in this short C-terminal tail, even though the tripeptide lacks the receptor-binding “message” sequence (His-Phe-Arg-Trp) that drives pigmentation and classical melanocortin-receptor signaling.[2]
That separation of activity from the pigmentation pharmacophore is the central reason KPV attracts research interest. Investigators wanted the anti-inflammatory signal of α-MSH without the skin-darkening, appetite, and sexual-function effects mediated by melanocortin receptors. KPV appears to deliver a meaningful fraction of that anti-inflammatory activity in cell and animal models while behaving very differently from the parent hormone at the receptor level.
The historical route to KPV is worth understanding because it explains why the tripeptide is treated as a distinct research entity. α-MSH is cleaved from the large precursor protein pro-opiomelanocortin (POMC), the same precursor that yields ACTH, β-endorphin, and other melanocortins. Once the anti-inflammatory reputation of α-MSH was established in the 1990s, researchers performed classic fragment-mapping: they synthesized progressively shorter pieces of the 13-residue hormone and asked which retained the anti-inflammatory effect. The surprising answer was that the C-terminal tripeptide — KPV — carried much of the activity, even though it sits entirely outside the central His-Phe-Arg-Trp core that receptors recognize. That single observation converted KPV from a metabolic fragment into a research compound in its own right, and it framed the two questions that still drive the field: how does such a small peptide act, and can it be delivered where it is needed?
KPV structure, sequence, and molecular properties
KPV is one of the smallest bioactive peptides studied for inflammation. Its compact size is relevant to how it is absorbed and how it enters cells, both of which shape the research findings discussed below.
| Property | Value |
|---|---|
| Peptide name | KPV (also written Lys-Pro-Val, α-MSH 11–13) |
| Sequence (1-letter / 3-letter) | KPV / Lys-Pro-Val |
| Amino acids | Lysine, Proline, Valine (3 residues) |
| Molecular formula | C₁₆H₃₀N₄O₄ |
| Molecular weight | ≈342.4 g/mol |
| CAS number | 67727-97-3 |
| Parent molecule | α-melanocyte-stimulating hormone (α-MSH) |
| Regulatory status (July 2026) | Not FDA-approved; investigational / research-use-only |
Note that a related, more stable analogue frequently appears in the literature: the dimeric compound (CKPV)₂, in which two KPV units are joined through cysteine residues. Some of the anti-fungal and anti-inflammatory data attributed to “KPV” in commercial write-ups actually derives from this dimer or from the tetrapeptide GKPV (α-MSH 10–13). Where the distinction matters, this article names the specific molecule tested.
Two structural features deserve emphasis because they recur in the mechanistic discussion. First, KPV contains proline in the middle position. Proline’s rigid ring constrains the peptide’s conformation and confers relative resistance to some peptidases compared with a fully flexible tripeptide — a small stabilizing advantage, though not enough to make KPV a durable circulating drug. Second, the N-terminal lysine carries a positive charge at physiological pH, which is consistent with the cationic character shared by many antimicrobial peptides and may relate to KPV’s reported direct effects on microbial membranes. Neither feature makes KPV large or complex, but both help explain why a molecule this small can be biologically active rather than inert.
A brief timeline of KPV research
Understanding the arc of the literature helps calibrate expectations. The melanocortin anti-inflammatory story matured through the 1990s, when α-MSH was characterized as an anti-inflammatory and antipyretic neuropeptide and its C-terminal fragments were mapped for retained activity. Around the turn of the millennium, the antimicrobial dimension emerged, with reports that α-MSH and KPV directly inhibited common pathogens.[7] The most influential mechanistic and in-vivo gut work arrived in 2008, when two independent groups reported KPV’s PepT1-mediated uptake and efficacy in mouse colitis.[3][4] Comprehensive reviews consolidated the melanocortin-tripeptide field in the same period.[9] The 2010s shifted toward the delivery problem, culminating in engineered nanoparticle systems designed to concentrate KPV at inflamed colon.[6] The 2020s have been defined less by new efficacy data than by the regulatory conversation around compounding access. Read as a whole, the timeline shows a compound whose mechanism was worked out early and whose translational path has stalled at the human-trial threshold.
