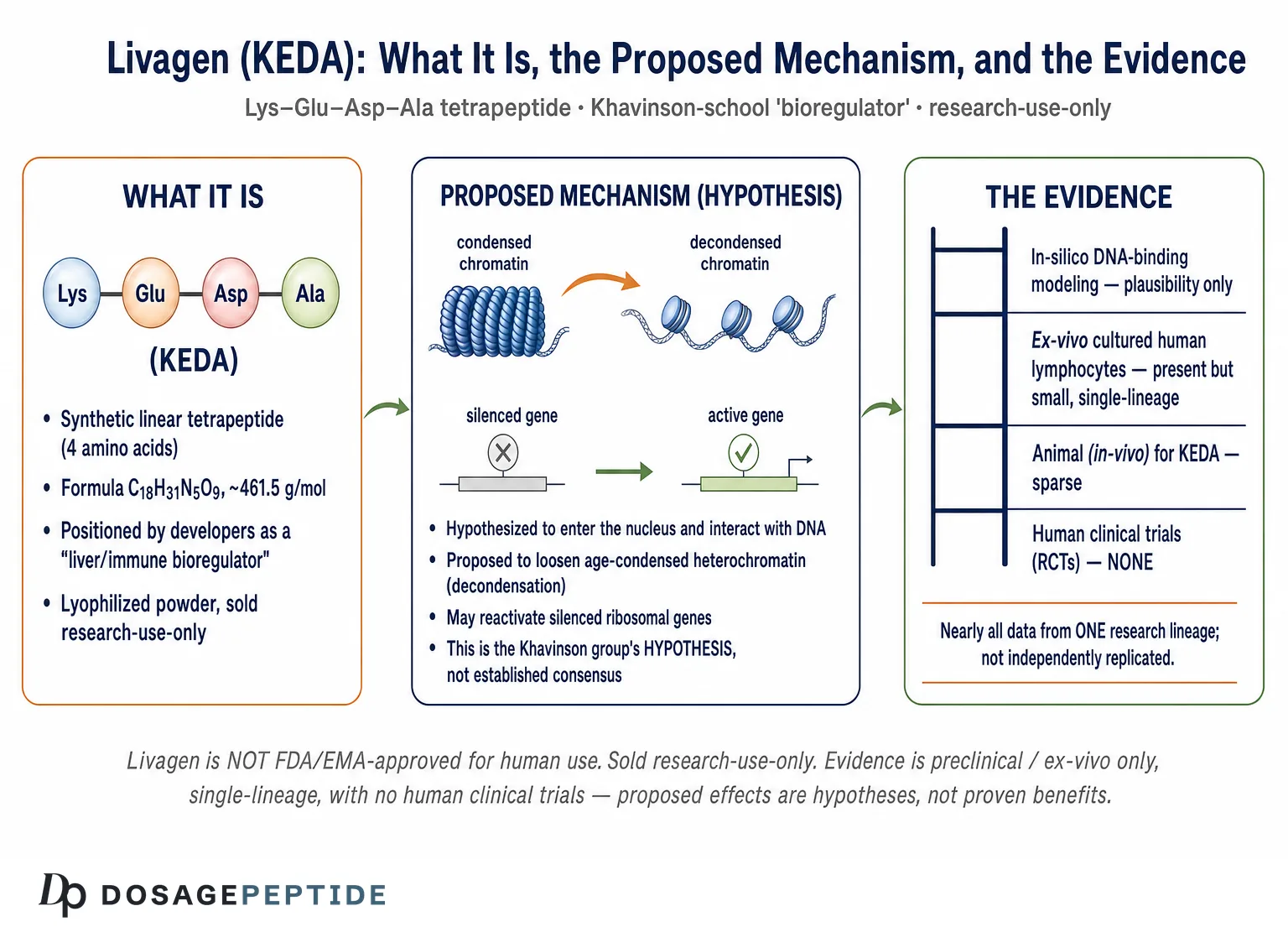
Livagen is a synthetic tetrapeptide bioregulator (sequence Lys–Glu–Asp–Ala, abbreviated KEDA) developed within the Russian “Khavinson school” of short peptide research, and the central research question surrounding it is a bold one: can a four–amino–acid molecule loosen age–condensed chromatin and switch silenced genes back on? This article is a research–framed reference on what Livagen actually is, what its proposed epigenetic mechanism claims, and—critically—how thin and how single–sourced the evidence base really is. Livagen is a research–use–only compound; it is not approved by the FDA or EMA for human therapeutic use, and the discussion below presents its proposed effects as hypotheses under investigation, not as established clinical facts.
Throughout, we separate what has been observed in a laboratory dish from what has merely been proposed, and we flag repeatedly that nearly all of the primary data comes from a single research lineage that has not been independently replicated in the West. If you are looking for practical reconstitution and handling background, see our peptide reconstitution guide, and for a fuller research protocol overview of this specific compound, the Livagen 20 mg vial dosage protocol.
What is Livagen and where does it come from?
