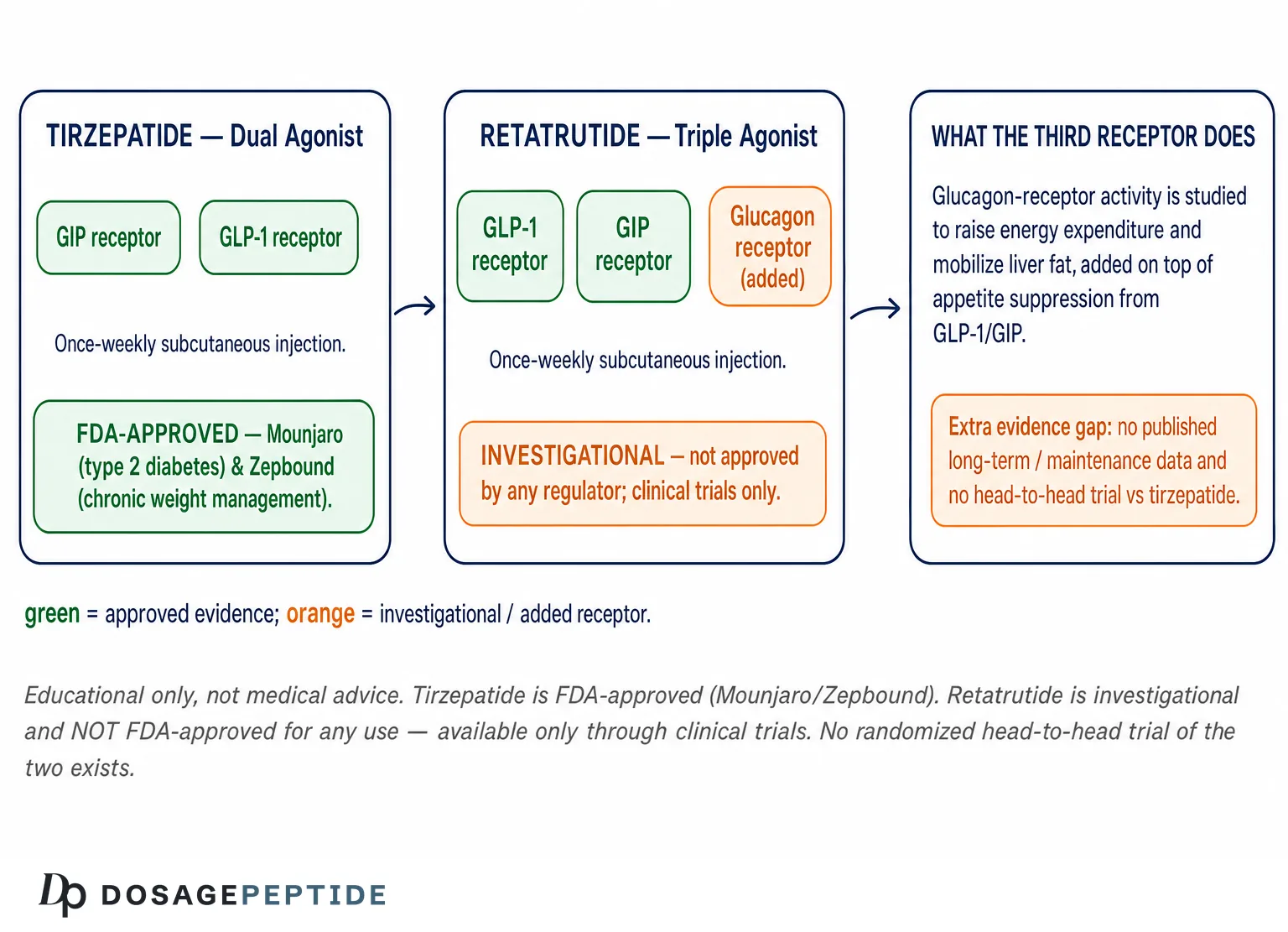
Two once-weekly injectable peptides have come to define the modern conversation about pharmacological weight loss: tirzepatide, an approved dual GIP/GLP-1 receptor agonist, and retatrutide, an investigational triple GcGR/GIP/GLP-1 agonist that adds glucagon-receptor activity to the same incretin backbone. This article compares the two on mechanism, weight-loss efficacy, glycemic and lipid effects, tolerability, dosing cadence, and regulatory status — drawing only on published trial data and clearly flagging where evidence is early or cross-trial rather than head-to-head. Everything below is educational and research-oriented; it is not medical advice, and it does not describe an approved use of retatrutide.
Why compare retatrutide and tirzepatide at all?
Both molecules belong to the incretin-mimetic class that has reshaped obesity medicine, but they occupy very different positions on the evidence and regulatory map. Tirzepatide is FDA-approved and marketed as Mounjaro for type 2 diabetes and Zepbound for chronic weight management, backed by a large phase 3 program with multi-year follow-up. Retatrutide is investigational: as of this writing it has completed a landmark phase 2 trial and its sponsor has reported positive phase 3 topline results, but it is not approved by any regulator and is available only through clinical trials.
The comparison is worth making precisely because the two drugs share a design philosophy — multi-receptor agonism — yet differ by a single, consequential receptor. Tirzepatide engages the GIP and GLP-1 receptors; retatrutide adds the glucagon receptor. That third target is the whole story of why retatrutide is being studied, and understanding it is the key to reading the trial numbers correctly. Throughout, we will separate what is demonstrated from what is plausible, and we will be explicit that no randomized head-to-head trial has yet compared these two agents directly.