How does KPV work? The proposed anti-inflammatory mechanism
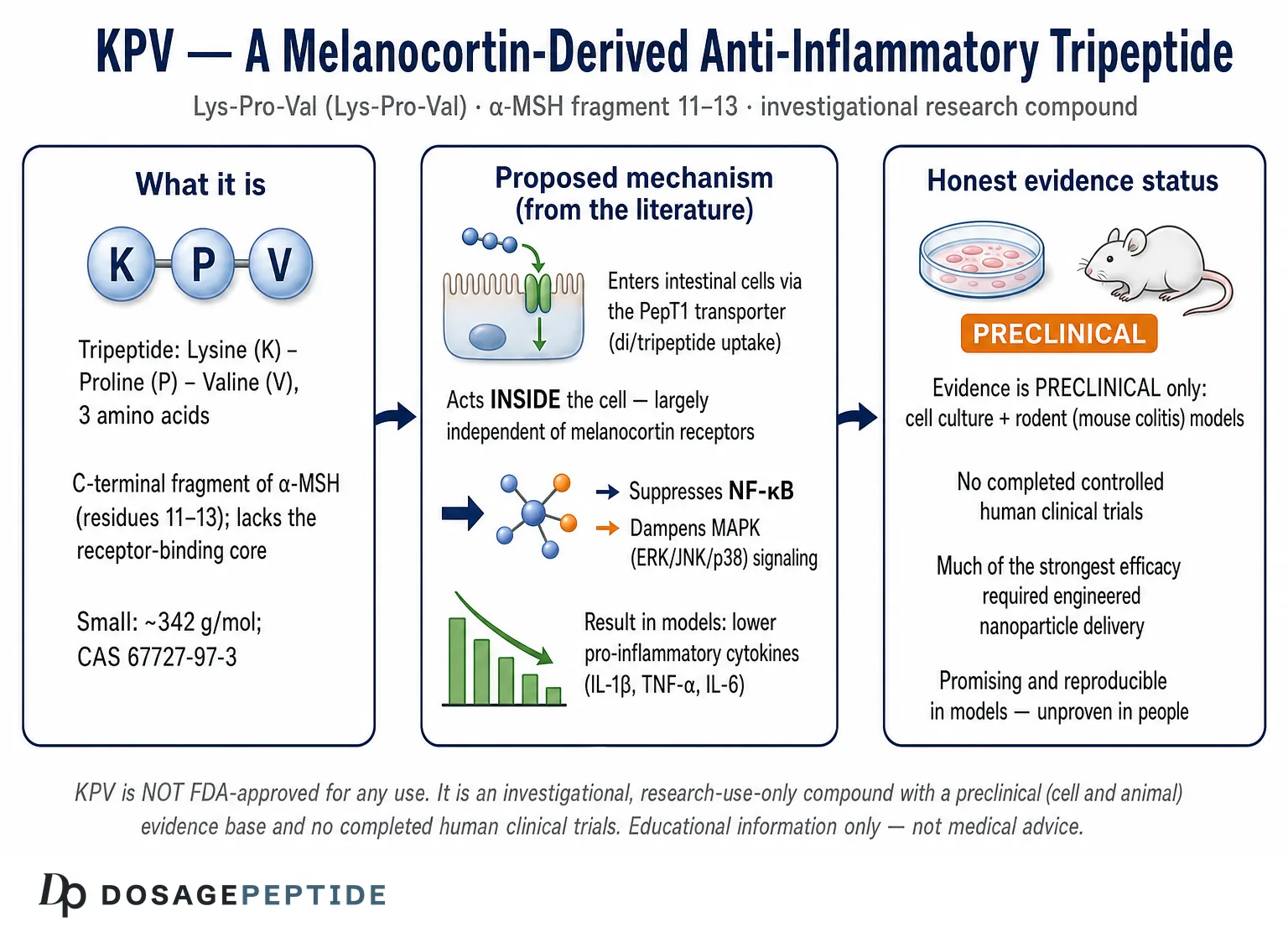
The defining feature of KPV’s proposed mechanism is that it appears to act intracellularly and largely independent of cell-surface melanocortin receptors. This is a genuine departure from how α-MSH was long assumed to work, and it is the reason KPV is studied as its own entity rather than as a mere α-MSH surrogate.
Entry into cells via the PepT1 transporter
The most rigorously characterized route by which KPV enters intestinal epithelial cells is the di/tripeptide transporter PepT1 (SLC15A1). In the landmark study by Dalmasso and colleagues, human PepT1 transported KPV into Caco2-BBE intestinal epithelial cells with high affinity — a reported Kₜ of roughly 160 µM — allowing KPV to act at low, even nanomolar, concentrations.[3] This detail matters for two reasons. First, PepT1 is normally expressed in the small intestine but is upregulated in the colon during inflammatory bowel disease, which means inflamed colonic tissue may preferentially import KPV — a built-in targeting mechanism. Second, transporter-mediated uptake means the peptide reaches the cytoplasm intact rather than depending on a surface receptor.
PepT1 (SLC15A1) is a proton-coupled oligopeptide transporter that normally shuttles di- and tripeptides — the digestion products of dietary protein — across the apical membrane of small-intestinal enterocytes. Its expression pattern is the key to KPV’s intestinal selectivity: in the healthy colon PepT1 is expressed at low levels, but in the inflamed colon of IBD it is induced. A tripeptide that is a PepT1 substrate therefore has a plausible route to accumulate preferentially in exactly the tissue where inflammation is occurring. This is a delivery logic built into the biology rather than engineered from outside, and it is one reason the gut became the flagship model system for KPV. The measured affinity (Kₜ ≈ 160 µM) sits in a range that allows meaningful uptake at the low concentrations used experimentally, and the same transporter is exploited by several approved peptidomimetic drugs, so the pathway itself is well validated in pharmacology.
Suppression of NF-κB signaling
Once inside the cell, KPV’s best-supported target is the nuclear factor-κB (NF-κB) pathway, the master transcriptional switch for many pro-inflammatory genes. Across cell models, KPV reduces NF-κB activation triggered by inflammatory stimuli such as IL-1β and TNF-α.[3] Mechanistic work on α-MSH C-terminal peptides indicates this occurs through interference with the NF-κB activation cascade — reduced degradation of the inhibitory protein IκB-α and impaired nuclear translocation of the p65/RelA subunit — so that fewer inflammatory transcripts are produced.[1] The result is lower transcription of cytokines and chemokines downstream of NF-κB.
To appreciate why targeting NF-κB is significant, it helps to recall what this transcription factor does. In a resting cell, NF-κB dimers (commonly p65/RelA paired with p50) are held inactive in the cytoplasm by inhibitory IκB proteins. When an inflammatory signal arrives — a cytokine binding its receptor, or a microbial product engaging a toll-like receptor — the IκB kinase (IKK) complex phosphorylates IκB, tagging it for degradation. Freed NF-κB then translocates to the nucleus and switches on dozens of genes: TNF-α, IL-1β, IL-6, IL-8, adhesion molecules, and inducible enzymes such as iNOS and COX-2. Because so many inflammatory outputs funnel through this one node, a molecule that partially blunts NF-κB activation can reduce a broad swath of the inflammatory response at once. That breadth is the attraction — and also the reason caution is warranted, since NF-κB is essential for normal immune defense and is not a pathway one would want to shut down completely.