Livagen is a member of the class of compounds usually called peptide bioregulators or, informally, Khavinson peptides. These are very short synthetic peptides—typically two to four amino acids—that emerged from work led by Professor Vladimir Khavinson and colleagues at the St. Petersburg Institute of Bioregulation and Gerontology (Russia) beginning in the late twentieth century. The founding idea behind the whole class is that each organ produces characteristic short peptides that help regulate that organ’s own gene expression, and that supplying a synthetic version of such a peptide might restore more youthful patterns of gene activity in aging tissue.[1]
Within that family, Livagen (KEDA) is generally described as a liver–associated bioregulator, positioned by its developers as a compound intended to influence hepatic and immune–cell gene expression. It is structurally and conceptually close to Vilon (the dipeptide Lys–Glu, or KE), which is the smallest and best–studied member of this immediate group. In effect, Livagen can be read as a KEDA “extension” of the KE motif that sits at the heart of Vilon. For a deeper look at that parent dipeptide, see our explainer on what Vilon is and how the lysyl–glutamic acid peptide works.
The single most useful frame for a newcomer is this: Livagen is an investigational research peptide with an ambitious epigenetic hypothesis and a thin, single–lineage evidence base. It is not a proven anti–aging therapy, not a licensed liver medicine, and not something with human clinical–trial support. Everything credible that can be said about it lives at the level of laboratory cell studies and mechanistic modeling. Holding that frame steady is what separates an honest reference from the promotional material that dominates search results for this compound.
It is important to be clear about provenance from the outset. Livagen is not a molecule with a long, independent, multi–laboratory research history. The overwhelming majority of primary data on Livagen specifically comes from the Khavinson group and its close collaborators (including the Georgian cytogenetics group led by T. Lezhava). That does not make the findings wrong, but it does mean the compound sits in an evidentiary category very different from a peptide that has been studied by dozens of unaffiliated teams. We return to this replication problem in detail below.
The historical context: why the bioregulator program exists
To evaluate Livagen fairly, it helps to understand the research program that produced it. The Khavinson school grew out of Soviet–era work, beginning in the 1970s, on tissue extracts—initially complex peptide preparations isolated from animal organs such as the thymus (Thymalin), the pineal gland (Epithalamin), and the retina and cortex. The observation that drove decades of subsequent work was that these crude organ extracts appeared, in the group’s hands, to influence the function of the corresponding organ and to affect markers of aging in experimental animals. The program then moved from complex, poorly–defined extracts toward defined synthetic short peptides—the idea being to identify the minimal active amino–acid sequence responsible for a given tissue effect and to synthesize it as a pure, reproducible chemical entity.
Livagen sits in that lineage as one of the “second generation” defined peptides. Where the dipeptide Vilon (KE) was distilled as a thymic/immune bioregulator, Livagen (KEDA) was positioned by its developers as a liver–oriented bioregulator. Understanding this history matters for two reasons. First, it explains why the mechanism claims are so ambitious: the entire program is built on the premise that short peptides carry tissue–specific gene–regulatory information. Second, it explains the evidentiary structure—a large body of internally consistent work from one school, published substantially in Russian–language and Russian–affiliated journals, rather than a distributed literature accumulated by competing independent laboratories. Both the ambition and the insularity are relevant when weighing the claims.
Naming, abbreviations, and what “bioregulator” means here
You will see Livagen referred to by several labels: its trade–style name Livagen, its single–letter sequence KEDA, and its full residue sequence Lys–Glu–Asp–Ala. The word “bioregulator” in this literature is a term of art from the Khavinson school rather than a standard pharmacological classification; it denotes a short peptide proposed to act as a tissue–specific regulator of gene expression. Readers should not assume “bioregulator” implies any regulatory approval, standardized potency, or validated clinical endpoint—it does not. If you encounter unfamiliar terms while reading peptide literature, our peptide glossary defines many of them.
A related terminology trap is the distinction between peptide bioregulators (defined synthetic short peptides like Livagen) and peptide bioregulator complexes or cytamines/cytomax (the older, complex organ–extract preparations from which the class descended). Marketing copy sometimes conflates the two, borrowing the somewhat larger clinical–use history of the extract preparations to lend weight to a defined synthetic peptide that has its own, thinner, evidence base. When reading about Livagen, insist on evidence that is specifically about the KEDA tetrapeptide, not about a related organ extract or a differently–sequenced sibling peptide.
What is the chemical structure of Livagen?
Livagen is a linear tetrapeptide. Its defining features are summarized below and are consistent across chemical reference listings, including the molecular formula C18H31N5O9 and molar mass of roughly 461.5 g/mol.[7]
| Property | Value |
|---|---|
| Peptide class | Synthetic short–peptide bioregulator (Khavinson class) |
| Amino acid sequence | Lys–Glu–Asp–Ala (KEDA) |
| Single–letter code | KEDA |
| Peptide form | H–Lys–Glu–Asp–Ala–OH (free N– and C–termini) |
| Molecular formula | C18H31N5O9 |
| Molecular weight | ≈461.5 g/mol |
| Physical form (as supplied) | Lyophilized (freeze–dried) white powder |
| Regulatory status | Research–use–only; not FDA/EMA approved for human therapy |
Each of the four residues contributes something to the proposed behavior of the molecule. Lysine (Lys, K) carries a positively charged side chain at physiological pH; glutamic acid (Glu, E) and aspartic acid (Asp, D) carry negatively charged carboxylate side chains; and alanine (Ala, A) is a small, neutral, hydrophobic residue. This mix of a cationic residue with two anionic residues is exactly the kind of charged, compact motif that the Khavinson group proposes can interact electrostatically with DNA—a point we develop in the mechanism section.