A note on how to read the numbers
Weight-loss percentages from different trials are not directly comparable. They come from different populations, different treatment durations, different placebo runs, and different statistical estimands (for example, the “efficacy” estimand that assumes continued treatment versus the “treatment-regimen” estimand that counts discontinuations). When we place a tirzepatide figure next to a retatrutide figure, we are describing each trial’s own headline result, not the outcome of a controlled comparison. Treat every cross-trial contrast in this article as suggestive context rather than proof of superiority.
What is tirzepatide and how does it work?
Tirzepatide is a once-weekly subcutaneous peptide that activates two incretin receptors simultaneously: the glucose-dependent insulinotropic polypeptide (GIP) receptor and the glucagon-like peptide-1 (GLP-1) receptor. GLP-1 receptor agonism is the better-known of the two mechanisms; it suppresses appetite, slows gastric emptying, and enhances glucose-dependent insulin secretion. GIP receptor agonism is more nuanced. On its own GIP has complex metabolic effects, but when co-activated alongside GLP-1 it appears to amplify weight-loss and glycemic benefits and may improve gastrointestinal tolerability relative to GLP-1 activity alone.
The clinical payoff of this dual mechanism was established in the SURMOUNT-1 trial, a phase 3 randomized, double-blind, placebo-controlled study of 2,539 adults with obesity or overweight without diabetes. Over 72 weeks, mean weight reduction reached 15.0% on the 5 mg dose, 19.5% on 10 mg, and 22.5% on the 15 mg dose, versus roughly 2.4% with placebo, using the efficacy estimand; 96% of participants on the two higher doses achieved at least 5% weight loss.[1] These results made tirzepatide the most effective approved obesity pharmacotherapy at the time of its launch.
Two design features of SURMOUNT-1 are worth understanding because they recur throughout this comparison. First, the trial ran for a long 72 weeks, which matters because incretin-driven weight loss accrues slowly and the curves in these studies keep descending for a year or more before flattening. A short trial systematically understates a drug’s eventual effect. Second, the trial reported results under more than one statistical estimand. The efficacy estimand estimates what happens if a participant takes the drug as intended, while the treatment-regimen estimand counts everyone as randomized, including those who stopped early — and therefore produces smaller numbers. When you see two different figures quoted for the same trial (for example, roughly 22.5% versus roughly 20.9% for tirzepatide 15 mg), the gap usually reflects which estimand is being cited, not a contradiction in the data.
How GIP and GLP-1 signaling combine
The biology underneath tirzepatide is more subtle than “two appetite drugs stacked together.” GLP-1 receptor agonism acts on hypothalamic and hindbrain circuits that govern hunger and satiety, and peripherally it delays gastric emptying so that a meal produces prolonged fullness. GIP receptor signaling contributes through partly separate pathways: it influences energy balance, adipose-tissue handling of nutrients, and central appetite circuits, and it may temper the nausea that GLP-1 agonism can provoke. The net effect of co-agonism has repeatedly exceeded what GLP-1 agonism alone achieves in cross-trial terms, which is the practical evidence that the second receptor is doing real work. This is the template retatrutide inherits and extends.
Approved indications and formulations
Tirzepatide is approved in two branded forms. Mounjaro is indicated for glycemic control in type 2 diabetes, where it produces large reductions in HbA1c alongside weight loss. Zepbound is indicated for chronic weight management in adults with obesity, or overweight with at least one weight-related comorbidity. Both are once-weekly subcutaneous injections titrated upward over weeks to a maintenance dose, a schedule designed to blunt gastrointestinal side effects. For readers researching preparation and measurement, our tirzepatide 5 mg vial dosage protocol and the general peptide reconstitution guide walk through the arithmetic in a research context.
What is retatrutide and how is its mechanism different?
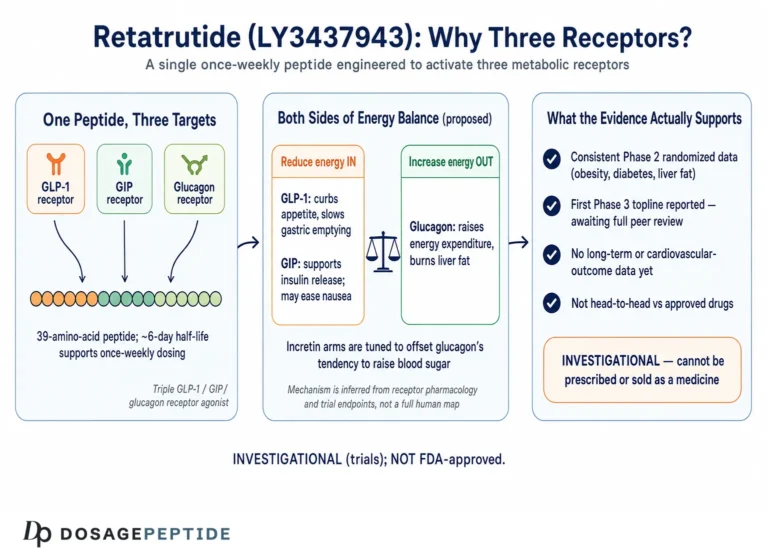
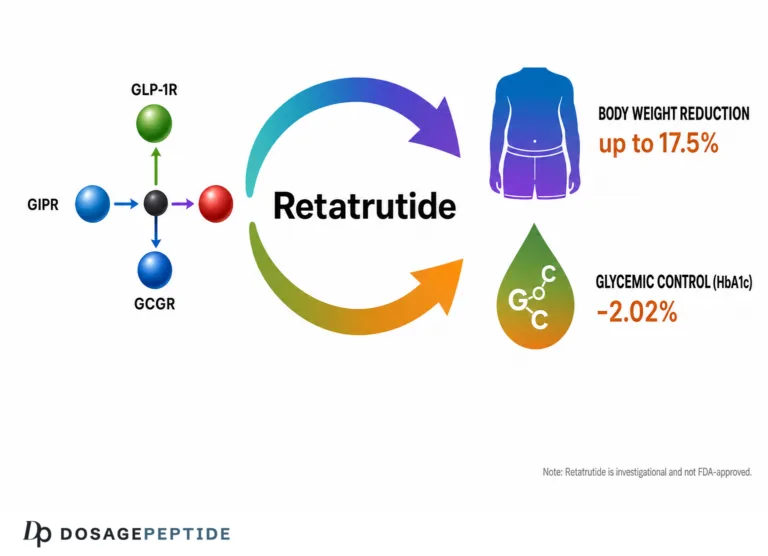
Retatrutide (development code LY3437943) is a once-weekly subcutaneous peptide that activates three receptors: the glucagon receptor (GcGR), the GIP receptor, and the GLP-1 receptor. It shares tirzepatide’s incretin backbone but adds glucagon-receptor agonism — hence the shorthand “triple G” or “triple agonist.” The addition is deliberate and counterintuitive to anyone who remembers glucagon primarily as the hormone that raises blood sugar.