Dampening of MAPK pathways
In addition to NF-κB, the Dalmasso study reported that KPV reduced IL-1β-induced phosphorylation of mitogen-activated protein kinases (MAPKs) — the ERK1/2, JNK, and p38 arms of the signaling network — further limiting the inflammatory transcriptional program.[3] Because MAPK and NF-κB signaling converge on many of the same inflammatory genes, simultaneous partial inhibition of both pathways is a plausible explanation for the cytokine reductions observed.
Reduction of pro-inflammatory cytokines
The functional readout of these upstream effects is a decrease in the pro-inflammatory mediators that NF-κB and MAPK drive. In cell and animal colitis models, KPV has been associated with reduced expression of IL-1β, TNF-α, IL-6, IL-12, IFN-γ, and the chemokine IL-8, along with reduced neutrophil infiltration as measured by myeloperoxidase activity.[3][4] Importantly, these are expression-level and tissue-level findings in models, not measured clinical outcomes in patients.
Melanocortin-receptor-independent activity
A recurring theme across the literature is that KPV’s anti-inflammatory action does not require the melanocortin-1 receptor (MC1R) or the other melanocortin receptors that mediate α-MSH’s pigmentary and neuroendocrine effects. Reviews of α-MSH-related tripeptides describe the C-terminal fragment as acting “beyond the pharmacophore,” retaining anti-inflammatory potency while shedding receptor-dependent signaling.[5] This is mechanistically important and also a caution: because the exact intracellular binding partners of KPV are not fully mapped, parts of its mechanism remain hypotheses supported by pathway-level data rather than a fully resolved molecular picture.
What is the evidence for KPV? An honest review by study type
The single most important thing to understand about KPV is the level of its evidence. The literature is genuinely interesting and internally consistent, but it is overwhelmingly preclinical: cell culture (in vitro) and rodent (in vivo) studies. There are, at the time of writing (July 2026), essentially no completed, peer-reviewed randomized human clinical trials establishing efficacy or safety for any indication. Any source presenting KPV as a “proven” treatment for gut disease, skin conditions, or infection is overstating what the data support.
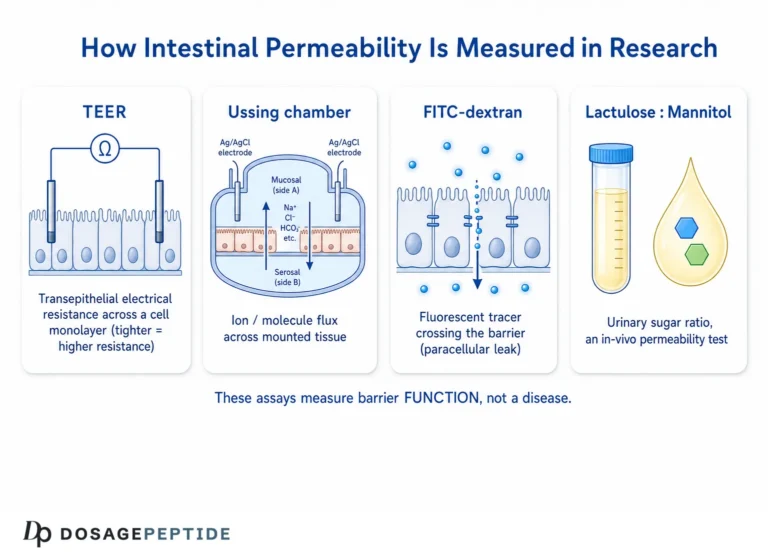
It is also worth naming what the preclinical work does and does not say about the popular “gut health” and “leaky gut” framing that surrounds KPV in consumer content. The colitis studies measured inflammation markers and disease severity in animals with induced colitis; some barrier-function readouts are implied by the Caco2-BBE tight-junction system, but the studies were not designed as tests of “intestinal permeability” in otherwise healthy subjects. The reasonable research-level statement is that KPV reduced inflammation in models of active colonic inflammation. The leap from that to “KPV heals leaky gut” in people without diagnosed disease is not supported by the cited literature and should be treated as marketing language, not science.
In-vitro (cell culture) evidence
The cell-based data are the mechanistic backbone. Using Caco2-BBE intestinal epithelial cells and Jurkat T cells, Dalmasso and colleagues showed PepT1-mediated KPV uptake, reduced NF-κB and MAPK activation, and decreased IL-8 output after inflammatory stimulation.[3] Later nanoparticle work found that macrophages exposed to KPV-loaded particles showed reduced TNF-α expression after an LPS challenge.[6] Broader melanocortin reviews document anti-inflammatory effects of KPV and related peptides in keratinocytes, fibroblasts, and immune cells.[2] These are consistent and reproducible, but in-vitro potency does not guarantee clinical benefit.
Cell-culture systems earn their place at the base of the evidence pyramid because they let researchers isolate a single mechanism under controlled conditions. In the KPV work, the Caco2-BBE line is particularly apt: it is a human colonic epithelial line that polarizes and forms tight junctions, mimicking the intestinal barrier, and it expresses PepT1. That combination let Dalmasso and colleagues demonstrate the whole chain in one system — transporter-mediated uptake, then intracellular signaling suppression, then reduced chemokine output.[3] The strength of such a design is mechanistic clarity. The weakness is everything the dish leaves out: no circulating immune cells, no microbiome, no systemic pharmacokinetics, and stimulus concentrations chosen for experimental convenience rather than physiological realism. A clean in-vitro result is a necessary starting point, not a substitute for the messier reality of a living organism.