Why a four–residue peptide is such an unusual candidate
It is worth pausing on how small Livagen is. Most peptides that have entered clinical use—insulin, GLP–1 agonists, growth–hormone secretagogues—are much larger, fold into defined shapes, and act through well–characterized cell–surface receptors. A tetrapeptide has essentially no stable three–dimensional fold; it is a short, flexible string of four residues. Conventional pharmacology would not expect such a molecule to carry a specific, tissue–targeted “instruction.” The whole interest of the Khavinson claim—and the whole reason to be cautious—is that it proposes a mode of action (direct, sequence–selective interaction with DNA and chromatin) that is not how the vast majority of known peptides behave. When a mechanism sits so far outside established pharmacology, the evidentiary bar for accepting it should be correspondingly high. That is the lens through which the rest of this article evaluates Livagen.
Zinc coordination and metal–peptide interactions
A secondary structural feature reported in parts of the Russian literature is that some of these short peptides, including KEDA, may coordinate metal ions such as zinc through their charged side chains, and that metal–peptide interactions may modulate their effects on chromatin. This has been explored in the context of how bioregulators interact with heavy metals during aging. This is a niche, mechanistically–framed line of inquiry rather than a validated functional property, and it should be read as a research curiosity about peptide–metal chemistry rather than an established feature of how Livagen “works” in any therapeutic sense.
How Livagen relates to KE and the wider peptide family
The KE dipeptide (Lys–Glu) is the recurring “core” motif of this group. Vilon is essentially KE; Livagen is KEDA; and other members extend or vary the sequence to target different tissues. This shared architecture is one reason the proposed mechanisms of these peptides are described in nearly identical language across the literature—they are being studied by the same group, using the same assays, under the same theoretical framework. The similarity is a strength for internal consistency but a weakness for independent validation, because the findings are not being stress–tested by outside laboratories using different methods.
What is the proposed mechanism of action of Livagen?
The mechanism attributed to Livagen is the single most important—and most contested—part of its story, so it deserves careful, honest handling. What follows is the Khavinson group’s specific hypothesis, not an established consensus.
The epigenetic / chromatin–decondensation model
The core claim is that Livagen acts as an epigenetic modulator that reverses some of the chromatin changes associated with aging. In aging cells, portions of the genome become progressively packed into tightly condensed heterochromatin. Heterochromatin is transcriptionally quiet, so genes trapped in these condensed regions are effectively silenced. The Khavinson model proposes that Livagen (and related peptides) can trigger decondensation—a loosening or “unpacking” of condensed chromatin, sometimes called deheterochromatinization—thereby making previously silenced genes accessible for transcription again.[2]
Two specific downstream observations are repeatedly reported by the group for Livagen:
- Reactivation of ribosomal genes. The peptides are reported to reactivate ribosomal RNA genes (in the nucleolar organizer regions) that had become silenced by age–related condensation. Because ribosomal genes drive the cell’s protein–synthesis machinery, their reactivation is presented as a plausible route to “restored” cellular function.[2]
- Decondensation of pericentromeric structural heterochromatin. In the group’s cytogenetic work, Livagen (together with Epithalon) was distinguished by inducing decondensation of the pericentromeric structural heterochromatin of chromosomes 1 and 9—regions that normally remain tightly packed even in young cells.[2]
The proposed “peptide–DNA complementarity” mechanism
How could a four–residue peptide plausibly reach chromatin at all? The Khavinson framework hypothesizes that these small peptides can cross the cell membrane and the nuclear envelope, enter the nucleus, and interact directly with DNA—binding preferentially to specific short nucleotide sequences and thereby influencing whether nearby genes are transcribed. This idea is sometimes described as peptide–DNA complementarity: a given short peptide is proposed to “match” a particular DNA motif.[1]
The strongest independent–looking support for the plausibility (not the therapeutic reality) of this idea comes from a computational study published in a mainstream, high–profile journal, Nucleic Acids Research. That paper systematically modeled how all possible dipeptides could bind double–stranded DNA and identified a subset of dipeptides—including the KE motif central to this peptide family—as capable of sequence–selective binding in a DNA groove.[3] This is genuinely interesting and lends the “peptides can bind DNA motifs” premise some credibility at the level of molecular modeling. However, two caveats are essential: (a) Khavinson is a co–author of that modeling paper, so it is not fully independent of the originating school; and (b) demonstrating that a dipeptide can bind a DNA motif in silico is a very long way from proving that Livagen enters human nuclei in vivo and produces a beneficial, clinically meaningful change in gene expression.
Immune and interleukin modulation
Because these peptides are studied largely in lymphocytes and are historically linked to thymic/immune bioregulation (the KE dipeptide arose from thymus–peptide research), the model also proposes immune modulation—for example, effects on lymphocyte gene activity and cytokine/interleukin expression in aged immune cells. In the Livagen literature specifically, the immune angle is tied to the observation that its chromatin effects were measured in lymphocytes drawn from elderly donors, with the interpretation that reactivating silenced genes could partially counter aspects of immune aging. Again, this is an interpretive hypothesis layered on top of laboratory cytogenetic observations, not a demonstrated clinical immunotherapy effect.