The rationale is that glucagon-receptor agonism increases energy expenditure and promotes hepatic lipid mobilization, effectively adding a “burn” component on top of the “eat less” component supplied by GLP-1. The potential risk — that glucagon might worsen glycemia — is offset in the molecule by the powerful glucose-lowering, insulinotropic action of concurrent GLP-1 and GIP agonism. In principle, the three signals are balanced so that appetite falls, energy output rises, and glucose control is preserved or improved. Whether that balance holds across long-term use in diverse patients is exactly what the phase 3 program is designed to answer.
The phase 2 signal that put retatrutide on the map
The pivotal early evidence is the phase 2 trial published in the New England Journal of Medicine in 2023, which randomized 338 adults with obesity to escalating retatrutide doses or placebo over 48 weeks. Mean weight reduction reached 24.2% on the 12 mg dose (and about 22.8% on 8 mg), versus 2.1% with placebo — and, notably, the weight-loss curves had not yet plateaued at week 48, suggesting the ceiling had not been reached.[2] That combination of magnitude and momentum is what generated the intense interest in retatrutide as a potential next step beyond dual agonism.
The phase 2 dose-response was orderly, which is reassuring from a pharmacology standpoint because a clean dose-dependence argues that the effect is real and mechanism-driven rather than an artifact. The trial tested several dose tiers, and higher maintenance doses produced progressively greater weight loss, as summarized below. These are phase 2 figures from a single mid-stage trial and should be read as an early signal, not a settled result.
| Retatrutide maintenance dose | Approx. mean weight loss at 48 weeks (phase 2) |
|---|---|
| Placebo | ~2.1% |
| 1 mg | ~8.7% |
| 4 mg | ~17.1% |
| 8 mg | ~22.8% |
| 12 mg | ~24.2% |
What that table captures is the reason retatrutide became the most-watched molecule in obesity research: even mid-range doses produced weight loss competitive with the best approved therapy, and the top dose exceeded it — in a shorter trial, on curves still trending downward.
Why add glucagon at all?
To appreciate the design gamble, it helps to recall that glucagon is conventionally the hormone that opposes insulin and raises blood glucose — the last thing an obesity or diabetes drug would seem to want. But glucagon also has effects that are useful for weight loss when they can be harnessed safely: it increases resting energy expenditure, promotes the breakdown and export of fat from the liver, and can suppress appetite through central pathways. The engineering insight behind retatrutide is that pairing glucagon-receptor agonism with strong GLP-1 and GIP agonism lets the beneficial energy-expenditure and hepatic effects come through while the incretin activity neutralizes the unwanted glucose elevation. The phase 2 glycemic data, in which retatrutide lowered rather than raised HbA1c in participants with diabetes, are the practical evidence that the balance held in that trial.
Retatrutide remains investigational and is not approved for any use. Readers researching the dosing arithmetic used in trials can consult our retatrutide 6 mg vial dosage protocol, which is provided strictly for educational reference and not as a recommendation to use an unapproved drug.
Dual agonism versus triple agonism: the receptor logic
The cleanest way to understand why these two drugs behave differently is to think of each receptor as a distinct lever on body weight and metabolism. Tirzepatide pulls two levers hard; retatrutide pulls three.
GLP-1: the appetite brake
GLP-1 receptor agonism is the foundation of both molecules. It reduces appetite through central and peripheral pathways, slows gastric emptying so meals feel filling for longer, and stimulates insulin release in a glucose-dependent manner. This is the mechanism shared by first-generation agents like semaglutide, and it is the primary driver of the weight loss seen across the entire class. For a fuller treatment of this hormone, see our explainer on key peptide and metabolic terms.
GIP: the potentiator
GIP receptor agonism is the second lever in both drugs. Co-activated with GLP-1, GIP appears to enhance weight-loss efficacy and glycemic control and may improve tolerability. Its precise contribution is still an area of active research, but the clinical signal from tirzepatide — larger weight loss than GLP-1 monotherapy in cross-trial comparisons — is consistent with a real additive effect. In the metabolic-triad framing, GIP is the amplifier that makes the other levers hit harder.