Animal (in-vivo) evidence — colitis models
The most cited KPV animal work uses chemically induced mouse models of colitis. In the Dalmasso study, orally or luminally delivered KPV reduced disease severity in both DSS (dextran sodium sulfate) and TNBS (trinitrobenzene sulfonic acid) colitis, lowering myeloperoxidase activity and pro-inflammatory cytokine transcripts.[3] Independently, Kannengiesser and colleagues reported that the α-MSH-derived tripeptide KPV had anti-inflammatory potential in murine IBD models, with reduced colitis severity and preserved mucosal architecture, and probed its mode of action.[4] The convergence of two independent groups in different colitis paradigms is the strongest part of the KPV story — but both are rodent models, which imperfectly mirror human IBD.
The table below summarizes the direction of the key preclinical findings. These are model-level readouts — changes in tissue markers and cytokine transcripts in mice and cells — not clinical endpoints such as symptom remission in patients. They are presented to show the internal consistency of the data, not to imply proven human benefit.
| Readout | System | Reported effect of KPV |
|---|---|---|
| NF-κB activation | Caco2-BBE cells (IL-1β stimulated) | Reduced |
| MAPK phosphorylation (ERK/JNK/p38) | Caco2-BBE cells | Reduced |
| IL-8 chemokine expression | Epithelial / T-cell models | Reduced |
| Myeloperoxidase (neutrophil influx) | DSS & TNBS colitis (mouse) | Reduced |
| IL-6, IL-12 transcripts | DSS colitis (mouse) | Reduced |
| IL-1β, TNF-α, IFN-γ transcripts | TNBS colitis (mouse) | Reduced |
| TNF-α expression | LPS-stimulated macrophages (nanoparticle KPV) | Reduced |
| Overall colitis severity / histology | Murine IBD models | Improved |
Targeted-delivery and nanoparticle studies
Because a free tripeptide is rapidly absorbed in the upper gut, researchers have tested delivery systems to concentrate KPV at inflamed colonic tissue. Xiao and colleagues loaded KPV into hyaluronic-acid-functionalized nanoparticles that target CD44, a receptor overexpressed on inflamed colonic epithelium and activated macrophages, and reported efficient alleviation of ulcerative-colitis-like disease in mice at far lower KPV doses than free peptide required.[6] This line of work is scientifically elegant but underscores a practical point: much of the promising efficacy depends on engineered delivery, not simply on taking the raw peptide.
The delivery problem is central enough to KPV’s story that it deserves to be stated plainly. A free tripeptide taken orally faces a gauntlet: gastric acid, brush-border and cytosolic peptidases, and the very PepT1 transporters that absorb it in the upper small intestine before it can travel further down the gut. Even a molecule with excellent intrinsic activity can fail to reach an inflamed distal colon at a useful concentration. The hyaluronic-acid-nanoparticle approach addresses this by shielding the peptide during transit and then releasing it where CD44 is enriched on inflamed tissue and activated macrophages. Other groups have pursued polysaccharide-hydrogel and pH-responsive carriers for related colon-targeting goals. The recurring lesson is that “KPV works in colitis” is really shorthand for “KPV works in colitis when it is delivered to the right place,” and the second clause does much of the heavy lifting.
This matters for interpreting consumer-facing claims. A commercial product that is simply free KPV is not the same thing as the nanoparticle-formulated KPV that produced the strongest efficacy in the literature. Extrapolating from the engineered-delivery studies to an unformulated peptide is not scientifically justified, and it is a common overstatement in popular write-ups.
Antimicrobial evidence
Separate from inflammation, α-MSH C-terminal peptides show direct antimicrobial activity. Cutuli and colleagues reported that α-MSH and its C-terminal tripeptide KPV inhibited Staphylococcus aureus colony formation and reduced viability and germ-tube formation of the yeast Candida albicans, with effects observed even at low (physiological) concentrations.[7] A notable feature was that this antimicrobial action did not appear to impair host neutrophil killing — unusual for an anti-inflammatory agent. Related work on the dimer (CKPV)₂ has explored anti-fungal effects in a Candida vaginitis model via macrophage polarization.[8] Again: in-vitro and animal data, not human infection trials.
The antimicrobial mechanism is thought to differ from the anti-inflammatory one. Rather than working through intracellular signaling, KPV’s direct microbial effects appear to involve interaction with the pathogen itself — consistent with the cationic, membrane-active behavior seen in the broader antimicrobial-peptide family, and reported changes in microbial cyclic AMP. What makes this profile scientifically interesting is the combination: most anti-inflammatory drugs blunt inflammation partly by suppressing immune killing of microbes, whereas the melanocortin peptides in these studies reduced inflammation while leaving — and in some assays even adding to — antimicrobial defense. If that dual action held up in humans it would be unusual and valuable, but the operative word is “if”; no human infection study has tested it.
Skin, wound-healing, and dermatologic evidence
The dermatologic rationale for KPV follows directly from its mechanism: NF-κB suppression in keratinocytes and fibroblasts without corticosteroid-type tissue thinning. The skin is also, in a sense, a natural home for melanocortin biology, since α-MSH is produced in the skin and its receptors are expressed by multiple cutaneous cell types — so it is unsurprising that its anti-inflammatory C-terminal fragment shows activity there. Reviews of α-MSH-related peptides describe reduced inflammatory-mediator release from skin cells, decreased immune-cell recruitment in contact-hypersensitivity models, and support for wound closure in experimental settings.[2][9] These findings motivate interest in eczema, contact dermatitis, and psoriasis, but the human evidence for topical or systemic KPV in these conditions remains limited and largely uncontrolled.