The immune framing is reinforced by the closely related Vilon work. In a 2004 Biogerontology paper, the parent dipeptide Vilon (KE) was reported to reactivate chromatin in cultured lymphocytes from old people, using the same cytogenetic approach later applied to Livagen.[6] Because Vilon and Livagen share the KE core, the group interprets their overlapping chromatin effects as evidence of a coherent, motif–driven mechanism across the family. A skeptic would note the alternative reading: that the same laboratory, using the same assay on the same kind of cells, tends to report the same kind of result across structurally similar peptides—which is exactly what independent replication is designed to test and which has not been done at scale.
What the mechanism claim does NOT establish
It is worth being explicit about the boundary of the mechanism claim, because marketing language routinely oversteps it. Even taken entirely at face value, the chromatin–decondensation model establishes only that, in a culture dish, adding Livagen to elderly lymphocytes was associated with cytogenetic changes consistent with looser chromatin. It does not establish that Livagen is absorbed intact when administered, that it reaches target tissues, that it selectively acts on the “right” genes, that any resulting gene–expression change is durable, or that the net effect on a living organism is beneficial rather than neutral or harmful. Each of those is a separate, unproven step. The gap between “associated with chromatin decondensation in vitro” and “improves liver function or extends healthspan in people” spans essentially the entire drug–development pipeline, none of which has been completed for Livagen.
What does the actual evidence show, by study type?
Honest evaluation of Livagen requires sorting the evidence into tiers and refusing to let a lower tier masquerade as a higher one. Here is the evidence landscape, from strongest available to entirely absent.
In–vitro / ex–vivo cytogenetic studies (the core of the evidence)
The primary, compound–specific evidence for Livagen is a small set of ex–vivo cytogenetic studies on cultured human lymphocytes, mostly from elderly donors. The landmark Livagen–specific paper is Khavinson and colleagues’ 2002 report in the Bulletin of Experimental Biology and Medicine, “Effects of Livagen Peptide on Chromatin Activation in Lymphocytes from Old People.” In that work, Livagen added to cultured lymphocytes from elderly subjects was reported to activate ribosomal genes and decondense age–condensed heterochromatin.[4]
A companion 2004 paper in the same journal, “Effects of Short Peptides on Lymphocyte Chromatin in Senile Subjects” (Khavinson, Lezhava, Malinin), compared five peptides—Vilon, Epithalon, Livagen, Prostamax, and Cortagen—in lymphocytes from subjects aged roughly 75–88 years. All five reportedly activated ribosomal genes and decondensed chromatin fibrils, and Livagen (with Epithalon) was singled out for effects on the pericentromeric heterochromatin of chromosomes 1 and 9.[2] Related cytogenetic work by the Georgian collaborators extended these observations, including a 2007 Annals of the New York Academy of Sciences paper describing bioregulator effects on pericentromeric and telomeric heterochromatin and on chromosomal damage induced by metal ions in lymphocytes from very old individuals (roughly 80–91 years).[5]
What this tier can and cannot support is worth stating plainly. It can support the claim that, in the hands of this group, in cultured lymphocytes, Livagen was associated with cytogenetic markers of chromatin decondensation. It cannot support claims about liver disease outcomes, longevity, immune restoration in living humans, or any clinical benefit—none of those endpoints were measured.
There are also methodological features of this study tier that a careful reader should weigh. The studies are generally small, the donor numbers are limited, and the endpoints are cytogenetic scores that require expert interpretation and can be sensitive to scoring conventions. Blinding and pre–registration—now standard expectations for reducing bias—are not features of this older literature. And crucially, the comparison group in these designs is typically “treated versus untreated cells from the same aged donors,” which speaks to an in–dish effect of the peptide but says nothing about whether the same thing would happen in an intact human body. None of these caveats prove the findings false; they simply place them where they belong—early, exploratory, hypothesis–generating laboratory work.
What about liver–specific evidence?
Livagen is marketed heavily as a “liver bioregulator,” so it is fair to ask what liver–specific data actually exist. The honest answer is that the liver framing derives largely from the peptide’s positioning within the organ–peptide theory—the idea that KEDA is a liver–associated regulatory motif—rather than from a body of controlled hepatology studies demonstrating improved liver function, reduced fibrosis, or better outcomes in liver disease. The measured effects that anchor the compound’s reputation are the lymphocyte chromatin observations, not liver–function endpoints. A reader should therefore treat “Livagen supports liver health” as a marketing extrapolation from mechanism–theory, not as an evidence–backed clinical claim.
Animal (in–vivo) studies
For the KEDA peptide specifically, robust, independently reported in–vivo animal efficacy data are sparse. The broader bioregulator class has an extensive Russian–language animal literature (lifespan and tumor–incidence studies in rodents for peptides such as Epithalon and Vilon), but caution is required: findings for one member of the class should not be silently transferred to Livagen, because the peptides differ in sequence and proposed tissue targets. Where you see sweeping “anti–aging” animal claims attached to Livagen online, the underlying data are usually either from a different peptide or from the same small cytogenetic lineage rather than from independent in–vivo Livagen trials.