Glucagon: the energy-expenditure dial
Glucagon-receptor agonism is retatrutide’s distinguishing third lever. Beyond its classic role in glucose metabolism, glucagon raises resting energy expenditure and drives hepatic fat mobilization. In a molecule that simultaneously activates GLP-1 and GIP to keep glucose in check, this glucagon component is hypothesized to push weight loss further and to deliver outsized benefits for liver fat. The strongest evidence for the liver-fat effect comes from a phase 2a study in which retatrutide reduced hepatic lipid content by roughly 81–82% at the 8 mg and 12 mg doses over 24 weeks, with the majority of participants reaching normal liver fat — among the most pronounced pharmacological liver-fat reductions reported in a clinical trial.[3]
How do the weight-loss numbers compare across trials?
Here the cross-trial caveat matters most. The headline figures below come from separate trials with different durations and populations, so read them as each drug’s own best-published result rather than as a controlled contest.
Tirzepatide (SURMOUNT-1, 72 weeks): up to 22.5% mean weight loss on 15 mg in adults without diabetes.[1]
Retatrutide (phase 2, 48 weeks): up to 24.2% mean weight loss on 12 mg, with curves still descending at study end.[2]
Two features stand out. First, retatrutide reached a numerically larger mean weight loss in less time (48 versus 72 weeks), which is part of why it attracted so much attention. Second, retatrutide’s phase 2 result came from a smaller, earlier-stage trial than tirzepatide’s phase 3 program — a fundamental difference in evidence weight. A large phase 3 trial with hard endpoints and long follow-up is a far stronger basis for clinical decisions than a phase 2 signal, however impressive that signal is.
What the phase 3 retatrutide data now show
The evidence picture has moved recently. Retatrutide’s sponsor has reported positive phase 3 topline results from the TRIUMPH program, with company-disclosed figures describing mean weight reductions on the order of roughly 19% at the 4 mg dose up to approximately 28% at the 12 mg dose over 80 weeks in adults with obesity and a weight-related comorbidity without diabetes. Because these detailed results were first communicated through the sponsor rather than a peer-reviewed journal at the time of writing, they should be treated as company-reported topline data pending full publication and regulatory review, not yet as the settled peer-reviewed record. If confirmed on publication, they would extend retatrutide’s efficacy signal from phase 2 into a large, long-duration phase 3 population — but approval decisions still lie ahead.
Putting the class in context: where semaglutide fits
It helps to anchor both drugs against the first-generation benchmark. In the STEP-1 trial, once-weekly semaglutide (a GLP-1 receptor agonist) produced a mean weight loss of 14.9% at 68 weeks.[4] Tirzepatide’s dual mechanism pushed that ceiling into the low-20s, and retatrutide’s triple mechanism appears, in early data, to push it further still. The trajectory across GLP-1 → dual → triple agonism is a clean illustration of how adding receptor targets has correlated with larger average weight loss. For readers comparing the older agent, see our semaglutide 5 mg vial dosage protocol.
One caution keeps this progression honest, however. Correlation across a class is not the same as a guarantee that each additional receptor delivers a proportional, safe, and durable gain. Adding targets also adds complexity, potential off-target effects, and new safety questions — the transient heart-rate rise seen with retatrutide is a concrete example of a signal that appears with the third receptor and not with the first two. The history of drug development is full of mechanisms that looked cleanly additive in early data and proved more complicated at scale. So the upward line from semaglutide to tirzepatide to retatrutide is best read as a hypothesis strongly supported by early evidence, not as a law guaranteeing that triple agonism will end up strictly superior once the full safety and durability picture is in. That is precisely why the completed, published phase 3 record matters so much for retatrutide, and why an approved drug with years of data behind it retains a real advantage even against a challenger posting bigger headline numbers.
Side-by-side comparison table
| Category | Retatrutide | Tirzepatide |
|---|---|---|
| Mechanism | Triple agonist: GcGR + GIP + GLP-1 | Dual agonist: GIP + GLP-1 |
| Regulatory status | Investigational; phase 3 (TRIUMPH) reported, not approved | FDA-approved (Mounjaro, Zepbound) |
| Peak weight loss (own trial) | ~24.2% at 48 wks (phase 2, 12 mg) | ~22.5% at 72 wks (SURMOUNT-1, 15 mg) |
| Phase 3 status | Topline reported (~28% at 12 mg, sponsor data) | Full phase 3 program published |
| Maintenance data | Pending peer-reviewed phase 3 publication | ~25% maintained at 88 wks (SURMOUNT-4) |
| Dosing | Once-weekly subcutaneous, titrated | Once-weekly subcutaneous, titrated |
| Notable extra signal | Large hepatic fat reduction; transient ↑ heart rate | Established glycemic control; cardiometabolic benefits |
| Key labeled/observed risks | GI events; transient heart-rate increase | GI events; thyroid C-cell boxed warning; gallbladder risk |
| Access today | Clinical trials only | Commercially available; coverage varies |
The table crystallizes the trade-off. Retatrutide leads on early efficacy signal and liver-fat effect; tirzepatide leads decisively on evidence depth, durability data, and the fact that it is actually approved and obtainable.
How durable is the weight loss, and what happens if you stop?
Efficacy at a single timepoint is only half the story; obesity is a chronic condition, and what happens over years matters as much as what happens over months. Here tirzepatide has a decisive evidence advantage because its program includes a dedicated maintenance trial.