The skin rationale is a clean illustration of KPV’s theoretical appeal and its evidentiary limits side by side. Topical corticosteroids, the mainstay of inflammatory skin disease, also suppress NF-κB, but they do so through the glucocorticoid receptor and carry well-known long-term costs: skin atrophy, telangiectasia, and tachyphylaxis. A peptide that reaches the same transcriptional node without engaging the steroid receptor is an attractive concept precisely because it might avoid those costs. That is a genuinely reasonable hypothesis grounded in mechanism. What it is not, yet, is a demonstrated clinical fact — there is no body of controlled human dermatology trials showing that KPV outperforms or safely substitutes for existing therapy. The honest position is that the skin data are hypothesis-generating.
How KPV differs from full-length α-MSH
It is easy to assume KPV is simply “α-MSH, smaller,” but the two behave differently in ways that matter for research interpretation. Full-length α-MSH engages the melanocortin receptors (MC1R through MC5R), producing pigmentation, effects on appetite and energy balance, and receptor-mediated anti-inflammatory signaling — a broad, receptor-driven profile. KPV, lacking the receptor-binding core, largely bypasses these receptors and instead acts intracellularly on NF-κB and MAPK signaling.[5] The practical consequence is that KPV can, in principle, reduce inflammation without darkening skin or triggering melanocortin-mediated systemic effects. The trade-off is that KPV likely accesses only a subset of α-MSH’s activities, and because its intracellular targets are less completely mapped than α-MSH’s receptor pharmacology, some of its mechanism remains inferred from pathway-level data rather than fully resolved.
Human clinical evidence
This section is short by necessity. There is no robust, published, controlled human trial demonstrating that KPV as an isolated tripeptide treats IBD, skin disease, or infection in people. The clinical melanocortin literature involves the parent hormone α-MSH or engineered analogues in specific contexts, not KPV monotherapy with hard efficacy endpoints. Reports of human “use” come from compounding-pharmacy and clinic settings and do not constitute trial-grade evidence. KPV should be described as investigational, with a preclinical evidence base only.
KPV vs. BPC-157 and other healing peptides
KPV is frequently discussed alongside BPC-157 and other “healing” or anti-inflammatory research peptides. They differ substantially in origin and proposed mechanism, and it is a mistake to treat them as interchangeable. The table below summarizes research-level distinctions; for a mechanism-first companion reference, see our overview of what BPC-157 is and how it is studied.
| Feature | KPV | α-MSH (parent) | BPC-157 |
|---|---|---|---|
| Type | Tripeptide (Lys-Pro-Val) | 13-aa peptide hormone | 15-aa synthetic pentadecapeptide |
| Origin | C-terminal fragment of α-MSH | Cleaved from POMC precursor | Partial sequence linked to a gastric protein |
| Proposed primary mechanism | Intracellular NF-κB / MAPK suppression; PepT1 uptake | Melanocortin-receptor signaling + anti-inflammatory C-terminus | Angiogenesis / growth-factor and nitric-oxide pathway modulation (proposed) |
| Melanocortin receptor dependence | Largely independent | Receptor-dependent (MC1R–MC5R) | Not melanocortin-based |
| Pigmentation effect | None reported | Yes (skin darkening) | None reported |
| Strongest evidence area | Rodent colitis; in-vitro anti-inflammatory | Broad anti-inflammatory (preclinical) | Rodent tendon/gut/wound models |
| Human clinical trials | Essentially none | Limited/context-specific | Essentially none |
| FDA approval | No | No (for these uses) | No |
The practical takeaway: KPV and BPC-157 are both investigational, both lack human trials, and both are studied primarily in rodents — but their proposed mechanisms are unrelated. KPV is a melanocortin-derived anti-inflammatory that works on NF-κB; BPC-157 is studied for angiogenesis-linked tissue repair. Claims that one “does the same thing” as the other are not supported by the mechanistic literature.
The comparison also clarifies where the two compounds might, in principle, occupy different research niches. KPV’s data are strongest in inflammatory contexts — colitis, cutaneous inflammation — where the goal is to quiet an overactive immune response. BPC-157’s preclinical reputation is built more on regenerative contexts — tendon, ligament, and gut-wall repair — where the goal is to accelerate healing. These are overlapping but distinct problems, and a compound optimized for one is not automatically useful for the other. This is worth stating because consumer content frequently blends the two into a generic “healing peptide” category that flattens real mechanistic differences and, in doing so, obscures how thin the human evidence is for both. A reader comparing them should hold two facts simultaneously: their proposed mechanisms differ meaningfully, and neither has cleared the bar of controlled human trials.
One more comparison point is the relationship between KPV and its own parent. Because KPV is a fragment of α-MSH, it is tempting to treat the parent hormone’s larger and older literature as though it underwrites KPV. It does not, cleanly. α-MSH acts substantially through melanocortin receptors that KPV largely bypasses, so the parent’s receptor-mediated effects — and any safety or efficacy data tied to them — cannot be assumed to carry over. KPV inherits a hypothesis from α-MSH, not a proof.
What research models are used to study KPV?