This distinction matters more than it might seem. The strongest animal claims in the entire bioregulator field—rodent lifespan extension and reduced spontaneous tumor incidence—are most often attached to Epithalon (AEDG) and, to a lesser extent, Vilon (KE). Livagen (KEDA) does not carry an equivalent, well–characterized in–vivo efficacy dossier of its own. When those headline rodent numbers are recycled onto Livagen product pages, they are borrowing credibility from a different molecule. A rigorous reader treats each peptide’s animal evidence as compound–specific and declines to average the family into a single “proven in animals” impression.
Human clinical trials
This tier is, for practical purposes, empty. There are no published randomized controlled trials of Livagen, and no Livagen trials are registered on ClinicalTrials.gov. The human–derived data that exist are the ex–vivo lymphocyte studies described above—human cells studied in a dish—not clinical trials in living patients with defined endpoints, control groups, blinding, and safety monitoring. Any source presenting Livagen as “clinically proven” for liver health, immunity, or longevity is overstating the evidence. The correct summary is: preclinical and ex–vivo only, single–lineage, not clinically validated.
| Evidence tier | Status for Livagen (KEDA) | What it can support |
|---|---|---|
| In–silico / molecular modeling | Present (dipeptide–DNA binding, KE motif) | Plausibility that short peptides can bind DNA motifs |
| In–vitro / ex–vivo (human lymphocytes) | Present but single–lineage, small | Association with chromatin decondensation markers in cultured cells |
| Animal (in–vivo) | Sparse for KEDA specifically | Little; class–level data should not be transferred |
| Human RCTs | None | Nothing—no clinical efficacy or safety established |
What research models and methods were used to study Livagen?
Understanding the methods clarifies exactly how narrow the evidence base is. The signature Livagen experiments share a common design.
Cultured human lymphocytes from elderly donors
The characteristic model is peripheral blood lymphocytes cultured from elderly human donors (frequently in the 75–91 year range), sometimes compared against younger controls. Peptide is added to the culture, and chromatin state is assessed. This is an ex–vivo design: it uses genuine human cells but studies them outside the body, which is why it must not be described as a “clinical trial.”
Cytogenetic and chromatin assays
The readouts are cytogenetic and biophysical rather than clinical:
- Nucleolar organizer region (NOR) staining to assess ribosomal–gene activity, often via silver staining of the acrocentric chromosomes.
- C–banding and heterochromatin analysis to evaluate the condensation state of pericentromeric structural (C–) heterochromatin on specific chromosomes (notably 1, 9, and 16).
- Thermal denaturation / melting analysis of chromatin to quantify how tightly packed the chromatin is.
- Sister chromatid exchange (SCE) assays, sometimes combined with metal–ion challenge (e.g., cobalt), to probe chromosomal stability and damage.[5]
Computational / molecular–modeling methods
Separately, the plausibility of direct peptide–DNA interaction has been probed computationally, most notably in the Nucleic Acids Research systematic modeling of dipeptide binding to double–stranded DNA. That analysis identified a subset of dipeptides—on the order of a few dozen out of all possible pairs—capable of selective binding, with the KE dipeptide flagged as a selective binder to a particular tetranucleotide motif.[3] These methods speak to mechanistic plausibility, not to therapeutic effect.
How to read a study built on these methods
A practical takeaway for anyone reading the Livagen literature: match the method to the claim. A silver–stained NOR count tells you about ribosomal–gene activity in a dish; it does not tell you about protein synthesis in a living liver. A C–banding score tells you about heterochromatin condensation in a metaphase spread; it does not tell you about immune competence in an aging person. A docking simulation tells you whether a peptide could fit a DNA groove; it does not tell you whether that binding happens at physiological concentrations inside a human nucleus, or what it would do there. Keeping the method–to–claim mapping strict is the single most useful habit for cutting through the noise around this compound.
What is the pharmacology and handling profile of Livagen?
Because Livagen has never gone through formal human pharmacokinetic development, its pharmacology is described in general peptide terms rather than from validated human PK studies.
Structure, stability, and half–life
As a small, unmodified linear tetrapeptide, Livagen would be expected—on general biochemical principles—to have a very short plasma half–life if introduced into a living system, because short peptides are rapidly cleaved by peptidases. It is important to label this as an inference from peptide chemistry, not a measured human value: there is no validated, published human half–life for Livagen. This uncertainty is itself a limitation, because the proposed mechanism (nuclear entry and DNA interaction) presupposes that intact peptide reaches the nucleus, which has not been demonstrated pharmacokinetically in humans.
This creates a genuine internal tension in the Livagen story that is rarely acknowledged. On one hand, the compound is proposed to act by entering the nucleus intact and interacting with DNA—a demanding delivery requirement. On the other hand, a tiny linear peptide like KEDA is precisely the sort of molecule that peptidases in blood, tissue, and cells degrade quickly, and that has poor membrane permeability without a delivery vehicle. Reconciling “acts on nuclear DNA” with “degraded within minutes and poorly membrane–permeant” is a real mechanistic hurdle. Proponents sometimes argue that even fragments or transient exposure could trigger downstream signaling, but that is a hypothesis, not a resolved pharmacokinetic fact. Anyone claiming a defined, favorable pharmacokinetic profile for Livagen is going beyond the published data.