Tirzepatide maintenance: the SURMOUNT-4 evidence
The SURMOUNT-4 trial used a randomized-withdrawal design: all participants took open-label tirzepatide for 36 weeks (reaching a mean weight reduction of about 20.9%), then were randomized either to continue the drug or switch to placebo for another 52 weeks. Those who continued tirzepatide lost an additional 5.5%, reaching an overall mean reduction of 25.3% from baseline to week 88. Those switched to placebo regained about 14% of their body weight.[5] The message is unambiguous: the weight loss is maintained — and even extended — only while treatment continues, and stopping leads to substantial regain.
Retatrutide durability: not yet in the peer-reviewed record
Retatrutide has no equivalent published long-term maintenance trial yet. Its phase 2 data end at 48 weeks with weight still falling, and the phase 3 topline figures, while extending the duration to 80 weeks, remain sponsor-reported pending full publication. It is reasonable to hypothesize that retatrutide, like every drug in this class, will require continued use to preserve its effect, but that expectation is an extrapolation from class behavior rather than a demonstrated finding for this specific molecule. This is a genuine gap in the retatrutide evidence base and one of the clearest points in tirzepatide’s favor today.
The broader lesson from SURMOUNT-4 — and from the withdrawal extension of the STEP-1 semaglutide trial, which showed the same rebound pattern — is that these drugs treat the physiology of appetite and energy balance while they are present in the body, not the underlying predisposition to weight gain. When the drug is removed, the compensatory biology that defends a higher body-weight set point reasserts itself. This reframes the entire comparison: the relevant question is rarely “how much weight can a drug take off in a year” but “how much can be kept off over a decade of continued, tolerable therapy.” On that longer horizon, tirzepatide has actual data and retatrutide has, so far, only a promising short-to-medium-term trajectory.
How do they compare on glycemic control?
Both drugs improve glucose metabolism, but the depth of evidence again differs sharply.
Tirzepatide has a full diabetes program behind its Mounjaro indication, with consistent, large HbA1c reductions and a favorable weight profile that make it a standard-of-care option in type 2 diabetes. Its glucose-lowering is well characterized across the SURPASS trials and confirmed in real-world use.
Retatrutide’s glycemic story is more preliminary but encouraging. Because glucagon-receptor agonism could theoretically raise glucose, the phase 2 program specifically examined participants with type 2 diabetes and found that retatrutide lowered HbA1c rather than raising it — evidence that the molecule’s GLP-1 and GIP activity more than offsets any glucagon-driven glucose elevation. A dedicated phase 3 diabetes trial is part of the TRIUMPH program, and its published results will be the real test of retatrutide’s glycemic profile. Until then, tirzepatide is the only one of the two with an approved, evidence-backed diabetes indication.
This point deserves emphasis because it is the crux of the whole triple-agonist bet. The single biggest theoretical objection to adding glucagon to an obesity drug is that it could worsen glucose control — a serious problem in a population where prediabetes and diabetes are common. The phase 2 diabetes data are the first real-world rebuttal to that objection: not only did glucose control not deteriorate, it improved. If the phase 3 diabetes trial confirms this at scale, it would establish that the triple-agonist design solved its central engineering risk. If it does not, glycemic safety could become the limiting factor. Either way, this is a question that only completed, published phase 3 data can answer, and it is one of the most important things to watch in the retatrutide program.
How do they compare on lipids and cardiometabolic markers?
Weight loss of this magnitude tends to improve the whole cardiometabolic panel — blood pressure, triglycerides, and glycemic markers all typically move in a favorable direction — and both drugs show that pattern.
Tirzepatide has documented improvements in blood pressure, lipids, and other cardiometabolic parameters across its phase 3 program, consistent with its degree of weight loss, and cardiovascular outcome data continue to accumulate. Retatrutide’s phase 2 data included favorable movement in lipid markers, including reductions in non-HDL cholesterol and triglycerides, alongside its striking effect on liver fat.[3] The hepatic-fat result is arguably retatrutide’s most distinctive cardiometabolic feature and reflects the glucagon component of its mechanism directly.
It is worth dwelling on why the liver-fat finding is so striking, because it is the clearest place where the triple mechanism appears to do something the dual mechanism does not do as forcefully. Metabolic dysfunction-associated steatotic liver disease (MASLD, formerly NAFLD) is closely coupled to obesity and insulin resistance, and it is a major driver of long-term cardiometabolic and liver risk. Glucagon-receptor agonism directly promotes hepatic fat oxidation and export, so a drug that safely engages that receptor would be expected to clear liver fat faster than one relying on weight loss alone to do it indirectly. The phase 2a data — relative hepatic-fat reductions above 80% at the higher doses, with most participants reaching a normal liver-fat level in 24 weeks — are consistent with exactly that prediction. Tirzepatide also improves liver fat, largely as a downstream consequence of its substantial weight loss, but the retatrutide signal stands out for its magnitude and its apparent mechanistic directness. If it holds up in larger, biopsy-confirmed studies, hepatic steatosis could become one of the areas where triple agonism has the strongest differentiated rationale — though, as with everything about this molecule, that remains to be confirmed in the full program.
One caveat specific to retatrutide is the observed transient increase in heart rate, which rose early, peaked around week 24, and then declined over the remainder of the phase 2 trial. Heart-rate changes are seen across the incretin class, but the glucagon component may contribute here, and the long-term clinical significance is precisely the kind of question phase 3 cardiovascular follow-up is meant to resolve. This is a signal to watch, not a demonstrated harm.