Understanding the toolbox behind the KPV literature helps calibrate how far the findings can be extrapolated. The evidence rests on a small set of standard laboratory systems.
| Model / method | What it tests | Key limitation |
|---|---|---|
| Caco2-BBE cell line | Intestinal epithelial uptake and signaling (PepT1, NF-κB, MAPK) | Immortalized cells; no immune or microbial context |
| Jurkat T cells | T-cell NF-κB response to TNF-α | Single cell type; artificial stimulation |
| DSS-induced colitis (mouse) | Epithelial-barrier-driven acute colitis | Chemical injury model; imperfect IBD analogue |
| TNBS-induced colitis (mouse) | T-cell-mediated (Th1) colitis | Hapten model; not spontaneous disease |
| LPS-stimulated macrophages | Innate cytokine output (TNF-α) | In-vitro; dose and timing artificial |
| Microbial cultures (S. aureus, C. albicans) | Direct antimicrobial activity | Plate assays; not in-host infection |
| Contact-hypersensitivity / skin models | Cutaneous inflammation and wound closure | Rodent skin; endpoints differ from human disease |
Every headline claim about KPV traces back to one or more of these systems. None of them is a human being with the target disease, which is why the honest framing is “promising in models, unproven in people.”
Pharmacology, stability, and research handling
KPV’s pharmacology is dominated by its small size. A tripeptide is a substrate for peptidases and, in the gut, for the very transporters that give it its intestinal targeting. This creates a tension: efficient PepT1 uptake in the small intestine can mean a free oral tripeptide is absorbed or degraded before reaching an inflamed colon — precisely the problem the nanoparticle delivery work was designed to solve.[6]
Routes of administration used in research
KPV has been examined across several delivery routes in the preclinical literature, and the choice of route shapes what a study can conclude. Oral and intra-colonic delivery dominate the IBD work, because the target tissue is the gut lumen and epithelium and because PepT1-mediated uptake is an intestinal phenomenon. Topical application appears in the skin and wound models, where the goal is local anti-inflammatory action in the epidermis and dermis. Parenteral (injected) administration is used in some systemic-inflammation and mechanistic studies. Each route interrogates a different aspect of the molecule: oral studies test the delivery-plus-uptake problem, topical studies isolate local tissue effects, and injected studies bypass absorption to probe intrinsic activity. Because these routes are not interchangeable, a finding from one delivery method does not automatically generalize to another — a topical anti-inflammatory result, for instance, says little about oral bioavailability.
Half-life and stability
Published, well-characterized human pharmacokinetic parameters for KPV are not established, which is itself a marker of how early-stage the compound is. As a short unmodified peptide, it is expected to have a short circulating half-life and to be susceptible to enzymatic hydrolysis; this is a general property of tripeptides rather than a KPV-specific measured value, and it should be treated as an inference, not a citable figure. The absence of solid human PK data is a genuine open question in the field.
This uncertainty is not merely academic. Without validated human half-life, absorption, and clearance figures, there is no rigorous basis for translating the concentrations used in cell and animal studies into any human exposure, which is one more reason human dosing cannot responsibly be inferred from the preclinical record. The nanoparticle and delivery research described earlier is, in part, an implicit acknowledgment of this pharmacokinetic fragility: engineered carriers exist precisely because the free peptide’s intrinsic stability and residence time were judged insufficient to reach the target reliably. In short, KPV’s pharmacology is characterized enough to explain its behavior in the laboratory and to justify continued study, but not enough to support clinical claims or exposure estimates in people.
Reconstitution and laboratory handling (research context)
In research settings, lyophilized KPV is typically supplied in vials (a 10 mg vial is a common research format) and reconstituted with a sterile diluent, kept cold, and protected from light and repeated freeze–thaw cycles — standard practice for research peptides. Because KPV is often studied both systemically and topically, handling considerations vary by the experimental route; a small tripeptide is also more sensitive to degradation than a larger, more folded peptide, which is one reason careful cold-chain handling is emphasized in the literature. For a structured, research-framed walkthrough of vial reconstitution and concentration planning specific to this compound, see our KPV 10 mg vial research protocol overview.
General laboratory technique for dissolving and calculating concentrations of any lyophilized peptide is covered in our peptide reconstitution guide, and concentration math — converting a vial’s milligram content and diluent volume into a per-unit concentration — can be worked through with our dosage calculator. These tools are provided strictly for research and educational purposes and do not constitute human dosing guidance. Unfamiliar terms used throughout this article — PepT1, NF-κB, MAPK, myeloperoxidase — are defined in our peptide research glossary.
Where does KPV sit in melanocortin biology?
KPV does not exist in a vacuum; it is one endpoint of the melanocortin system, and placing it in that context clarifies both its promise and the limits of extrapolating from its parent hormone. The melanocortin peptides — α-, β-, and γ-MSH and ACTH — are all cleaved from the precursor protein POMC and act on a family of five G-protein-coupled receptors (MC1R–MC5R). Through these receptors the system governs pigmentation (MC1R), adrenal steroid output (MC2R/ACTH), energy balance and appetite (MC3R/MC4R), and exocrine and immune functions (MC5R and others). α-MSH sits at the crossroads of pigmentation and immune modulation, which is exactly why researchers wanted to separate those roles.[2]
KPV represents an attempt to isolate the immune-modulatory arm from the rest. By stripping away the receptor-binding core, the tripeptide sheds pigmentation and the neuroendocrine effects on appetite and adrenal function, retaining a receptor-independent anti-inflammatory action. This is genuinely useful conceptually: it means the anti-inflammatory activity of the melanocortin system is not solely a downstream consequence of receptor signaling but has a component that a tiny, receptor-blind fragment can carry on its own. It is also a caution against borrowing α-MSH’s reputation wholesale — the parent hormone’s well-documented effects on pigmentation, feeding, and the HPA axis do not transfer to KPV, and neither necessarily do all of its anti-inflammatory mechanisms.
The broader melanocortin literature also situates KPV among other anti-inflammatory fragments and analogues, including the tetrapeptide GKPV and the stabilized dimer (CKPV)₂, each with its own data set.[5] This family relationship is why careful sourcing matters so much for KPV specifically: the surrounding literature is rich, but not all of it is about the exact three-amino-acid molecule.