Absorption route and formulation
Because there is no approved human formulation, there is likewise no established, validated route of administration or bioavailability figure for Livagen as a therapeutic. Some bioregulators in this family have been explored in oral/sublingual forms in the Russian supplement market and others in injectable research forms, but bioavailability by any route has not been rigorously established for KEDA in peer–reviewed Western pharmacokinetic studies. This absence is not a minor footnote—without knowing how much intact peptide reaches the circulation and then the target cell nucleus, the mechanistic model cannot be considered validated in vivo.
Reconstitution and research handling
Livagen is supplied as a lyophilized powder for laboratory research. General, research–framed handling practices reported by suppliers and consistent with standard peptide handling include:
- Dry storage: the lyophilized powder is relatively stable and is often stored refrigerated (2–8 °C), with freezing (≤ −20 °C) for long–term storage, protected from light.
- Reconstitution: dissolved using bacteriostatic water under aseptic technique; a 20 mg vial reconstituted with 3.0 mL yields roughly 6.7 mg/mL.
- After reconstitution: kept refrigerated and used within a limited window (commonly cited as up to about 30 days), not re–frozen.
These are laboratory handling notes for research material, not administration instructions. For the mechanics of reconstitution generally, see our peptide reconstitution guide; for the compound–specific research protocol write–up, see the Livagen 20 mg vial dosage protocol.
How does Livagen compare to Vilon, Vesugen, and Epithalon?
Livagen is best understood alongside its sibling bioregulators. They share the same theoretical framework and much of the same research group, but differ in sequence, size, and proposed tissue target.
| Peptide | Sequence | Length / MW (approx.) | Proposed target focus | Human RCT evidence |
|---|---|---|---|---|
| Livagen | Lys–Glu–Asp–Ala (KEDA) | Tetrapeptide / ≈461.5 g/mol | Liver / immune–cell gene expression, chromatin decondensation | None |
| Vilon | Lys–Glu (KE) | Dipeptide / ≈275 g/mol | Thymus / immune bioregulation | None (Western RCTs) |
| Vesugen | Lys–Glu–Asp (KED) | Tripeptide / ≈390 g/mol | Vascular wall / endothelium | None (Western RCTs) |
| Epithalon | Ala–Glu–Asp–Gly (AEDG) | Tetrapeptide / ≈390 g/mol | Pineal / telomerase, chromatin | None (Western RCTs) |
A few relationships are worth emphasizing. Vilon (KE) is essentially the shared “core” motif; Vesugen (KED) adds an aspartate and is positioned as the vascular member; and Livagen (KEDA) adds an alanine on top of the KED–like backbone. Epithalon (AEDG) is a different sequence entirely and is the member most associated with telomerase claims. In the shared cytogenetic experiments, Epithalon and Livagen are the two most often reported to act on the deep pericentromeric heterochromatin of chromosomes 1 and 9, whereas the others act more on ribosomal–gene reactivation and facultative heterochromatin.[2]
For fuller treatments of the two most directly comparable siblings, see our guides on Vilon (the lysyl–glutamic acid dipeptide) and Vesugen, the vascular bioregulator. One caution: because these peptides are so often studied together by the same group, their online marketing tends to blur their evidence bases into a single “bioregulators work” narrative. Each should be judged on its own compound–specific data, which for Livagen is limited to the ex–vivo cytogenetic studies described here.
Shared strengths and shared weaknesses across the family
It is analytically useful to separate what these peptides share from what distinguishes them, because their evidence profiles have a common shape.
| Attribute | Shared across the family | Implication for Livagen |
|---|---|---|
| Theoretical framework | Organ–peptide, direct gene–regulation hypothesis | Ambitious, non–standard mechanism; high evidentiary bar |
| Primary evidence type | Ex–vivo cytogenetics + rodent/Russian literature | No human RCTs; surrogate endpoints only |
| Research provenance | Single school + close collaborators | Independent replication largely absent |
| Regulatory status (West) | Research–use–only; not FDA/EMA approved | Not a validated therapeutic |
| Distinguishing feature | Sequence, size, proposed tissue target | Livagen = KEDA, liver/immune, chr. 1 & 9 effects |
The practical consequence is that a claim demonstrated (even weakly) for one family member should not be silently imported to Livagen, and vice versa. The peptides share a hypothesis, not a validated body of interchangeable clinical evidence. When a source supports a Livagen claim by citing an Epithalon telomerase study or a Vilon immune study, that is a category error worth flagging.
What are the limitations, open questions, and safety signals?
This is the section that most peptide marketing pages omit, and it is the most important one for a YMYL topic.
The replication problem is the central limitation
The overriding issue with Livagen is that its evidence base is concentrated in one research lineage and has not been independently replicated by unaffiliated Western laboratories. The chromatin–decondensation findings come from the Khavinson group and its Georgian cytogenetic collaborators; the molecular–modeling support co–lists Khavinson as an author. In science, extraordinary claims—such as a four–residue peptide selectively reprogramming gene expression—require independent replication before they can be treated as established. That independent replication has not, to date, occurred at scale. Until it does, the honest scientific posture is skepticism, not endorsement.