How do the two drugs compare on tolerability and safety?
Gastrointestinal side effects are the defining tolerability issue for the entire incretin class, and both drugs share that profile. Nausea, vomiting, diarrhea, and constipation are the most common adverse events, are generally mild to moderate, are dose-related, and cluster during the dose-escalation phase. Slow, stepwise titration is the standard strategy for minimizing them and improving adherence for both agents.
The reason titration works is mechanistic. Much of the nausea traces to GLP-1’s delay of gastric emptying and its action on brainstem nausea circuits; the gut and brain adapt to a given exposure over a few weeks, so introducing the drug at a low dose and stepping up gradually lets tolerance develop before the next increment. Skipping steps or escalating too quickly is the most common cause of intolerable symptoms and of early discontinuation. In practice this means the first two to three months of any incretin therapy are the hardest, after which most people who were going to tolerate the drug have done so. It also means the two drugs’ real-world tolerability is shaped as much by how carefully they are titrated as by any intrinsic difference between them.
How the two tolerability profiles differ in emphasis
Although the GI picture is broadly similar, the emphasis differs. Tirzepatide’s tolerability is exhaustively documented across a large program, and the addition of GIP agonism is thought to make it somewhat gentler on the gut than pure high-dose GLP-1 agonism at comparable efficacy. Retatrutide’s GI profile in phase 2 also resembled the class, but its distinctive feature is the transient tachycardia — a heart-rate rise that is not a prominent feature of tirzepatide and that appears tied to the glucagon component. The two drugs therefore carry slightly different monitoring emphases: for tirzepatide, attention to biliary symptoms and the thyroid contraindication; for retatrutide, attention to heart rate and blood pressure alongside the shared GI management.
Tirzepatide’s labeled safety considerations
As an approved drug, tirzepatide carries a defined label. It includes a boxed warning for thyroid C-cell tumors, based on rodent data, and it is contraindicated in people with a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2 (MEN2). It also carries warnings around gallbladder and biliary disease, pancreatitis, acute kidney injury from dehydration, and other class effects. These are managed through screening, monitoring, and patient counseling in clinical practice.
Retatrutide’s safety picture is still forming
Retatrutide’s safety profile in phase 2 resembled the incretin class — dose-related GI events dominating — with the additional, distinctive transient heart-rate increase noted above. Because the drug is investigational, it has no approved label, no boxed warnings, and no fully characterized long-term safety record. The larger, longer phase 3 program is where the complete adverse-event picture, including any signals that appear only with scale or time, will be established. Honesty requires stating plainly that retatrutide’s long-term safety is not yet known to the standard applied to an approved medicine.
How do dosing and administration compare?
Both drugs are once-weekly subcutaneous injections given with the same slow-titration philosophy: start at a low dose and step upward over several weeks to a target maintenance dose, allowing the gut to adapt and keeping nausea manageable. This shared cadence means that, from a practical routine standpoint, the two agents feel similar — a weekly injection rotated among standard sites.
The differences are in specifics and status. Tirzepatide has an established, FDA-labeled titration schedule with defined dose steps and maintenance targets. Retatrutide’s dosing in trials also follows a multi-step escalation, but the exact regimen that would reach the market — if it is approved — is not yet finalized, and any figures circulating for retatrutide reflect trial protocols rather than an approved label. For the arithmetic of reconstitution and measurement in a research context, our dosage calculator and reconstitution guide lay out the underlying math; neither should be read as a protocol recommendation.
What are the approval and access realities?
This is the single most important practical distinction, and it deserves to be stated without hedging.
Tirzepatide is approved and obtainable. It is available by prescription in many countries as Mounjaro (diabetes) and Zepbound (weight management). Access is gated mainly by cost, insurance coverage, and periodic supply constraints rather than by regulatory availability. A patient and clinician can start it today if it is appropriate and coverage allows.
Retatrutide is not approved anywhere. Its only legitimate route of access is enrollment in a clinical trial. Material sold outside that channel as “retatrutide” is unregulated, of unverified identity and purity, and outside the safety framework that governs approved medicines. Any research interest in retatrutide should be grounded in this reality: it is an investigational compound whose approval, labeling, and availability are still undetermined and depend on the outcome of ongoing regulatory review.
Who does each drug suit — in a research framing?
Because retatrutide is investigational, the question of “who should use it” cannot be answered clinically; it can only be framed as which mechanistic profile each drug represents. The following is an educational mapping of mechanism to metabolic priority, not a treatment recommendation.
- Where an approved, evidence-dense option is the priority: tirzepatide is the clear reference point. It has phase 3 efficacy, published maintenance data, an established safety label, and real-world availability — the full package that supports actual clinical decisions.
- Where appetite is the dominant driver of weight: the GLP-1/GIP dual mechanism of tirzepatide already addresses appetite and satiety powerfully, and adding a third receptor may offer diminishing marginal benefit for this specific lever.
- Where energy expenditure or hepatic fat is the metabolic bottleneck: retatrutide’s glucagon component is the theoretically relevant addition, and its liver-fat data are its most distinctive feature — but this remains an investigational hypothesis, not an approved use.
- Where the goal is to track the frontier of efficacy: retatrutide’s phase 3 readouts are the data to watch, with the explicit understanding that watching is all that is currently possible outside a trial.