Why is there so little human evidence, and what would change that?
A fair question for any research peptide with two decades of preclinical work is why human trials have not followed. Several structural reasons apply to KPV. As an unpatentable natural fragment, KPV offers limited commercial incentive for the expensive, multi-phase trials required for drug approval — a well-known barrier for small endogenous molecules. Its delivery challenges mean a viable human product would likely require a formulation (such as the nanoparticle systems above), which adds development complexity. And the anti-inflammatory indications it targets — IBD, inflammatory skin disease — already have competitive, evidence-backed therapies against which any newcomer must prove itself in large, controlled studies.
What would meaningfully advance the field is straightforward to state and hard to do: adequately powered, randomized, placebo-controlled human trials with objective endpoints — endoscopic and histologic remission for IBD, validated severity scores for dermatologic disease — alongside proper human pharmacokinetic and safety characterization. Until such data exist, the responsible framing does not change: KPV is a mechanistically interesting, preclinically supported, investigational compound, and any stronger claim runs ahead of the evidence.
This gap is not a criticism of the science that does exist. The preclinical work is careful, reproducible across independent laboratories, and mechanistically coherent. It is simply the wrong category of evidence to support therapeutic claims in people, and honest communication requires keeping that distinction sharp.
Limitations, open questions, and safety signals
A rigorous reading of the KPV literature reveals as much about what is unknown as about what is known:
- No human efficacy data. The entire efficacy case rests on cell and rodent studies. Rodent colitis models do not reliably predict human IBD outcomes.
- Delivery dependence. Much of the most convincing efficacy required engineered nanoparticle delivery, not the free peptide, complicating any translation to a simple product.[6]
- Incomplete mechanism. KPV’s downstream NF-κB and MAPK effects are well documented, but its precise intracellular binding partners are not fully defined; “melanocortin-independent” describes what it does not use more than it pins down what it does.
- Molecule confusion. Data from GKPV and (CKPV)₂ are sometimes reported as “KPV,” inflating the apparent evidence for the pure tripeptide.
- No established human safety profile. Without controlled trials, there is no reliable human data on dose-limiting toxicity, immunogenicity, or long-term effects. Preclinical safety at studied doses does not establish human safety.
These are not reasons to dismiss KPV — the preclinical signal is real and reproducible — but they are firm reasons to reject any characterization of KPV as a validated therapy.
A further, subtler limitation concerns purity and identity in the research-supply market. Because KPV is inexpensive to synthesize and sold widely as a research chemical, product-to-product variability in purity, actual peptide content, and even correct sequence is a real concern that the academic literature does not address — those studies used characterized, laboratory-grade material. Any inference from a published study to a specific vendor’s product assumes an equivalence that is not guaranteed. This is a general caveat for research peptides, but it applies squarely to KPV and is another reason the honest framing keeps the science and the marketplace clearly separated.
What is the regulatory status of KPV in 2026?
As of July 2026, KPV is not approved by the FDA for any therapeutic indication, and there is no licensed prescription KPV product on the US market. It has not completed the clinical-trial and approval process required for a marketed drug. KPV is appropriately described as an investigational research compound.
The regulatory picture is also actively in flux. KPV is among the peptides scheduled for evaluation by the FDA’s Pharmacy Compounding Advisory Committee, which met in late July 2026 to consider whether several peptides — including BPC-157, TB-500, and KPV — should be added to the Section 503A Bulk Drug Substances list used by compounding pharmacies.[10] The existence of such a review does not equal approval; being considered for — or removed from — a compounding list is a separate regulatory question from drug approval, and none of these peptides has been shown safe and effective through the standard approval pathway. Readers should verify the current status directly, as compounding-access decisions can change quickly.
It is useful to spell out what the different regulatory statuses actually mean, because they are easy to conflate. FDA drug approval means a compound has passed adequate and well-controlled human trials demonstrating safety and efficacy for a specific indication — KPV has not. Inclusion on the Section 503A bulk-substances list would allow compounding pharmacies to prepare a substance for individual prescriptions under certain conditions — a narrower permission that is still not approval, and one the FDA was, as of the July 2026 review, proposing not to grant for KPV and several peer peptides.[10] “Research use only” is not a regulatory endorsement of any kind; it is a category for materials sold for laboratory investigation, explicitly not for human administration. Keeping these tiers distinct is essential to reading KPV’s status honestly, and because these determinations can shift, readers should confirm the current position with primary FDA sources rather than relying on any single article.
Because of this, KPV is handled in the same category as other research-use-only peptides: studied in laboratories, discussed in the scientific literature, and not marketed as an approved treatment. Nothing in this article is medical advice or an endorsement of human use.
Frequently Asked Questions
What is KPV peptide used for in research?
In research, KPV is studied mainly as an anti-inflammatory tripeptide. The largest body of evidence involves rodent models of inflammatory bowel disease (colitis), where it reduced inflammation markers. It has also been examined in skin-inflammation, wound-healing, and antimicrobial models. All of these are preclinical uses — cell culture and animal studies — not approved human treatments.
Is KPV FDA-approved?
No. As of July 2026, KPV is not FDA-approved for any therapeutic use, and there is no licensed prescription KPV product on the US market. It is considered an investigational research compound. It was under review by the FDA’s Pharmacy Compounding Advisory Committee in July 2026, but regulatory review is not the same as approval, and no human efficacy has been established through the standard trial pathway.
How is KPV related to alpha-MSH?