Why does single–lineage evidence deserve extra caution rather than extra credit for consistency? Because internal consistency is exactly what you would expect from a single team applying a single method under a single guiding hypothesis—whether or not the underlying effect is real. Consistency within a lab is not the same as reproducibility across labs. The history of biomedical research is full of striking findings that looked robust within their originating group and then failed to replicate when independent teams applied blinded, pre–registered protocols. This is not an accusation of misconduct; it is the ordinary reason the scientific community treats independent replication—not repetition by the same group—as the currency of credibility. Livagen simply has not been through that process.
Mechanistic gaps
- Nuclear delivery is assumed, not proven in vivo. The model requires intact peptide to reach the nucleus of living human cells. Given rapid peptidase cleavage of short peptides, whether meaningful intact Livagen reaches human nuclei in vivo is unresolved.
- From cytogenetic marker to clinical benefit is a huge leap. Even if Livagen loosens chromatin in cultured lymphocytes, it does not follow that this improves liver function, immunity, or lifespan in a person. Decondensing chromatin is not inherently “good”—context matters, and inappropriate gene reactivation could in principle be harmful.
- Endpoints measured are surrogate, not outcome. Ribosomal–gene activation and heterochromatin melting are laboratory surrogates, not validated clinical outcomes.
Safety signals and unknowns
Because there are no human clinical trials, there is no formal human safety, toxicology, or adverse–event dataset for Livagen. The bioregulator class is often described as low–toxicity in the originating literature, but “no reported toxicity in a small, single–lineage literature” is very different from “demonstrated safe.” A specific conceptual concern for any compound proposed to alter gene expression and reactivate silenced heterochromatin is the theoretical risk of activating genes that are silenced for good reason. None of this has been characterized in controlled human studies. The correct statement is that Livagen’s human safety profile is unknown.
Beyond the compound itself, the research–chemical supply channel introduces its own risks that are independent of Livagen’s biology. Products sold as “Livagen” are not manufactured under pharmaceutical quality systems, and purity, identity, correct sequence, endotoxin content, and sterility can vary between suppliers and lots. A certificate of analysis (COA) from an independent laboratory is the minimum verification a researcher should expect, but even a COA does not turn a research chemical into a validated medicine. These quality–control uncertainties are a practical safety consideration entirely separate from the (also unresolved) question of the peptide’s intrinsic pharmacology.
Open research questions
If Livagen were to be studied rigorously, the questions that would need answering are clear and, notably, mostly unanswered today:
- Does Livagen reach and enter human cell nuclei intact in vivo, and at what concentrations?
- If chromatin decondensation occurs in vivo, which specific genes are affected, and is the pattern beneficial, neutral, or harmful?
- Do the in–dish cytogenetic findings replicate in independent laboratories using blinded, pre–registered designs?
- Are there any measurable clinical endpoints—liver function, immune parameters, healthspan markers—that change with administration in controlled human trials?
- What is the dose–response and safety profile across a realistic range of exposures?
Until these are addressed, Livagen remains an interesting mechanistic hypothesis in search of the confirmatory, independent, in–vivo and clinical evidence that would move it out of the research–curiosity category.
What is the regulatory status of Livagen?
As of mid–2026, Livagen is not approved by the U.S. FDA, the EMA, or any other major Western regulatory agency for human therapeutic use. It is not a licensed pharmaceutical product in those jurisdictions. In the United States it is sold only as a research chemical, labeled for laboratory and research use only, and it is not intended for human consumption or clinical administration. There are no Livagen trials registered on ClinicalTrials.gov.
The picture in Russia is different: some peptide bioregulators developed by this school have historically been registered domestically (as pharmaceuticals or supplements) within the Russian regulatory system, and Livagen belongs to that broader lineage. However, a domestic Russian registration is not equivalent to FDA/EMA approval and does not reflect the same evidentiary bar for efficacy and safety. For a Western reader, the operative facts are simple: research–use–only, not approved for human therapeutic use, no registered clinical trials.
What “research–use–only” actually means
The phrase “research use only” (RUO) is not a marketing softener—it is a meaningful legal and practical boundary. A compound sold RUO has not been evaluated by regulators for safety or efficacy in humans, is not manufactured to pharmaceutical standards, and is not permitted to be marketed with therapeutic claims or sold for human consumption. Product pages that pair an RUO label with wellness–style benefit language (“supports liver health,” “anti–aging”) are in tension with that status. For a young, YMYL–sensitive audience, the responsible reading is to treat Livagen as a laboratory reagent whose human effects are unproven, and to disregard therapeutic framing that the evidence does not support.
Why the regulatory gap is unlikely to close soon
Bringing a compound like Livagen to approval would require the full arc of modern drug development: characterized pharmacokinetics, reproducible mechanism, dose–ranging, and adequately powered, controlled human trials with meaningful endpoints. That pathway is expensive and is typically driven by patent–protected commercial sponsors. A decades–old, widely–sold, unpatentable short peptide has little commercial incentive attached to it, which is part of why—despite years of availability—the confirmatory Western evidence has not materialized. This is a structural reason to expect the evidence gap to persist, and another reason to keep expectations grounded.
How is Livagen handled in a research setting?
In legitimate research contexts, Livagen is treated like any other research–grade lyophilized peptide: stored appropriately, reconstituted with bacteriostatic water under aseptic technique, kept refrigerated after reconstitution, and used within a limited stability window. Documentation of source, lot, and certificate of analysis (COA) is standard practice for research materials so that purity and identity can be verified. None of this constitutes guidance for human use; it is research material handling. For the general procedure, our reconstitution guide covers dilution math, bacteriostatic water, and storage, and the Livagen 20 mg vial dosage protocol page collects the compound–specific research details in one place.