A useful way to hold all of this together is the “metabolic triad” mental model: think of GLP-1 as the appetite brake, GIP as the potentiator that makes the other signals hit harder, and glucagon as the energy-expenditure dial. Tirzepatide turns the first two dials firmly. Retatrutide turns all three. If a given person’s weight is driven mainly by appetite and portion control, the first two dials may already deliver most of the achievable benefit, and the marginal value of the third is uncertain. If the limiting factor is a sluggish metabolic rate or a heavy burden of liver fat, the third dial is exactly the one that theory says should matter — which is why retatrutide’s most striking non-weight result is its effect on hepatic steatosis. The model is a teaching device, not a diagnostic tool, but it captures why two drugs built on the same backbone can be expected to behave somewhat differently.
Will there ever be a direct head-to-head trial?
The honest answer is that no randomized head-to-head trial of retatrutide against tirzepatide has been published, and until one exists, every comparison — including this article — is an inference across separate studies. Direct comparisons do get run in this field; tirzepatide itself was compared head-to-head against semaglutide in a dedicated trial, which is the gold-standard way to settle a superiority question. Whether retatrutide is ultimately studied directly against tirzepatide will depend on regulatory and commercial priorities, but the scientific value of such a trial is obvious, because only a controlled comparison in a single population under a single protocol can convert the current cross-trial impression into an actual finding.
Until then, the intellectually defensible position is calibrated humility. Retatrutide’s numbers are genuinely impressive and its mechanism is genuinely novel, but “impressive numbers in an earlier-stage program” is not the same claim as “proven superiority.” The two statements are often conflated in popular coverage, and keeping them distinct is the single most important habit for reading this comparison accurately. When the full phase 3 record is published and, ideally, a direct comparison is run, the picture will sharpen. For now, tirzepatide is the established, approved reference standard, and retatrutide is the most promising challenger — still investigational, still unproven on the long-term axes that matter most, and worth watching closely.
It is also worth remembering that “which drug is more effective” is not the only axis that decides real outcomes. Tolerability determines who can actually stay on a drug long enough to benefit; access and cost determine who can obtain it at all; and durability determines whether early loss becomes lasting change. A molecule that produces a slightly larger average loss but is harder to tolerate, or unavailable, or unproven over years, does not automatically win on the metrics that matter to a person managing a chronic condition. This is why the comparison cannot be collapsed into a single percentage. The most defensible summary is that tirzepatide is the evidence-complete option available today, and retatrutide is the higher-ceiling candidate whose full value — and full risk profile — will only be known when its phase 3 program is published, scrutinized, and, if warranted, translated into an approval and a label.
What are the key open questions for retatrutide?
Several questions must be answered by the completed, published phase 3 program before retatrutide can be assessed on the same footing as tirzepatide:
- Peer-reviewed phase 3 efficacy and durability. Sponsor topline figures need to become published, scrutinized results, including how weight loss is maintained over the full trial duration.
- Long-term safety at scale. Larger, longer exposure is required to characterize rare adverse events and to clarify the significance of the transient heart-rate increase.
- Cardiovascular outcomes. Dedicated outcome data will determine whether the metabolic improvements translate into hard cardiovascular endpoints.
- Regulatory decisions. Approval status, labeling, contraindications, and any boxed warnings are all still undetermined.
Until those questions are resolved, any comparison that ranks retatrutide above tirzepatide on the basis of a larger phase 2 number is comparing an early signal against an established body of evidence — an apples-to-oranges contrast that the eventual head-to-head or fully published phase 3 data will replace.
How should you evaluate claims about these two drugs?
Because both agents sit at the center of intense marketing and online discussion, it is worth having a disciplined framework for reading any comparison — including this one. The following checklist is an educational tool for weighing evidence, not clinical guidance.
- Confirm the evidence stage. A phase 3 result with thousands of participants and long follow-up carries far more weight than a phase 2 signal or a sponsor press release. Always ask which stage a number comes from.
- Match durations before comparing percentages. A 24% figure at 48 weeks and a 22.5% figure at 72 weeks are not measuring the same thing; the curves are still moving. Never compare endpoints from different time horizons as if they were equivalent.
- Check the estimand. Efficacy-estimand and treatment-regimen-estimand figures differ, sometimes by several percentage points, for the same trial and dose. A quoted number without its estimand is incomplete.
- Separate approved from investigational. Approval is not a formality; it reflects a completed, scrutinized evidence package and a defined safety label. Retatrutide has neither yet.
- Distinguish peer-reviewed from company-reported. Sponsor topline announcements are real but preliminary. Treat them as leading indicators, and wait for the published paper before treating them as settled.
- Weigh durability, not just peak loss. The number that matters for a chronic condition is what is kept off over years, which is a maintenance question, not a peak-effect question.
- Map mechanism to the specific problem. Appetite-dominant weight, hepatic fat, and energy-expenditure limitations are different problems that the GLP-1, glucagon, and GIP levers address differently.
- Discount vendor and forum sources. The most reliable information comes from trial publications and regulatory documents, not from sellers or anecdote.
Applied to the retatrutide-versus-tirzepatide question, this framework produces a consistent conclusion: tirzepatide wins on every axis that depends on completed, published, long-term evidence, while retatrutide leads only on the early-efficacy axis that is still maturing.
What about cost, access, and counterfeit risk?
The practical differences extend well beyond the clinic. Tirzepatide, being approved, moves through the regulated pharmaceutical supply chain: it is manufactured to pharmacopeial standards, dispensed by pharmacies, and (intermittently) subject to shortage but not to questions of authenticity when obtained through legitimate channels. Its main access barriers are price and insurance coverage, which vary widely by country and plan and can be substantial for weight-management use in particular.