KPV is the C-terminal fragment of alpha-melanocyte-stimulating hormone (α-MSH), corresponding to residues 11–13 of the hormone. It carries much of α-MSH’s anti-inflammatory activity but lacks the message sequence that drives melanocortin-receptor signaling and pigmentation, so it does not cause skin darkening. This is why KPV is studied as an anti-inflammatory without α-MSH’s pigmentary effects.
How does KPV reduce inflammation at the molecular level?
KPV appears to enter intestinal cells through the PepT1 transporter and then act inside the cell to suppress the NF-κB pathway, the master switch for many inflammatory genes. It also dampens MAPK signaling (ERK, JNK, p38). The downstream result in models is reduced production of pro-inflammatory cytokines such as IL-1β, TNF-α, and IL-6. Notably, this activity is largely independent of melanocortin receptors.
Is KPV the same as BPC-157?
No. KPV is a three-amino-acid melanocortin-derived peptide that works on NF-κB and MAPK signaling. BPC-157 is a 15-amino-acid synthetic peptide studied for tissue repair through angiogenesis-related and nitric-oxide pathways. They have different origins and different proposed mechanisms. Both are investigational and lack human trials, but they are not interchangeable and should not be described as doing “the same thing.”
Are there human clinical trials proving KPV works?
No robust, published, controlled human clinical trials establish KPV’s efficacy or safety as an isolated tripeptide for gut disease, skin conditions, or infection. The evidence base is preclinical — cell culture and rodent studies. Reports of clinic or compounding-pharmacy “use” are not trial-grade evidence. Any claim that KPV is a proven human therapy overstates the science.
Does KPV have antimicrobial activity?
In laboratory studies, α-MSH and its C-terminal tripeptide KPV inhibited the bacterium Staphylococcus aureus and the yeast Candida albicans, apparently without impairing the host’s own neutrophil killing. This is an interesting dual anti-inflammatory-plus-antimicrobial profile, but it comes from in-vitro and animal work, not human infection trials, and should not be interpreted as a treatment for infections in people.
Why are nanoparticles used to deliver KPV in studies?
Because KPV is a very small peptide, it is rapidly absorbed or degraded in the upper gut and may not reach an inflamed colon efficiently on its own. Researchers loaded KPV into hyaluronic-acid nanoparticles that target CD44, a receptor enriched on inflamed colonic tissue, achieving strong effects at much lower doses. This highlights that much of the promising efficacy depends on engineered delivery, not the raw peptide alone.
Is KPV a steroid or does it work like one?
KPV is not a steroid. It is a three-amino-acid peptide fragment of the hormone α-MSH. It is sometimes compared to corticosteroids because, in research models, both can suppress the NF-κB inflammatory pathway. But they reach that pathway differently: steroids act through the glucocorticoid receptor, whereas KPV appears to act intracellularly without that receptor. This mechanistic difference is the theoretical basis for interest in KPV, though it has not been validated by human trials.
What forms is KPV studied in?
In the literature, KPV appears as the free tripeptide, as the tetrapeptide GKPV (α-MSH 10–13), and as the stabilized dimer (CKPV)₂. It has also been formulated into hyaluronic-acid nanoparticles and other colon-targeting carriers to improve delivery. This variety matters because data from GKPV or the dimer are sometimes loosely reported as “KPV,” which can overstate the evidence for the pure tripeptide. Careful reading requires noting which exact molecule a given study tested.
Why is KPV being reviewed by the FDA in 2026?
KPV was included in a July 2026 FDA Pharmacy Compounding Advisory Committee review evaluating whether several research peptides should be added to the Section 503A list that governs what compounding pharmacies may prepare. This is a compounding-access question, separate from full drug approval. Being reviewed — or being proposed for exclusion — is not the same as being approved as safe and effective, which KPV has not been through standard clinical trials.
References
- Brzoska T, et al. α-MSH related peptides: a new class of anti-inflammatory and immunomodulating drugs. PubMed 17934097.
- Singh M, Mukhopadhyay K. Alpha-melanocyte stimulating hormone: an emerging anti-inflammatory antimicrobial peptide. BioMed Research International, 2014. PMC4130143.
- Dalmasso G, Charrier-Hisamuddin L, Nguyen HTT, Yan Y, Sitaraman S, Merlin D. PepT1-mediated tripeptide KPV uptake reduces intestinal inflammation. Gastroenterology, 2008;134(1):166–178. PMC2431115.
- Kannengiesser K, et al. Melanocortin-derived tripeptide KPV has anti-inflammatory potential in murine models of inflammatory bowel disease. Inflammatory Bowel Diseases, 2008;14(3):324–331. Oxford Academic.
- Brzoska T, et al. Terminal signal: anti-inflammatory effects of α-MSH related peptides beyond the pharmacophore. PubMed 21222263.
- Xiao B, et al. Orally targeted delivery of tripeptide KPV via hyaluronic acid-functionalized nanoparticles efficiently alleviates ulcerative colitis. Molecular Therapy, 2017. PMC5498804.
- Cutuli M, Cristiani S, Lipton JM, Catania A. Antimicrobial effects of α-MSH peptides. Journal of Leukocyte Biology, 2000;67(2):233–239. PubMed 10670585.
- Ji HX, et al. The synthetic melanocortin (CKPV)₂ exerts anti-fungal and anti-inflammatory effects against Candida albicans vaginitis via inducing macrophage M2 polarization. PLOS One, 2013. PLOS One.
- Brzoska T, Luger TA, Maaser C, Abels C, Böhm M. α-Melanocyte-stimulating hormone and related tripeptides: biochemistry, anti-inflammatory and protective effects. Endocrine Reviews, 2008;29(5):581–602. PubMed 18612139.
- US FDA. July 23–24, 2026 Meeting of the Pharmacy Compounding Advisory Committee. FDA.gov.