Frequently Asked Questions
What is Livagen used for?
In research, Livagen (KEDA) is used to study chromatin biology and epigenetic aging—specifically whether a short peptide can decondense age–condensed heterochromatin and reactivate silenced genes in cultured human lymphocytes. It is often described as a liver/immune bioregulator. It has no approved human therapeutic use and is sold as a research–use–only compound, not a treatment for any condition.
Is Livagen FDA approved?
No. As of 2026, Livagen is not approved by the FDA, EMA, or any major Western regulator for human therapeutic use. It is available only as a research chemical labeled for laboratory use, and it is not intended for human consumption. No Livagen clinical trials are registered on ClinicalTrials.gov. Some related bioregulators have domestic Russian registrations, which are not equivalent to FDA approval.
How does Livagen supposedly work?
The Khavinson group hypothesizes that Livagen enters the cell nucleus and interacts with DNA, loosening tightly packed heterochromatin (deheterochromatinization) so that age–silenced genes—including ribosomal genes—can be transcribed again. This is a proposed epigenetic mechanism supported mainly by that group’s ex–vivo lymphocyte studies and by computational DNA–binding modeling. It is not an independently established mechanism.
Is there human clinical evidence for Livagen?
No randomized controlled human trials of Livagen have been published, and none are registered. The human–derived data are ex–vivo cytogenetic studies—human lymphocytes cultured in a dish and treated with the peptide—not clinical trials with patients, controls, and clinical endpoints. Sources calling Livagen “clinically proven” for liver, immune, or anti–aging benefits are overstating the evidence.
How is Livagen different from Vilon and Vesugen?
All three are Khavinson–school bioregulators sharing the KE (Lys–Glu) core. Vilon is the KE dipeptide (thymic/immune focus); Vesugen is the KED tripeptide (vascular focus); and Livagen is the KEDA tetrapeptide (liver/immune focus). They differ in length, molecular weight, and proposed tissue target, but share the same unreplicated epigenetic hypothesis and none have Western clinical–trial validation.
Why is the evidence for Livagen considered weak?
Because it is single–sourced. Nearly all primary Livagen data come from one research lineage (the Khavinson group and its close collaborators), using the same cytogenetic assays, without independent Western replication. The findings are also surrogate laboratory markers (chromatin state, ribosomal–gene activity) rather than clinical outcomes, and there are no in–vivo human trials to confirm any benefit.
What are the risks of Livagen?
Livagen’s human safety profile is unknown—there is no formal toxicology or adverse–event dataset from controlled human trials. A theoretical concern for any compound that reactivates silenced genes is inappropriate gene activation. Absence of reported toxicity in a small single–lineage literature is not the same as demonstrated safety. It should be treated as an investigational research compound only.
How is Livagen stored and reconstituted for research?
Livagen ships as a lyophilized powder, typically stored refrigerated (2–8 °C) or frozen for long–term storage, protected from light. For research use it is reconstituted with bacteriostatic water under aseptic technique—for example, 3 mL into a 20 mg vial (≈6.7 mg/mL)—then kept refrigerated and used within a limited window. These are material–handling notes, not human–use instructions.
References
- Khavinson VKh, Lezhava TA, Monaselidze JR, et al. Peptide Epitalon activates chromatin at the old age. Neuro Endocrinol Lett. 2003;24(5):329–333. PMID: 14647006. https://pubmed.ncbi.nlm.nih.gov/14647006/
- Khavinson VKh, Lezhava TA, Malinin VV. Effects of short peptides on lymphocyte chromatin in senile subjects. Bull Exp Biol Med. 2004;137(1):78–81. PMID: 15085253. https://pubmed.ncbi.nlm.nih.gov/15085253/
- Kolchina N, Khavinson V, Linkova N, et al. Systematic search for structural motifs of peptide binding to double–stranded DNA. Nucleic Acids Res. 2019;47(20):10553–10563. doi:10.1093/nar/gkz850. https://academic.oup.com/nar/article/47/20/10553/5584680
- Khavinson VKh, Lezhava TA, Monaselidze JG, et al. Effects of Livagen Peptide on Chromatin Activation in Lymphocytes from Old People. Bull Exp Biol Med. 2002;134(4):389–392. doi:10.1023/A:1021924702103. https://link.springer.com/article/10.1023/A:1021924702103
- Lezhava T, Jokhadze T. Activation of pericentromeric and telomeric heterochromatin in cultured lymphocytes from old individuals. Ann N Y Acad Sci. 2007;1100:387–399. PMID: 17460203. https://pubmed.ncbi.nlm.nih.gov/17460203/
- Lezhava T, Khavinson V, Monaselidze J, et al. Bioregulator Vilon–Induced Reactivation of Chromatin in Cultured Lymphocytes from Old People. Biogerontology. 2004;5(2):73–79. PMID: 15105581. https://link.springer.com/article/10.1023/B:BGEN.0000025070.90330.7f
- Livagen. Wikipedia (chemical identity, formula C18H31N5O9, molar mass, sequence, regulatory context). https://en.wikipedia.org/wiki/Livagen