Retatrutide has no legitimate commercial supply because it is not approved. That vacuum has been filled by a grey market of material marketed online as “research” retatrutide, and this is a genuine hazard rather than a hypothetical one. Unapproved material carries no guarantee of identity, purity, dose accuracy, or sterility; it is not manufactured under regulated conditions; and it sits entirely outside the safety-monitoring system that catches problems with approved drugs. From an evidence standpoint, nothing about the encouraging trial data transfers to an unregulated vial of unknown provenance, because the trials studied a defined, quality-controlled compound at defined doses under medical supervision. The only responsible framing for retatrutide today is that its legitimate availability is confined to clinical trials, and that everything outside that channel is unverified.
For readers using our site’s educational resources, the arithmetic tools — the dosage calculator, the reconstitution guide, and the individual protocol pages — exist to explain how trial-defined dosing math works, not to endorse acquiring or using an unapproved substance outside a trial.
Frequently Asked Questions
Is retatrutide better than tirzepatide?
On raw weight-loss numbers, retatrutide reached a numerically larger mean reduction (about 24% at 48 weeks in phase 2) than tirzepatide (about 22.5% at 72 weeks in phase 3), and its sponsor-reported phase 3 topline figures are higher still. But retatrutide is investigational and lacks published long-term and maintenance data, while tirzepatide is approved with deep evidence. There has been no head-to-head trial, so “better” depends on whether you weight early efficacy or established, obtainable evidence.
Is tirzepatide a GLP-1 drug?
Tirzepatide is a dual agonist that activates both the GLP-1 receptor and the GIP receptor, so it is more than a pure GLP-1 agent. It is FDA-approved as Mounjaro for type 2 diabetes and as Zepbound for chronic weight management. Its dual mechanism is one reason it produces larger average weight loss than single-target GLP-1 drugs like semaglutide in cross-trial comparisons.
What does the “triple agonist” in retatrutide actually add?
Retatrutide activates the glucagon receptor in addition to the GIP and GLP-1 receptors that tirzepatide targets. Glucagon-receptor agonism is thought to raise energy expenditure and mobilize liver fat, adding an “energy burn” component on top of appetite suppression. The GLP-1 and GIP activity is designed to offset glucagon’s potential to raise blood sugar, so glucose control is preserved in the trials conducted so far.
Why does retatrutide raise heart rate?
In its phase 2 trial, retatrutide produced a transient heart-rate increase that peaked around week 24 and then declined. Heart-rate changes occur across the incretin class, and the glucagon component of retatrutide may contribute. The long-term clinical significance is not yet established and is a specific focus of the ongoing phase 3 and cardiovascular follow-up program.
What are tirzepatide’s main safety concerns?
Tirzepatide carries a boxed warning for thyroid C-cell tumors based on rodent data and is contraindicated in people with a history of medullary thyroid carcinoma or MEN2. It also carries warnings for gallbladder and biliary disease, pancreatitis, and dehydration-related kidney injury. Gastrointestinal side effects such as nausea are common, especially during dose escalation, and are managed with slow titration.
Do you have to stay on these drugs to keep the weight off?
The evidence strongly suggests yes. In the SURMOUNT-4 trial, participants who stopped tirzepatide regained a large share of their lost weight, while those who continued maintained and even extended their loss. This reflects obesity as a chronic condition that requires ongoing management. Retatrutide has no published long-term maintenance data yet, but the same pattern is expected across the class.
When will retatrutide be available?
Retatrutide is investigational and available only through clinical trials. Its sponsor has reported positive phase 3 topline results, but full publication, regulatory submission, and approval decisions are still ahead, and no approval date is guaranteed. Any product sold as retatrutide outside a clinical trial is unregulated and falls outside the safety oversight that governs approved medicines.
How do these two compare with semaglutide?
Semaglutide is a single-target GLP-1 agonist that produced about 14.9% weight loss at 68 weeks in the STEP-1 trial. Tirzepatide’s dual mechanism pushed average weight loss into the low-20s, and retatrutide’s triple mechanism appears in early data to go further still. The progression from GLP-1 to dual to triple agonism illustrates how adding receptor targets has tracked with larger average weight loss across trials.
References
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). N Engl J Med. 2022;387(3):205–216. https://pubmed.ncbi.nlm.nih.gov/35658024/
- Jastreboff AM, Kaplan LM, Frías JP, et al. Triple–Hormone-Receptor Agonist Retatrutide for Obesity — A Phase 2 Trial. N Engl J Med. 2023;389(6):514–526. https://www.nejm.org/doi/full/10.1056/NEJMoa2301972
- Sanyal AJ, Kaplan LM, Frias JP, et al. Triple hormone receptor agonist retatrutide for metabolic dysfunction-associated steatotic liver disease: a randomized phase 2a trial. Nat Med. 2024;30(7):2037–2048. https://www.nature.com/articles/s41591-024-03018-2
- Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP-1). N Engl J Med. 2021;384(11):989–1002. https://www.nejm.org/doi/full/10.1056/NEJMoa2032183
- Aronne LJ, Sattar N, Horn DB, et al. Continued Treatment With Tirzepatide for Maintenance of Weight Reduction in Adults With Obesity: The SURMOUNT-4 Randomized Clinical Trial. JAMA. 2024;331(1):38–48. https://pubmed.ncbi.nlm.nih.gov/38078870/